
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 35; 2023 > Article
- Original Article Association between lone work and self-rated health status: using the 5th Korean Working Conditions Survey
-
Eunseun Han1,2
 , Ui-Jin Kim1,2, Yongho Lee1,2, Sanghyuk Lee1,2, Seunghon Ham1,2,3, Wanhyung Lee1,2,3, Won-Jun Choi1,2,3, Seong-Kyu Kang1,2,3
, Ui-Jin Kim1,2, Yongho Lee1,2, Sanghyuk Lee1,2, Seunghon Ham1,2,3, Wanhyung Lee1,2,3, Won-Jun Choi1,2,3, Seong-Kyu Kang1,2,3 -
Annals of Occupational and Environmental Medicine 2023;35:e29.
DOI: https://doi.org/10.35371/aoem.2023.35.e29
Published online: July 31, 2023
1Department of Occupational and Environmental Medicine, Gil Medical Center, Incheon, Korea.
2Graduate School, Gachon University, Incheon, Korea.
3Department of Occupational and Environmental Medicine, College of Medicine, Gachon University, Incheon, Korea.
- Correspondence: Seong-Kyu Kang. Department of Occupational and Environmental Medicine, College of Medicine, Gachon University, 21 Namdong-daero, 774beon-gil, Namdong-gu, Incheon 21565, Korea. sk.kang@gachon.ac.kr
• Received: January 2, 2023 • Revised: April 27, 2023 • Accepted: June 30, 2023
Copyright © 2023 Korean Society of Occupational & Environmental Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background Lone workers are generally defined as individuals who work alone without supervision, including self-employed people. While lone workers are considered a vulnerable group in some countries, there is a lack of research on their health status in domestic studies. Globally, the number of lone workers has been increasing, and this trend has been further accelerated since the coronavirus disease 2019 (COVID-19) pandemic with the rise of remote work.
-
Methods The study analyzed data from 44,281 participants, excluding unpaid family workers, soldiers, and those with missing data. Lone workers were defined as individuals who reported having no colleagues with the same job at their current workplace. Self-rated health status was categorized as “good” or “poor.”
-
Results This study found a statistically significant higher number of lone workers among women compare to men. The largest occupational category for lone workers was service and sales workers, followed by agriculture and fisheries workers. A majority of non-lone workers reported working 40 hours or less per week, while the majority of lone workers reported working 53 hours or more per week. In addition, lone workers had significantly poorer health status evaluations compared to non-lone workers (odds ratio: 1.297; 95% confidence interval: 1.165–1.444).
-
Conclusions Further research is needed to investigate the causal relationship between lone work and health, using data collected after the COVID-19 pandemic.
BACKGROUND
A lone worker is defined as someone who works without supervision, including those who are self-employed.1 It can also be referred to as ‘isolated workers,’ but it is important ot describe them as ‘lone workers’ to avoid confusion with ‘remote workers.’ The types of lone workers are categorized into three groups: public facing lone workers, mobile lone workers, and fixed-site lone workers.2 According to a study, there are approximately 53 million lone workers in Canada, the USA, and the EU, accounting for about 15 percent of the total workforce. The International Data Corporation estimates that about 1.3 billion people are mobile workers who work alone.3 Lone workers face challenges in dealing with hazard situations because they work without supervisors or colleagues for mutual monitoring.4 In some countries, lone workers are considered vulnerable to health risks. Consequently, guidelines have been implemented to ensure a safe working environment for lone workers in countries such as the UK, Australia, and certain regions of Canada.5,6 Lone workers are exposed to various risks, including sudden illness such as heat stroke and occupational asthma, as well as occupational injuries like vehicle collisions, electrocution, and assaults.7
Due to the prolonged non-face-to-face situations during the coronavirus disease 2019 (COVID-19) epidemic, the number of lone workers, including telecommuters and couriers, has increased.8,9,10 There has been a rise in the number of people involved in non-contact economic activities, such as courier services and delivery platforms. Additionally, in the USA, the proportion of online purchases has exceeded 60%, and consumers’ purchasing behavior has rapidly shifted from offline to online and mobile platforms since the COVID-19 outbreak.11 Delivery agency services are expected to continue growing in the future due to the increased prevalence of non-contact economic activities, the rise in online consumption, and the diversification and advancement of platform.12,13 Even after the end of the COVID-19 pandemic, it is anticipated that the changed lifestyles, such as the increase in online consumption and the development of non-face-to-face work networks, will be sustained, leading to further expansion of lone work.
Self-reported health status is a commonly used indicator in health-related epidemiological investigations. It is associated with physical function, chronic disease prevalence, and mortality. Therefore, it can be serve as a valuable tool for evaluating the health status not only of the general population but also of specific worker groups.13,14 A recent validation study conducted using data from the aging panel study revealed that self-reported health status in the Korean population is a relatively accurate reflection of actual health status.15
While there have been several studies on the safety of lone workers, most of them have focused on the challenges of controlling risks in lone working environments.7,16 It has been difficult to find studies that analyze the health conditions of lone workers, and research specifically on Korean lone workers is scarce. However, lone work is a growing occupational pattern, and there is a significant lack of research on their health issues. Therefore, this study aims to draw attention to the health improvement and management of lone workers by analyzing the self-reported health status of lone workers and non-lone workers using data from the 5th Korean Working Conditions Survey (KWCS), which represents the Korean worker population.
METHODS
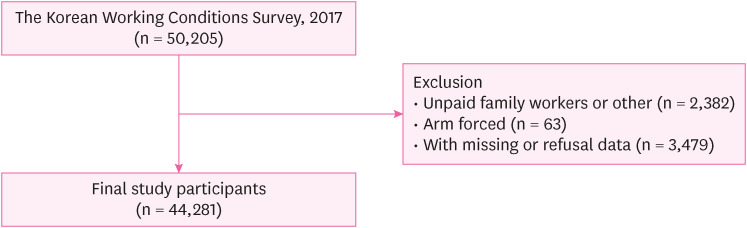
The KWCS is a survey that is based on the European Working Conditions Survey and the Labor Force Survey of the UK. It is conducted under the direction of the Occupational Safety and Health Research Institute in the Korea Occupational Safety and Health Agency. The survey covers various topics such as employment type, occupation and business categories, exposure to risk factors, and employment security. It is a questionnaire-based survey that includes Korean individuals who are 15 years of age or older and are either employees or self-employed at the time of the interview. The survey samples are collected using a multi-stage, random sampling method based on the Population and Housing Census. Participants are required to provide their consent and are assigned random participant numbers to ensure anonymity. In the 5th KWCS, a total of 50,205 participants responded. Among them, 44,281 workers had information on the variables such as gender, age, education, monthly income, employment type, job classification, characteristics of workers in the same job and self-rated health status. It should be noted that the Republic of Korea mandates at least 18 months of mandatory military duty for all male citizens over the age of 18. Therefore, 63 participants who were in the army were excluded from the study due to the lack of heterogeneity in terms of gender and age. Similarly, unpaid family workers were excluded from this study as their characteristics differed from those of general workers, such as not receiving wages and not being considered employees under the Korean Labor Standards Act. The final number of study participants and the exclusion criteria are illustrated in Fig. 1.
A self-reported questionnaire was utilized to evaluate the status of lone working and self-rated health. For the purpose of defining a lone worker, a specific question was chosen: “At your place of work, are there workers with the same job title as you?” Participants who responded with “Nobody else has the same job title” were considered long workers. Participants were asked the following question regarding their perception of health status: “How is your health in general?” They could choose from a 5-point scale (Very Good, Good, Fair, Poor, Very Poor). The responses were categorized into two groups: Poor (“Very Poor” or “Poor”) and Good (“Very Good”, “Good” or “Fair”). Furthermore, the prevalence ratio and 95% confidence interval (CI) for non-lone workers were estimated using the self-rated health status, which was categorized into five groups: Very Poor (1), Poor (2), Normal (3), Good (4), and Very Good (5).
In terms of general factors, the variables considered were sex, age, monthly income and education. Age was categorized into three groups: below 40 years, 40–59 years, and over 60 years. Monthly income was classified as lower than 1 million Korean Won (KRW), 1–2 million KRW, 2–3 million KRW, and 3 million KRW or more. Educational attainment was divided into four groups: less than elementary, junior high, high school, and college or higher.
Regarding occupational factors, the variables included job classification and working hours per week. Job classification was divided into four categories, excluding arm forced; white collar (technicians, experts, and paraprofessionals), pink collar (service workers, sales workers, and clerks), green collar (skilled workers in agriculture, forestry, and fishing), and blue collar (engineers, equipment machine operation and assembly workers, and simple labor workers). Working hours per week were divided into three categories: less than 40 hours, 41–52 hours, and over 53 hours.
For all statistical analyses, we used SAS (version 9.4, SAS institute, NC, USA). χ2 tests were employed to compare different characteristics and occupational factors among lone workers. The relationship between lone working and self-rated health status was analyzed. Multiple logistic regression analyses were performed to calculate odds ratios (ORs) and 95% CIs by adjusting for confounding factors, which were gender, age, education, monthly income, and job classification. Sampling clustering weights were used to calculate weighted percentages and 95% CIs. Survey design weights were determined based on the sampling rate, household survey initiation rate, and household size. Non-response adjustment weights were also applied to address non-response bias, while post-stratification weights were used to reduce bias in estimates, utilizing data from the Employment Trend Survey conducted by the Korea National Statistical Office. The final weight was calculated by multiplying the design weights, non-response adjustment weights, and post-stratification weights. The total sample size, weighted using these weights, was 26,844,999 people, which represents an estimated approximation of the total economically active population in Korea.
The study received approval from the Institutional Review Board of Gil Medical Center, Gachon University, under the reference number GCIRB2021-380.
RESULTS
Table 1 presents a comparison of demographic characteristics between lone workers and non-lone workers. The total number of participants was 44,281, with 36,267 (81.9%) being non-lone workers and 8,014 (18.1%) being lone workers. The results indicate significant differences between non-lone workers and lone workers in terms of sex, age, education, monthly income, working hours per week, job classification, and self-rated health status (p < 0.05). The proportion of women among lone workers was higher than that among non-lone workers. Among the various job classifications, pink collar had the highest proportion of lone workers. There were also differences in educational attainment, with a lower proportion of lone workers having a university or higher degree compared to non-lone workers. In terms of working hours, the majority of non-lone workers worked 40 hours or less per week, whereas the majority of lone workers worked 53 hours or more per week. This suggests that lone workers tend to have longer work hours compared to non-lone workers.
Table 1
Demographic characteristics of the study participants by lone work status (n = 44,281)
The results of the logistic regression analysis, including the compounding and mediating components, are presented in Table 2 as ORs and 95% CIs. These values measure the relationship between lone work and poor health. In Model A, where confounding variables are not modified, working alone was found to be significantly associated with poor health. Descriptively, lone workers had a much higher probability of reporting a poor self-rating of health compared to their non-lone worker counterparts (OR: 2.313; 95% CI: 2.100–2.547). In Model 2, which adjusted for age, sex, education, income, work hours per week and job classification, the relationship between lone workers and poor health was somewhat attenuated but remained statistically significant (OR: 1.297; 95% CI: 1.165–1.444).
Table 2
Results of OR and 95% CI using logistic regression model for Lone work
| Self-rated health status | Lone worker, OR (95% CI) | |||
|---|---|---|---|---|
| Model Aa | Model Bb | |||
| No | Yes | No | Yes | |
| Poor | Reference | 2.313 (2.100–2.547) | Reference | 1.297 (1.165–1.444) |
Table 3 presents the weighted frequency, percentage and rate ratio of self-rated health status for lone workers compared to non-lone workers. Compared to non-lone workers, lone workers were 2.37 times more likely (95% CI: 2.31–2.43) to report their health status as ‘Very Poor’ and 2.06 times more likely (95% CI: 2.05–2.08) to report ‘Poor.’
Table 3
The weighted numbers, percentage and prevalence ratio of self-rated health status
Supplementary Table 1 presents the distribution of lone workers across various industries. The sectors with the highest proportion of lone workers were wholesale and retail trade (29.76%), followed by agriculture, forestry, and fishing (17.39%), and then membership organizations, repair, and other personal services (14.51%).
DISCUSSION
This study aimed to investigate the general characteristics of lone workers in Korea and their self-rated health status. The data presented in Table 1 indicate that the proportion of lone workers in Korea was notably higher among female workers, those with lower levels of education, those working longer hours, and those earning lower monthly incomes. The findings from both Tables 2 and 3 suggest that even after adjusting for potential confounding factors, lone workers remain at a heightened risk of experiencing poor self-rated health compared to non-lone workers. Specifically, lone workers are more likely to rate their health as poor or very poor. Self-rated health status is a reliable indicator of general health, given its correlation with physical function, chronic disease prevalence, and mortality.14,15,17 Thus, the significant association observed between being a lone worker and poor self-rated health status suggests that lone workers face an increased risk of experiencing poor health compared to non-lone workers.
The higher prevalence of chronic diseases such as high blood pressure, diabetes, and hyperlipidemia18,19,20,21 among older female employees, who represent the majority of lone workers, may also contribute to their poorer self-rated health status.
Lone workers are not closely supervised, as they work in isolation from their peers and superiors.22 They can make them more alert and feel pressured about safety compared to other workers.23 Employees who feel overworked or unsafe at work are more likely to experience illness, which can be associated with poor-self rated health.24,25 Moreover, lone workers often lack social support compared to their counterparts, and reduced social support is linked to increased emotional fatigue.26,27 From physiological perspective, mental strain triggers the release of stress hormones and activates the autonomic nervous system, leading to muscle tension. This response is known as the “fight or flight reaction,” which enables a rapid response to life-threatening situations. However, long-term activation of the stress response system due to excessive exposure to stress hormones like cortisol can disrupt normal body processes. This can result in elevated blood pressure, increased blood flow to muscles, and heightened cellular metabolism.28 Conversely, studies have shown that high job satisfaction is associated with organizational support29 and strong relationships with colleagues.30 Job satisfaction can positively affect mental and physical health, and is significantly correlated with self-rated health status.31,32 Additionally, lone workers often work longer hours than traditional office worker.33 Previous research has demonstrated a negative correlation between long working hours and self-rated health status.34 Prolonged working hours can also limit personal time for leisure activities,35 leaving little opportunity for adequate recovery,35 In addition, studies on bus drivers and telecommuters, who are common types of lone workers, have revealed health issues related to nutritional imbalance due to inadequate meals and sedentary lifestyles,36 Long periods of sitting are detrimental to health and are associated with negative lifestyle choices, such as physical inactivity, insufficient sleep, and poor eating habits.37,38,39
The development of the internet has increased the number of people working from anywhere, regardless of geographical distance, and the number of people working alone has also increased.40,41 These workers have increased even more rapidly since the onset of the Corona Pandemics.42 However, the 5th KWCS used in this study differs from the current landscape of lone workers, as it reflects data from 2017, prior to the coronavirus pandemic. Nonetheless, this study can serve as an initial exploration into the potential health effects of lone workers, laying the groundwork for further research in this area.
Since the questionnaire used in the study relies on self-reported information, there is inherent subjectivity, and the characteristics, economic factors, and cultural background of the society can influence the data collection process. This introduces the possibility of non-response or inaccurately answered questions, which can affect the statistics. However, numerous studies have demonstrated that self-rated health is a valid indicator of overall health and a strong predictor of outcomes such as mortality, morbidity, and other health related outcomes. Furthermore, as this study is based on cross-sectional data from the KWCS, there are limitations in establishing temporal precedence or determining a causal relationship between lone work and self-rated health status. The criterion used to distinguish between lone workers and non-lone workers, which is simply based on whether ‘Nobody else has the same job in the workplace,’ does not take into account previous work experience, work type, or years of service. This may result in the health impact of lone work being underestimated. Additionally, there is a lack of data on social and medical records in this study. Social habits such as smoking, alcohol consumption, and caffeine intake have significant impact on health.43 Moreover, the absence of information on specific diseases makes it challenging to determine the relationship between lone workers and the prevalence of actual diseases. Further research focusing on causality or disease prevalence will be necessary. Overall, while this study provides valuable insights, it is important to acknowledge these limitations and encourage future research to address these areas of concern.
According to the employment survey released by Statistics Korea, the number of delivery workers increased by 9.7% compared to the previous year, representing the largest proportion of the economically active population at 1.4%. In addition, the caregiving and health services sector saw a 12% increase in workers compared to the previous ago. The number of telecommuters has experienced significant growth, surging from 95,000 people (0.3% of all employed) in 2019 to 1.14 million people (4.2% of all employed) in 2021. This remarkable increase can be attributed to the implementation of social distancing measures during the pandemic, which necessitated a shift towards telecommuting,44 Although it is anticipated that the number of telecommuters may decrease somewhat after the pandemic, it is expected to remain significantly higher than before the pre-pandemic levels.
CONCLUSIONS
The ongoing changes in lifestyle, such as the increased prevalence of telecommuting or online shopping, are expected to persist even after the end of COVID-19. These trends represent a significant and inevitable shift. The findings in this study indicated that lone workers tend to report poorer self-rated health compared to non-lone workers. This highlights the importance of expanding the focus and attention on lone workers. While this study has certain limitations, it is noteworthy as it is the first to demonstrate the association between lone work and health among Korean workers. It serves as a foundation for addressing the health of lone workers, a population that will continue to grow in the future. Further research is needed to investigate the health effects and accident risks associated with various types of lone work.
ACKNOWLEDGEMENTS
I would like to thank Safety and Health Policy Research Department (Occupational Safety and Health Research Institute, OSHRI) for offering raw-data of KWCS (Korean Working Conditions Survey). The paper’s contents are solely the responsibility of the author and do not necessarily represent the official vies of the OSHRI.
Abbreviations
CI
confidence interval
COVID-19
coronavirus disease 2019
KRW
Korean Won
KWCS
Korean Working Conditions Survey
Ors
odds ratio
-
Competing interests: The authors declare that they have no competing interests.
-
Author Contributions:
Conceptualization: Han ES, Kang SK.
Data curation: Lee SH, Kim UJ, Han ES.
Formal analysis: Han ES, Kim UJ, Lee YH.
Project administration: Kang SK.
Supervision: Kang SK.
Methodology: Lee WH.
Software: Lee WH.
Validation: Ham SH, Choi WJ, Lee WH.
Visualization: Han ES.
Writing - original draft: Han ES.
Writing - review & editing: Lee WH, Kang SK.
NOTES
SUPPLEMENTARY MATERIAL
Supplementary Table 1
The proportion of lone workers according to the Korean standard industrial classification
- 1. Health and Safety Executive. Working Alone: Health and Safety Guidance on the Risks of Lone Working. London, UK: HSE Books; 2009.
- 2. Brennan W. Managing risks to lone workers. Occup Health Wellbeing 2012;64(12):27.
- 3. Myers K. Identifying a Lone Worker: When Lone Doesn’t Mean Alone. Calgary, Canada: Blackline Safety; 2015.
- 4. Yanar B, Lay M, Smith PM. The interplay between supervisor safety support and occupational health and safety vulnerability on work injury. Saf Health Work 2019;10(2):172–179. 31297279.ArticlePubMedPMC
- 5. Government of Western Australia. Guidance Note: Working Alone. Perth, Australia: 2009.
- 6. Canadian Centre for Occupational Health and Safety. Working Alone – General: Osh Answers. Hamilton, Canada: Canadian Centre for Occupational Health and Safety; 2013.
- 7. Straub F. High risk, lone worker: the unacceptable risk. Prof Saf 2018;63(7):30–35. 31007311.PubMedPMC
- 8. Bick A, Blandin A, Mertens K. Work From Home After the COVID-19 Outbreak. Dallas, TX, USA: Federal Reserve Bank of Dallas, Research Department; 2020.
- 9. Narayanan L, Menon S, Plaisent M, Bernard P. Telecommuting: the work anywhere, anyplace, anytime organization in the 21st century. J Mark Manage 2017;8(2):47–54.
- 10. Wolfinbarger M, Gilly MC. Shopping online for freedom, control, and fun. Calif Manage Rev 2001;43(2):34–55.ArticlePDF
- 11. Kim RY. The impact of COVID-19 on consumers: preparing for digital sales. IEEE Eng Manage Rev 2020;48(3):212–218.Article
- 12. Lin C, Lekhawipat W. Factors affecting online repurchase intention. Ind Manage Data Syst 2014;114(4):597–611.Article
- 13. Granger E, Williams G, Di Nardo F, Harrison A, Verma A. The relationship between physical activity and self-rated health status in European adolescents: results of the EURO-URHIS 2 survey. Eur J Public Health 2017;27(Suppl 2):107–111.Article
- 14. Wilson IB, Cleary PD. Linking clinical variables with health-related quality of life. A conceptual model of patient outcomes. JAMA 1995;273(1):59–65. 7996652.ArticlePubMed
- 15. Idler EL. Self-assessed health and mortality: a review of studies. Int Rev Health Psychol 1992;1(1):33–54.
- 16. Brennan W. Safer lone working: assessing the risk to health professionals. Br J Nurs 2010;19(22):1428–1430. 21139525.ArticlePubMed
- 17. Benyamini Y, Idler EL. Community studies reporting association between self-rated health and mortality: additional studies, 1995 to 1998. Res Aging 1999;21(3):392–401.ArticlePDF
- 18. Lewington S, Lacey B, Clarke R, Guo Y, Kong XL, Yang L, et al. The burden of hypertension and associated risk for cardiovascular mortality in China. JAMA Intern Med 2016;176(4):524–532. 26975032.ArticlePubMed
- 19. Bragg F, Holmes MV, Iona A, Guo Y, Du H, Chen Y, et al. Association between diabetes and cause-specific mortality in rural and urban areas of China. JAMA 2017;317(3):280–289. 28114552.ArticlePubMedPMC
- 20. Czerwińska ME, Świerczewska A, Woźniak M, Kiss AK. Bioassay-guided isolation of iridoids and phenylpropanoids from aerial parts of Lamium album and their anti-inflammatory activity in human neutrophils. Planta Med 2017;83(12-13):1011–1019. 28371943.ArticlePubMed
- 21. Peters SA, Woodward M, Jha V, Kennedy S, Norton R. Women’s health: a new global agenda. BMJ Glob Health 2016;1(3):e000080.ArticlePubMedPMC
- 22. Hughes P, Ferrett E. Introduction to Health and Safety at Work. London, UK: Routledge; 2011.
- 23. Barkhordari A, Malmir B, Malakoutikhah M. An analysis of individual and social factors affecting occupational accidents. Saf Health Work 2019;10(2):205–212. 31297283.ArticlePubMedPMC
- 24. Kinman G.. Sickness presenteeism at work: prevalence, costs and management. Br Med Bull 2019;129(1):69–78. 30649219.ArticlePubMed
- 25. Kwon K, Park JB, Lee KJ, Cho YS. Association between Employment Status and Self-Rated Health: Korean working conditions survey. Ann Occup Environ Med 2016;28(1):43. 27617100.ArticlePubMedPMCPDF
- 26. Vander Elst T, Verhoogen R, Sercu M, Van den Broeck A, Baillien E, Godderis L. Not extent of telecommuting, but job characteristics as proximal predictors of work-related well-being. J Occup Environ Med 2017;59(10):e180–e186. 28820860.ArticlePubMed
- 27. Perry SJ, Rubino C, Hunter EM. Stress in remote work: two studies testing the Demand-Control-Person model. Eur J Work Organ Psychol 2018;27(5):577–593.Article
- 28. von Thiele U, Lindfors P, Lundberg U. Self-rated recovery from work stress and allostatic load in women. J Psychosom Res 2006;61(2):237–242. 16880027.ArticlePubMed
- 29. Bentley TA, Teo ST, McLeod L, Tan F, Bosua R, Gloet M. The role of organisational support in teleworker wellbeing: a socio-technical systems approach. Appl Ergon 2016;52:207–215. 26360212.ArticlePubMed
- 30. Fay MJ, Kline SL. Coworker relationships and informal communication in high-intensity telecommuting. J Appl Commun Res 2011;39(2):144–163.Article
- 31. Hills D, Joyce CM. Workplace aggression in clinical medical practice: associations with job satisfaction, life satisfaction and self-rated health. Med J Aust 2014;201(9):535–540. 25358579.ArticlePubMedPDF
- 32. Kroska A. The division of labor in the home: a review and reconceptualization. Soc Psychol Q 1997;60(4):304–322.Article
- 33. Song JT, Lee G, Kwon J, Park JW, Choi H, Lim S. The association between long working hours and self-rated health. Ann Occup Environ Med 2014;26(1):2. 24472333.ArticlePubMedPMCPDF
- 34. Donnelly R, Johns J. Recontextualising remote working and its HRM in the digital economy: an integrated framework for theory and practice. Int J Hum Resour Manage 2021;32(1):84–105.Article
- 35. Jansen N, Kant I, van Amelsvoort L, Nijhuis F, van den Brandt P. Need for recovery from work: evaluating short-term effects of working hours, patterns and schedules. Ergonomics 2003;46(7):664–680. 12745680.ArticlePubMed
- 36. McDonough B, Howard M, Angeles R, Dolovich L, Marzanek-Lefebvre F, Riva JJ, et al. Lone workers attitudes towards their health: views of Ontario truck drivers and their managers. BMC Res Notes 2014;7(1):297. 24886231.ArticlePubMedPMCPDF
- 37. Katzmarzyk PT, Church TS, Craig CL, Bouchard C. Sitting time and mortality from all causes, cardiovascular disease, and cancer. Med Sci Sports Exerc 2009;41(5):998–1005. 19346988.ArticlePubMed
- 38. Patel AV, Bernstein L, Deka A, Feigelson HS, Campbell PT, Gapstur SM, et al. Leisure time spent sitting in relation to total mortality in a prospective cohort of US adults. Am J Epidemiol 2010;172(4):419–429. 20650954.ArticlePubMedPMC
- 39. Dahl S, Kaerlev L, Jensen A, Tüchsen F, Hannerz H, Nielsen PS, et al. Hospitalization for lifestyle related diseases in long haul drivers compared with other truck drivers and the working population at large. Work 2009;33(3):345–353. 19759433.ArticlePubMedPDF
- 40. Gibson CB, Cohen SG. Virtual Teams That Work: Creating Conditions for Virtual Team Effectiveness. Hoboken, NJ, USA: John Wiley & Sons; 2003.
- 41. Wheatley D. Workplace location and the quality of work: the case of urban-based workers in the UK. Urban Stud 2021;58(11):2233–2257.ArticlePDF
- 42. Carroll N, Conboy K. Normalising the “new normal”: changing tech-driven work practices under pandemic time pressure. Int J Inf Manage 2020;55:102186. 32836643.ArticlePubMedPMC
- 43. Ekpanyaskul C, Padungtod C. Occupational health problems and lifestyle changes among novice working-from-home workers amid the COVID-19 pandemic. Saf Health Work 2021;12(3):384–389. 33747597.ArticlePubMedPMC
- 44. Statistics Korea. Industry and occupational characteristics of employed workers in the first half of 2021 local area employment survey. Updated 2021]. https://kostat.go.kr/board.es?mid=a10301030300&bid=211&act=view&list_no=414646 .
REFERENCES
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Workplace support, wellbeing and intention to leave among lone working healthcare assistants providing palliative and end-of-life care in the community: A mixed methods study
Katarzyna A. Patynowska, Emma Maun, Erin Raquel Fantoni, Tracey McConnell, Anne Finucane, Jonathan Clemo, Epiphany Leone, Natasha Wynne, Colette McAtamney, Felicity Hasson
Palliative Medicine.2026; 40(2): 194. CrossRef - Association between occupational exposure, musculoskeletal disorders, occupational depression, and workplace violence in Korean workers: a nationwide large-scale study
Shiva Raj Acharya, Jeevan Bhatta, Rajitha Kawshalya Mailan Arachchige Don
Global Health Journal.2026; 10(1): 26. CrossRef - No Worker is an Island: Physical and Social Isolation at Work in the United States
Kenneth A. Scott, Chandran Achutan, Ryan Hill
Journal of Occupational & Environmental Medicine.2026; 68(6): 465. CrossRef - Association Between Precarious Employment and Cognitive Decline: A Longitudinal Study of Middle-Aged and Older Workers in Korea
Seong-Uk Baek, Jin-Ha Yoon
Journal of General Internal Medicine.2025; 40(10): 2292. CrossRef - Impact of Changes in Type of Employment on Absenteeism/Presenteeism Among Korean Workers
Yunjun Park, Wanhyung Lee
Journal of Occupational & Environmental Medicine.2025; 67(11): e807. CrossRef - Association between single-person household wage workers in South Korea and insomnia symptoms: the 6th Korean Working Conditions Survey (KWCS)
Yoon Ho Lee, Yong-Jin Lee, Eun-Chul Jang, Young-Sun Min, Soon-Chan Kwon
Ann Occup Environ Med.2024; 36: e25. CrossRef
 Cite
Cite- Figure
-
- Related articles
-
- Association between working ≥10 hours per day and satisfaction with work environment among wage workers in Korea: a cross-sectional study using data from the 7th Korean Working Conditions Survey
- Association between sudden work recall and psychological health issues: a cross-sectional analysis of the 6th Korean Working Conditions Survey
- Health effects of weekend work on Korean workers: based on the 6th Korean Working Conditions Survey
- Association between multiple jobs and physical and psychological symptoms among the Korean working population
- Occupation classification model based on DistilKoBERT: using the 5th and 6th Korean Working Condition Surveys
Association between lone work and self-rated health status: using the 5th Korean Working Conditions Survey
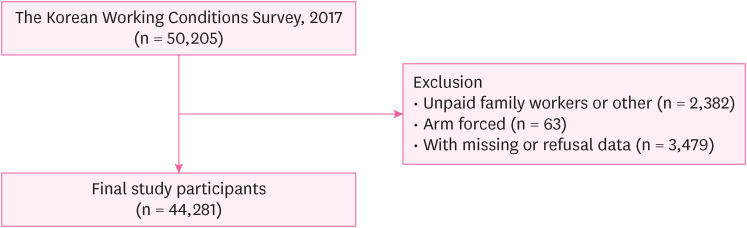
Fig. 1 Schematic diagram depicting study population.
Fig. 1
Association between lone work and self-rated health status: using the 5th Korean Working Conditions Survey
| Variables | Total participants | Non-lone worker | Lone worker | |||||
|---|---|---|---|---|---|---|---|---|
| No. | % | No. | %(col) | No. | %(col) | |||
| Total subjects | 44,281 | 100.00 | 36,267 | 81.9 | 8,014 | 18.1 | ||
| Sex | < 0.0001 | |||||||
| Men | 21,666 | 48.93 | 18,238 | 50.29 | 3,428 | 42.78 | ||
| Women | 22,615 | 51.07 | 18,029 | 49.71 | 4,586 | 57.22 | ||
| Age | < 0.0001 | |||||||
| 15–39 | 11,945 | 26.98 | 11,024 | 30.4 | 921 | 11.49 | ||
| 40–59 | 22,285 | 50.33 | 18,186 | 50.14 | 4,099 | 51.15 | ||
| ≥ 60 | 10,051 | 22.7 | 7,057 | 19.46 | 2,994 | 37.36 | ||
| Education | < 0.0001 | |||||||
| Elementary school (below 6 years) | 3,968 | 8.96 | 2,653 | 7.32 | 1,315 | 16.41 | ||
| Junior high school (7–9 years) | 3,843 | 8.68 | 2,847 | 7.85 | 996 | 12.43 | ||
| High school (10–12 years) | 16,979 | 38.34 | 13,340 | 36.78 | 3,639 | 45.41 | ||
| University (13 years and above) | 19,491 | 44.02 | 17,427 | 48.05 | 2,064 | 25.75 | ||
| Monthly income (\xef\xbf\xa610,000) | < 0.0001 | |||||||
| 0–99 | 6,302 | 14.23 | 4,612 | 12.72 | 1,690 | 21.09 | ||
| 100–199 | 15,169 | 34.26 | 12,419 | 34.24 | 2,750 | 34.31 | ||
| 200–299 | 12,377 | 27.95 | 10,257 | 28.28 | 2,120 | 26.45 | ||
| ≥ 300 | 10,433 | 23.56 | 8,979 | 24.76 | 1,454 | 18.14 | ||
| Working hours per week | < 0.0001 | |||||||
| 40 hours or less | 21,191 | 47.86 | 18,773 | 51.76 | 2,418 | 30.17 | ||
| 41–52 hours | 11,816 | 26.68 | 9,864 | 27.2 | 1,952 | 24.36 | ||
| 53 hours or more | 11,274 | 25.4 | 7,630 | 21.04 | 3,644 | 45.47 | ||
| Job classificationa | < 0.0001 | |||||||
| White | 12,569 | 28.38 | 11,745 | 32.38 | 824 | 10.28 | ||
| Pink | 17,242 | 38.94 | 12,859 | 35.46 | 4,383 | 54.69 | ||
| Green | 3,136 | 7.08 | 1,980 | 5.46 | 1,156 | 14.42 | ||
| Blue | 11,334 | 25.6 | 9,683 | 26.7 | 1,651 | 20.60 | ||
| Self-rated health status | < 0.0001 | |||||||
| Good | 42,266 | 95.45 | 34,912 | 96.26 | 7,354 | 91.76 | ||
| Poor | 2,015 | 4.55 | 1,355 | 3.74 | 660 | 8.24 | ||
| Self-rated health status | Lone worker, OR (95% CI) | |||
|---|---|---|---|---|
| Model Aa | Model Bb | |||
| No | Yes | No | Yes | |
| Poor | Reference | 2.313 (2.100–2.547) | Reference | 1.297 (1.165–1.444) |
| Self-rated health status | Non-lone worker | Lone worker | Prevalence ratioc | 95% confidence interval | ||
|---|---|---|---|---|---|---|
| No.a | %b | No.a | %b | |||
| Very good | 2,657,379 | 12.45 | 207,066 | 8.33 | 0.67 | 0.66–0.67 |
| Good | 13,402,236 | 62.77 | 1,414,603 | 56.92 | 0.91 | 0.91–0.91 |
| Fair | 4,803,687 | 22.50 | 745,501 | 30.00 | 1.33 | 1.33–1.34 |
| Poor | 459,343 | 2.15 | 110,373 | 4.44 | 2.06 | 2.05–2.08 |
| Very poor | 27,695 | 0.13 | 7,639 | 0.31 | 2.37 | 2.31–2.43 |
Table 1 Demographic characteristics of the study participants by lone work status (n = 44,281)
aWhite collar: technicians, experts and paraprofessionals; pink collar: service, sales workers and clerical support; green collar: skilled workers in agriculture, forestry, and fishing; blue collar; engineers, equipment machine operation and assembly workers, simple labor workers.
Table 2 Results of OR and 95% CI using logistic regression model for Lone work
OR: odds ratio; CI: confidence interval.
aModel A is not adjusted for confounding variables; bModel B is adjusted age, sex, education, income, work hours, and job classification.
Table 3 The weighted numbers, percentage and prevalence ratio of self-rated health status
aWeighted numbers, bWeighted percentage, cPrevalence ratio = rate ratio of self-rated health status of the lone workers versus the non-lone workers.

