Abstract
-
Background
Female farmers have a high prevalence of knee osteoarthritis (KOA) in South Korea. Femoral bowing has been reported to be related to KOA by increasing load on the mechanical axis. This study aimed to investigate factors related to femoral bowing in Korean female farmers.
-
Methods
We analyzed the legs of 264 female farmers registered with the Korea farmers' knee cohort of Jeonnam Center for Farmers' Safety and Health. A structured questionnaire was used to determine sociodemographic variables, agricultural career, cumulative squatting working time (CSWT), and cumulative heavy lifting working time. Femoral bone density was measured and Kellgren-Lawrence (KL) grades were obtained from the knee radiographs. Mechanical axis angle (MAA), femoral bowing angle (FBA), anatomical lateral distal femoral angle (aLDFA), anatomical medial proximal tibial angle (aMPTA), and condylar-plateau angle (CPA) were measured. We examined the relationship between the FBA and related factors by using multiple linear regression.
-
Results
The proportion of individuals with radiographic KOA (≥ KL grade 2) in this study was 37.9%. As KL grades increased, MAA, FBA, and CPA increased, whereas aLDFA and aMPTA decreased. FBA increased with age. Multiple linear regression analyses using FBA as a dependent variable showed relationship with higher age, lower height, higher BMI, lower bone mineral density, longer CSWT, and longer agricultural careers.
-
Conclusions
The results of this study suggest that external factors related to agricultural work in female farmers was associated with femoral bowing, in addition to internal factors such as age, bone density, height, and obesity.
-
Keywords: Knee; Osteoarthritis; Females; Farmers; Bone density; Femur; Genu varum
BACKGROUND
Osteoarthritis is a chronic degenerative disorder that causes anatomic and physiologic derangement. Its global prevalence is increasing and is expected to increase continuously [
1]. Osteoarthritis is a significant economic burden for individuals and is often a cause of ‘catastrophic health expenditure’ as defined by the World Health Organization [
2]. Knee osteoarthritis (KOA) is significant, in comparison to arthritis affecting other joints, as it affects ambulation and social function [
3,
4]. Females have a higher prevalence of osteoarthritis than males [
5]. This trend was seen in the fifth Korea National Health and Nutrition Examination Survey, which estimated that 26.7% of men and 47.3% of women have radiographic KOA. The rate of total knee arthroplasties has increased steadily from 2001 to 2010 in both sexes and the proportion of female patients has been steady at approximately 90% [
6]. Female farmers in South Korea have a higher prevalence than females in other occupations [
7]. The high prevalence is thought to be due to occupational factors, such as squatting, climbing, and lifting in addition to the biological vulnerability of women [
8,
9]. Various hypotheses have been suggested for the high prevalence of KOA in women [
10,
11,
12]. The malalignment of lower extremities as intrinsic factors of KOA is critical because it fails to distribute weight evenly [
13,
14,
15]. Varus deformity is the result of bone deformation with age and progressive KOA [
15,
16,
17]. The purpose of this study was to examine the epidemiological characteristics of lower limb alignment in female farmers and to determine whether squatting or physical burden might contribute to the change of lower limb alignment in female farmers. In particular, the coronal femoral bowing angle (FBA) has recently been noted as the major contributing factor to the mechanical axis angle (MAA) in females [
18,
19,
20,
21,
22]. Some researchers have hypothesized that the FBA is associated with the progression of KOA [
23,
24]. Therefore, we analyzed the characteristics of femoral deformation in Korean female farmers. We also identified the external and internal factors associated with the FBA.
METHODS
Participants
This cross-sectional study enrolled farmers registered with the Korea farmers' knee cohort (KFKC). This cohort consists of farmers from 16 districts in Jeonnam province, South Korea. We analyzed 528 knees of 264 women from this cohort aged 40–79 years, between 2013 and 2015. The subjects who underwent arthroplasty were excluded from the screening process in the KFKC because the KFKC is a magnetic resonance imaging-based cohort.
Related variables
Researchers obtained information on sex and age, physical profiles such as height and body mass index (BMI), working time and length of farming career, using the structured questionnaire. They obtained the bone mineral density measures and knee radiographs (weight-bearing whole leg anteroposterior view) from the KFKC database. To measure how much time the farmers spent working in a specific position (squatting or lifting), we took the unit task exposure as the median value of each sub-periods exposure and then defined cumulative squatting working time (CSWT) and cumulative heavy lifting working time (CLWT) by the following formula: cumulative working time (hours) = working years for lifetime × working months per year × 4 weeks × working days per week × working hours per day. However, right-skewed distribution was found in the initial analysis of CSWT and CLWT, so we converted the value of these variables into quartiles (4Q) for regression analysis. The bone marrow density data in the KFKC database were the sets of values measured at the lumbar spine (L1 to L4) and femoral neck. However, for this study, we used the value of femur bone mineral density (BMD[f]).
Radiographic measurements
The Kellgren-Lawrence (KL) grade was used to determine the stage of KOA [
25]. Two experienced physicians read the images taken with standardized weight-bearing for anteroposterior and Rosenburg view. We used an atlas from the Osteoarthritis Research Society International to increase the reliability of the readings [
26], and 4 mm was applied as the cut-off point for joint space narrowing, based on the International Knee Documentation Committee [
25,
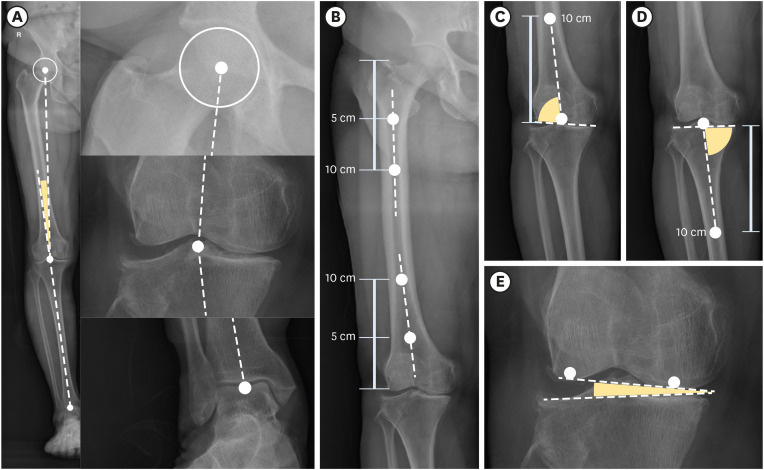
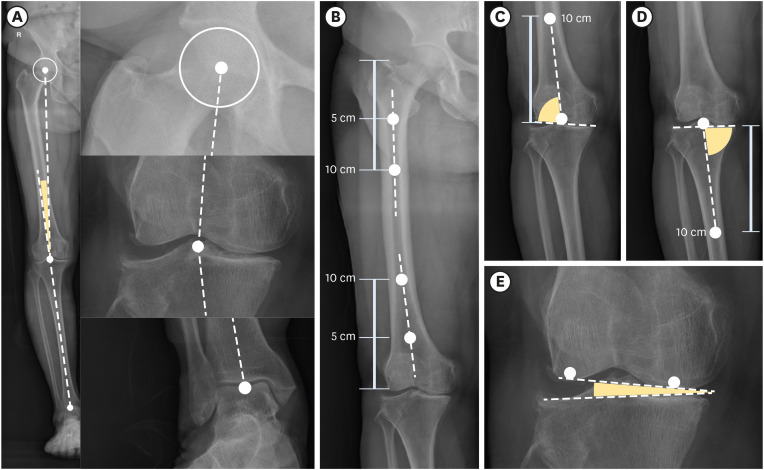
27]. The MAA was defined as the angle between one line connecting the center of the femoral head with the middle of the knee (midpoint of the tibial spine) and another line connecting the middle of the surface of the talus with the middle of the knee [
28]. The FBA was defined as an acute angle formed between the line drawn at the center of the femur below the level of the lesser trochanter passing through the center of the femur at a point 5 cm distal to the starting point and the line extending from the center of the femoral distal condyle through the center of the femur at a 5 cm proximal portion and a 5 cm further proximal point. The lateral FBA was expressed as a positive value [
29]. The anatomical lateral distal femoral angle (aLDFA) was the angle between the anatomical axis of the femur and the tangent to the subchondral plate of the femoral condyle. The anatomical medial proximal tibial angle (aMPTA) was the angle between the tangent to the subchondral plate of the tibia and the anatomical axis of the tibia [
30]. The measuring point for the anatomical shaft axis was 10 cm away from the joint surface. The condylar plateau angle (CPA) was the angle between the tangents to the subchondral plates of the femoral and tibial condyles (
Fig. 1) [
31].
Fig. 1
Measurement of MAA and lower limb angles. (A) MAA, (B) femoral bowing angle, (C) anatomical lateral distal femoral angle, (D) anatomical medial tibial angle, (E) condylar plateau angle.
MAA: mechanical axis angle.
Reliability of radiologic measurement
We calculated intraclass correlation coefficients (ICC) for interobserver reliability. The ICC of MAA was excellent (ICC 0.981) and the ICC of FBA and CPA was good (0.809 and 0.842 respectively). The ICCs of aLDFA and aMPTA, however, were moderate, at 0.561 and 0.695 respectively. The Kappa of the KL grade by 2 readers was moderate (kappa 0.581). The value measured by the more experienced reader was selected, and when the difference between the measured values was large, the re-measured value was used.
Statistical analysis
We performed 1-way analysis of variance and post hoc analysis by Scheffé's test to compare the mean values of the lower limb angles according to the KL grade group. The linear regression analysis with MAA as the dependent variable and FBA, aLDFA, CPA, and aMPTA as independent variables applied for estimating the contribution of lower limb angles for MAA. The relationship between the variables was obtained by Pearson's correlation analysis. To evaluate the association between the FBA and related factors, a linear regression analysis was performed with 2 models, to reduce the problem of multicollinearity. Model 1 included internal factors such as age, height, BMI, and BMD(f), and agricultural work-related external factors such as CSWT and CLWT. In model 2, CSWT, and CLWT were replaced by agricultural career All statistical analyses were performed using IBM SPSS version 21.0 (IBM Corp., Armonk, NY, USA). A p-value of < 0.05 was considered statistically significant.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Chosun University Hospital (approval No. 2013-12-006). Informed consent was submitted by all subjects when they were enrolled. All participants provided written informed consent for both the participation in the survey and the use of their data for research purposes.
RESULTS
General characteristics
The average age of the study participants was 57.27 years (± 8.19). The average height was 155.57 (± 6.36) cm, and the average weight was 59.01 (± 9.08) kg. The average BMI and BMD(f) were 24.31 kg/m
2 (± 3.15) and 0.92 g/cm
2 (± 0.14), respectively. The average duration of agricultural career was 27.05 years (± 15.21). The average CSWT was 25.03 thousand hours, with a skewness of 0.893. The average CLWT was 21.23 thousand hours, with a skewness of 1.495 (
Table 1).
Table 1General characteristics
|
Variables |
No. |
Minimum |
Maximum |
Mean |
SD |
Skewness |
|
Age (years) |
264 |
40.00 |
77.00 |
57.27 |
8.19 |
0.238 |
|
Height (cm) |
264 |
125.10 |
189.20 |
155.57 |
6.36 |
0.064 |
|
Weight (kg) |
264 |
36.00 |
84.10 |
59.01 |
9.08 |
0.270 |
|
BMI (kg/m2) |
264 |
16.64 |
33.49 |
24.34 |
3.15 |
0.363 |
|
BMD(f) (g/cm2) |
264 |
0.45 |
1.31 |
0.92 |
0.14 |
−0.099 |
|
Career (years) |
264 |
0.50 |
60.00 |
27.05 |
15.21 |
0.143 |
|
CSWT (1,000 hours) |
264 |
0.00 |
94.08 |
25.76 |
25.03 |
0.893 |
|
Quartile 1 |
43 |
0.00 |
1.41 |
0.41 |
|
Quartile 2 |
63 |
1.54 |
11.48 |
5.46 |
|
Quartile 3 |
78 |
11.95 |
34.50 |
22.76 |
|
Quartile 4 |
80 |
34.78 |
94.08 |
58.29 |
|
CLWT (1,000 hours) |
264 |
0.00 |
94.08 |
16.74 |
21.23 |
1.495 |
|
Quartile 1 |
75 |
0.00 |
1.04 |
0.27 |
|
Quartile 2 |
55 |
1.07 |
7.20 |
3.29 |
|
Quartile 3 |
68 |
7.31 |
25.62 |
14.79 |
|
Quartile 4 |
66 |
27.32 |
94.08 |
48.67 |
Comparison of the means of the lower limb angles by severity of ROA
Table 2 shows the comparison of the mean values of the lower limb angles according to the KL grade. As KL grade increased, MAA, FBA, and CPA increased significantly, whereas aLDFA and aMPFA decreased significantly. In post hoc tests, MAA, FBA, and aLDFA were divided into KL grades 0–2 and 3–4. In contrast, CPA showed significant differences in KL grades 0–1, grade 2, and grades 3–4, respectively.
Table 2Comparison of means of lower limb angles according to KL grade group
|
Variables |
KL grade |
No. |
Mean (degree) |
SD |
p-value |
Homogenous subset by post hoc analysis |
|
MAA |
Grade 0–1 |
328 |
2.52 |
2.72 |
< 0.001 |
1 |
|
Grade 2 |
143 |
2.95 |
3.11 |
1 |
|
Grade 3–4 |
57 |
8.15 |
5.06 |
2 |
|
Total |
528 |
3.25 |
3.59 |
|
|
FBA |
Grade 0–1 |
328 |
1.05 |
4.60 |
< 0.001 |
1 |
|
Grade 2 |
143 |
1.66 |
4.11 |
1 |
|
Grade 3–4 |
57 |
5.97 |
5.02 |
2 |
|
Total |
528 |
1.75 |
4.75 |
|
|
aLDFA |
Grade 0–1 |
328 |
85.13 |
2.83 |
< 0.001 |
1 |
|
Grade 2 |
143 |
84.49 |
3.14 |
1 |
|
Grade 3–4 |
57 |
82.72 |
2.77 |
2 |
|
Total |
528 |
84.69 |
3.00 |
|
|
CPA |
Grade 0–1 |
328 |
1.43 |
1.02 |
< 0.001 |
1 |
|
Grade 2 |
143 |
1.86 |
1.26 |
2 |
|
Grade 3–4 |
57 |
3.42 |
2.09 |
3 |
|
Total |
528 |
1.76 |
1.38 |
|
|
aMPTA |
Grade 0–1 |
328 |
92.79 |
4.84 |
0.034 |
1 |
|
Grade 2 |
143 |
93.07 |
1.78 |
1/2 |
|
Grade 3–4 |
57 |
94.31 |
3.09 |
2 |
|
Total |
528 |
93.03 |
4.08 |
|
The correlation between the lower limb angles
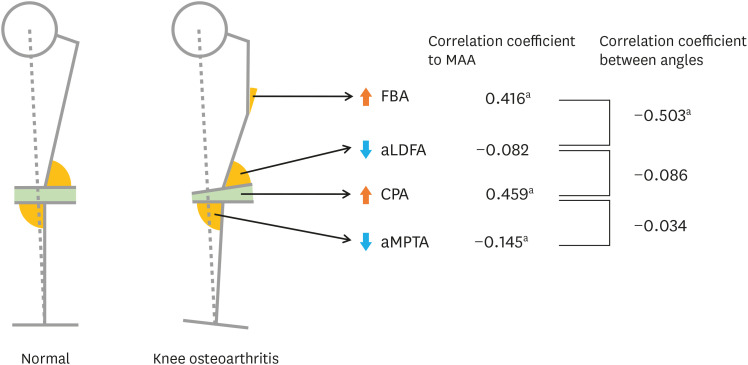
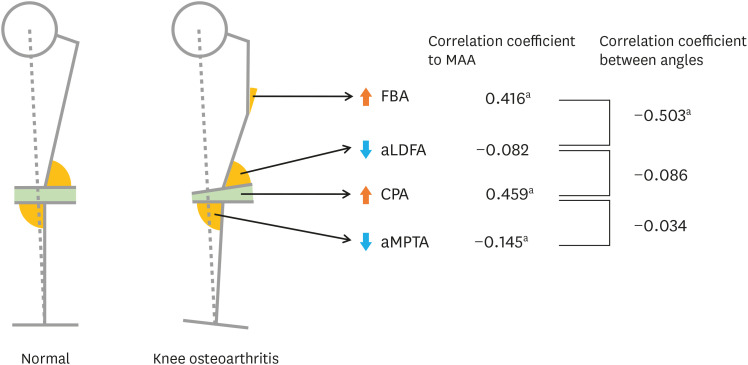
Table 3 shows the association between the variables through Pearson's correlation analysis. The variables highly correlated with age were the agricultural career (correlation coefficient [r] = 0.595), BMD(f) (r = 0.464), FBA (r = 0.424), MMA (r = 0.348), aLDFA (r = −0.372), CSWT (r = 0.307), and CPA (r = 0.269). Agricultural career was correlated with CSWT (r = 0.543) and CLWT (r = 0.251). CLWT and CSWT were also correlated (r = 0.555). MAA showed a significant positive correlation with FBA (r = 0.416) and CPA (r = 0.459), whereas aLDFA had no correlation and aMPTA had a significant negative correlation (r = −0.145). FBA showed a significant negative correlation with aLDFA (r = −0.503) and a significant positive correlation with CPA (r = 0.171) (
Fig. 2).
Table 3The correlation coefficient between factors
|
Variables |
Age |
Career |
CSWT |
CLWT |
BMI |
BMD(f) |
MAA |
FBA |
aLDFA |
CPA |
|
Career |
0.595b
|
|
|
|
|
|
|
|
|
|
|
CSWT |
0.307b
|
0.543b
|
|
|
|
|
|
|
|
|
|
CLWT |
0.021 |
0.251b
|
0.555b
|
|
|
|
|
|
|
|
|
BMI |
−0.144b
|
−0.062 |
−0.013 |
0.055 |
|
|
|
|
|
|
|
BMD(f) |
−0.464b
|
−0.275b
|
−0.205b
|
−0.016 |
0.397b
|
|
|
|
|
|
|
MAA |
0.348b
|
0.362b
|
0.163b
|
0.055 |
0.132b
|
−0.161b
|
|
|
|
|
|
FBA |
0.424b
|
0.419b
|
0.207b
|
0.020 |
0.021 |
−0.279b
|
0.416b
|
|
|
|
|
aLDFA |
−0.372b
|
−0.280b
|
−0.192b
|
−0.034 |
−0.110 |
0.184b
|
−0.082 |
−0.503b
|
|
|
|
CPA |
0.269b
|
0.276b
|
0.175b
|
0.051 |
0.063 |
−0.100a
|
0.459b
|
0.171b
|
−0.086a
|
|
|
aMPTA |
0.033 |
0.041 |
0.027 |
0.005 |
0.077 |
−0.045 |
−0.145b
|
−0.020 |
0.128b
|
0.034 |
Fig. 2
The change of lower limb angles from normal to knee osteoarthritis.
MAA: mechanical axis angle; FBA: femoral bowing angle; aLDFA: anatomical lateral distal femoral angle; CPA: condylar-plateau angle (joint space narrowing); aMPTA: anatomical medial proximal tibial angle.
ap < 0.01 by Pearson's correlation analysis.
Factors associated with the FBA
Table 4 shows the result of multiple linear regression analysis using FBA as a dependent variable. In model 1, FBA was positively correlated with increase in age, BMI, and CSWT. On the other hand, as the values of height, BMD(f), and CLWT (4Q) increased, FBA significantly decreased. In model 2, FBA was positively correlated with increase in age, BMI, and career. Likewise, as the height, BMD(f) and CLWT (4Q) increased, FBA significantly decreased. In model 1, the standardized coefficient beta (β*) was in order of age (β* = 0.27), height (β* = −0.21), and CSWT (β* = 0.13). However, in model 2, the standardized beta was in order of agricultural career (β* = 0.23), height (β* = −0.19), and age (β* = 0.17).
Table 4The related factors of femoral bowing angle by multiple linear regression
|
Model |
Variables |
Coefficients |
p-value |
R2
|
|
β (95% CI) |
β*
|
|
1 |
Intercept |
16.49 (5.11, 27.87) |
|
0.005 |
0.26 |
|
Internal factors |
Age (year) |
0.16 (0.10, 0.21) |
0.27 |
< 0.001 |
|
Height (cm) |
−0.16 (−0.22, −0.10) |
−0.21 |
< 0.001 |
|
BMI (kg/m2) |
0.18 (0.06, 0.30) |
0.12 |
0.005 |
|
BMD(f) (g/cm2) |
−3.93 (−6.98, −0.87) |
−0.12 |
0.012 |
|
External factors |
CSWT (4Q) |
0.58 (0.18, 0.97) |
0.13 |
0.005 |
|
CLWT (4Q) |
−0.46 (−0.81, −0.10) |
−0.11 |
0.012 |
|
2 |
Intercept |
15.73 (4.63, 26.83) |
|
0.006 |
0.28 |
|
Internal factors |
Age (year) |
0.10 (0.04, 0.16) |
0.17 |
0.001 |
|
Height (cm) |
−0.14 (−0.20, −0.08) |
−0.19 |
< 0.001 |
|
BMI (kg/m2) |
0.18 (0.06, 0.30) |
0.12 |
0.004 |
|
BMD(f) (g/cm2) |
−4.22 (−7.22, −1.23) |
−0.13 |
0.006 |
|
External factors |
Career (year) |
0.07 (0.04, 0.10) |
0.23 |
< 0.001 |
DISCUSSION
It is well known that the CPA is associated with KOA [
32], and this has been confirmed in our study. A higher CPA indicates that the medial tibiofemoral joint space is reduced compared to the lateral side. Therefore, medial compartment osteoarthritis leads to an increase in the CPA. In our study, age and BMI were related to the CPA, as in previous studies [
18,
23,
24].
In our study, we identified a significant association between the FBA and internal factors such as age, height, BMI, and BMD(f). In particular, we found an association of the FBA with occupational external factors such as prolonged squatting posture or agricultural career in Korean female farmers after the adjustment for known confounders. These results suggest that femoral bowing observed in female farmers is related to agricultural work.
The results of our study show that the FBA increases with age. However, an additional analysis comparing both sexes showed that this phenomenon only occurred in female farmers. The association between the FBA and age was similar, although subjects were limited to only persons with radiologic KOA. Interestingly, in female farmers without radiologic KOA, the FBA increased with age (
Supplementary Table 1). In interpreting these phenomena, Matsumoto et al.'s [
23] almost unique population-based study has become an important comparison with ours. They conducted a cross-sectional study comparing limb alignment between normal volunteers and KOA patients who visited Kobe university in Japan. They also found that the femoral shaft bowed medially with age. However, the relationship between age and the FBA in normal people did not show a significant difference between males and females. The increase in the FBA was more prominent in females than in males in KOA patients [
23]. This difference is presumed to be due to the different characteristics of the study subjects. Matsumoto et al.'s [
23] subjects were recruited by voluntary participation from the community, but our research subjects were limited to agricultural workers.
Several studies have shown that the FBA of patients with KOA is larger than that of the normal control group [
24,
29,
33,
34,
35,
36,
37]. These results have been reported mainly in hospital-based studies. Matsumoto et al. [
23] noted the possibility that an increase in the FBA triggers or worsens KOA. They showed that the mean FBA among females with mild KOA was 1.4 ± 3.1, but the mean FBA among profound KOA patients was 5.9 ± 3.2 [
23]. In addition, the FBA increased with the severity of KOA. Yau et al. [
37] suggested that femoral bowing was common in a Chinese population with end-stage KOA.
Our study showed the higher the BMD and height, the lower the FBA. Shimosawa et al. [
24] also showed similar results. Rickets and osteomalacia induced by poor dietary intake of vitamin D, present with bowing of the legs. In particular, vitamin D is related to the growth hormone/insulin-like growth factor 1 axis in childhood [
38]. Therefore, vitamin D or nutritional deficiency in childhood is a shared factor with lower peak bone density and lower height. Although the relationship between age and FBA is not clear, it is assumed that factors such as malnutrition and menopause have been mediated. Our study did not investigate vitamin D deficiency, but there is sufficient evidence that vitamin D deficiency causes low BMD. Insufficient daily calcium and vitamin D intake is common in Korean postmenopausal women [
39]. The softened bones of females with osteomalacia can lead to bowing, especially in the weight-bearing bones of the legs [
40].
In addition to confirming this fact, our study identified which external factors cause FBA in vulnerable women. Our conclusion is that prolonged squatting increases FBA, and heavy lifting decreases FBA. The squatting position of Korean female farmers, called Asian squat, is a deep squatting posture with spreading between both knees and contact between the thighs and calves [
41]. This posture applies force perpendicular to the proximal femur, whereas, heavy lifting in the standing position puts load along the axis of the long bones. In addition, heavy lifting is a resistance exercise that improves lower extremity muscles, and thus has a positive effect on bone density [
42]. Shin et al. [
20] showed the association between atypical femoral fractures with femoral bowing and loss of thigh muscle. These results support the conclusion that lifting maintains or strengthens muscles and can be a protective factor against femoral bowing.
Agricultural career was significantly related to the FBA even after adjusting age. In model 1, the standardized beta of age was the largest, at 0.27. In model 2, the standardized beta of age was reduced to 0.17 and the standardized beta of the agricultural career was the largest, at 0.23. This suggests that there may be external factors related to agricultural work that are not explained by CSWT and CLWT.
Interestingly, our study showed a clear negative correlation between the FBA and aLDFA (r = −0.503). FBA and aMPTA showed no correlation. As mentioned earlier, FBA has a positive correlation with the severity of KOA. According to a study by Matsumoto et al. [
23], The severity of KOA and aLDFA have a positive correlation. This trend was also confirmed in our study. Although both FBA and aLDFA are related to the severity of radiologic KOA, it is unusual to have an inverse correlation between FBA and aLDFA. However, this result was also reproduced in the study by Lu et al. [
33].
The femur is a long bone, while the femur condyle is a relatively wide and thick bone. Thus, when bone deformation is caused by external or internal factors, the femur's deformation will be greater than that of the condyle. We thus interpreted that as the FBA increased, aLDFA, the angle between the femur shaft and the femur condyle, also increased.
This study has the following limitations. First, since participants are female farmers living in a rural society, the results cannot be generalized to males, urban residents, and other occupational groups. Second, CLWT and CSWT were insufficient to verify reliability and validity. The CLWT and CSWT had a bimodal and right-skewed distribution, we, therefore, categorized the cumulative working times into 4Q. Third, survival bias is possible because people with knee arthroplasty were excluded from the study. Fourth, calcium or vitamin D intake, underlying diseases, medication use, dietary habits, menopause state, and housework were not identified as factors affecting femoral bowing.
Nevertheless, the strengths of this study are as follows. First, it was a community-based and occupation-based research. This study is important because most studies on FBA are mostly hospital-based studies, except for the study by Matsumoto et al. [
23]. Second, this study is a rare study that explores the external factors affecting the FBA. This study analyzed both internal and external factors influencing femoral bowing and adjusted for the effects of confounding variables.
This suggests that external factors related to agricultural work in female farmers can exacerbate the varus knee deformity through femoral bowing, in addition to internal factors such as age, bone density, height, obesity. This may be an important hypothesis explaining the high prevalence of KOA in female farmers in South Korea.
ACKNOWLEDGMENTS
The authors thank the Ministry of Agriculture, Food and Rural Affairs for financial and administrative assistance for this study.
Abbreviations
anatomical lateral distal femoral angle
anatomical medial proximal tibial angle
non-standardized coefficient beta
standardized coefficient beta
femur bone mineral density
cumulative heavy lifting working time
cumulative squatting working time
intraclass correlation coefficients
Korea farmers' knee cohort
NOTES
-
Funding: This research was supported by the Ministry of Agriculture, Food and Rural Affairs in Republic of Korea.
-
Competing interests: The authors declare that they have no competing interests.
-
Author Contributions:
Conceptualization: Song H, Kim DH.
Data curation: Do S, Kim DH, Lee G.
Investigation: Do S, Song H.
Methodology: Song H, Lee CG.
Writing - original draft: Do S, Song H.
Writing - review & editing: Lee CG, Kim DH, Kim KY, Ryu SY.
SUPPLEMENTARY MATERIAL
Supplementary Table 1
Mean and SD of the angles of lower limb alignment in normal group and radiographic knee OA group from Korea farmers' knee cohort (n = male 504, female 528)
aoem-32-e23-s001.xls
REFERENCES
REFERENCES
- 1. Cross M, Smith E, Hoy D, Nolte S, Ackerman I, Fransen M, et al. The global burden of hip and knee osteoarthritis: estimates from the global burden of disease 2010 study. Ann Rheum Dis 2014;73(7):1323–1330. 24553908.ArticlePubMed
- 2. Kim H, Cho SK, Kim D, Kim D, Jung SY, Jang EJ, et al. Impact of osteoarthritis on household catastrophic health expenditures in Korea. J Korean Med Sci 2018;33(21):e161. 29780297.ArticlePubMedPMCPDF
- 3. Kim IJ, Kim HA, Seo YI, Jung YO, Song YW, Jeong JY, et al. Prevalence of knee pain and its influence on quality of life and physical function in the Korean elderly population: a community based cross-sectional study. J Korean Med Sci 2011;26(9):1140–1146. 21935267.ArticlePubMedPMCPDF
- 4. Hunter DJ, Schofield D, Callander E. The individual and socioeconomic impact of osteoarthritis. Nat Rev Rheumatol 2014;10(7):437–441. 24662640.ArticlePubMedPDF
- 5. Srikanth VK, Fryer JL, Zhai G, Winzenberg TM, Hosmer D, Jones G. A meta-analysis of sex differences prevalence, incidence and severity of osteoarthritis. Osteoarthritis Cartilage 2005;13(9):769–781. 15978850.ArticlePubMed
- 6. Koh IJ, Kim TK, Chang CB, Cho HJ, In Y. Trends in use of total knee arthroplasty in Korea from 2001 to 2010. Clin Orthop Relat Res 2013;471(5):1441–1450. 23054516.ArticlePubMedPMC
- 7. Seok H, Choi SJ, Yoon JH, Song GG, Won JU, Kim JH, et al. The association between osteoarthritis and occupational clusters in the Korean population: a nationwide study. PLoS One 2017;12(1):e0170229. 28099527.ArticlePubMedPMC
- 8. McWilliams DF, Leeb BF, Muthuri SG, Doherty M, Zhang W. Occupational risk factors for osteoarthritis of the knee: a meta-analysis. Osteoarthritis Cartilage 2011;19(7):829–839. 21382500.ArticlePubMed
- 9. Palmer KT. Occupational activities and osteoarthritis of the knee. Br Med Bull 2012;102(1):147–170. 22544778.ArticlePubMedPMC
- 10. Ding C, Cicuttini F, Scott F, Glisson M, Jones G. Sex differences in knee cartilage volume in adults: role of body and bone size, age and physical activity. Rheumatology (Oxford) 2003;42(11):1317–1323. 12810930.ArticlePubMed
- 11. Richmond RS, Carlson CS, Register TC, Shanker G, Loeser RF. Functional estrogen receptors in adult articular cartilage: estrogen replacement therapy increases chondrocyte synthesis of proteoglycans and insulin-like growth factor binding protein 2. Arthritis Rheum 2000;43(9):2081–2090. 11014360.ArticlePubMed
- 12. Jones G, Glisson M, Hynes K, Cicuttini F. Sex and site differences in cartilage development: a possible explanation for variations in knee osteoarthritis in later life. Arthritis Rheum 2000;43(11):2543–2549. 11083279.ArticlePubMed
- 13. Tanamas S, Hanna FS, Cicuttini FM, Wluka AE, Berry P, Urquhart DM. Does knee malalignment increase the risk of development and progression of knee osteoarthritis? A systematic review. Arthritis Rheum 2009;61(4):459–467. 19333985.ArticlePubMed
- 14. Brouwer GM, van Tol AW, Bergink AP, Belo JN, Bernsen RMD, Reijman M, et al. Association between valgus and varus alignment and the development and progression of radiographic osteoarthritis of the knee. Arthritis Rheum 2007;56(4):1204–1211. 17393449.ArticlePubMed
- 15. Sharma L, Chmiel JS, Almagor O, Felson D, Guermazi A, Roemer F, et al. The role of varus and valgus alignment in the initial development of knee cartilage damage by MRI: the MOST study. Ann Rheum Dis 2013;72(2):235–240. 22550314.ArticlePubMedPMC
- 16. Hayashi D, Englund M, Roemer FW, Niu J, Sharma L, Felson DT, et al. Knee malalignment is associated with an increased risk for incident and enlarging bone marrow lesions in the more loaded compartments: the MOST study. Osteoarthritis Cartilage 2012;20(11):1227–1233. 22874524.ArticlePubMedPMC
- 17. Sharma L, Song J, Dunlop D, Felson D, Lewis CE, Segal N, et al. Varus and valgus alignment and incident and progressive knee osteoarthritis. Ann Rheum Dis 2010;69(11):1940–1945. 20511608.ArticlePubMedPMC
- 18. Kim JM, Hong SH, Kim JM, Lee BS, Kim DE, Kim KA, et al. Femoral shaft bowing in the coronal plane has more significant effect on the coronal alignment of TKA than proximal or distal variations of femoral shape. Knee Surg Sports Traumatol Arthrosc 2015;23(7):1936–1942. 24760162.ArticlePubMedPDF
- 19. Park YC, Yoon SP, Yang KH. Localization of atypical femoral fracture on straight and bowed femurs. J Bone Metab 2019;26(2):123–131. 31223609.ArticlePubMedPMCPDF
- 20. Shin WC, Moon NH, Jang JH, Park KY, Suh KT. Anterolateral femoral bowing and loss of thigh muscle are associated with occurrence of atypical femoral fracture: effect of failed tension band mechanism in mid-thigh. J Orthop Sci 2017;22(1):99–104. 27720510.ArticlePubMed
- 21. Chang CB, Choi JY, Koh IJ, Seo ES, Seong SC, Kim TK. What should be considered in using standard knee radiographs to estimate mechanical alignment of the knee? Osteoarthritis Cartilage 2010;18(4):530–538. 20060951.ArticlePubMed
- 22. Sebastian AS, Wilke BK, Taunton MJ, Trousdale RT. Femoral bow predicts postoperative malalignment in revision total knee arthroplasty. J Arthroplasty 2014;29(8):1605–1609. 24704122.ArticlePubMed
- 23. Matsumoto T, Hashimura M, Takayama K, Ishida K, Kawakami Y, Matsuzaki T, et al. A radiographic analysis of alignment of the lower extremities--initiation and progression of varus-type knee osteoarthritis. Osteoarthritis Cartilage 2015;23(2):217–223. 25481289.ArticlePubMed
- 24. Shimosawa H, Nagura T, Harato K, Kobayashi S, Nakamura M, Matsumoto M, et al. Variation of three-dimensional femoral bowing and its relation to physical status and bone mineral density: a study with CT. Surg Radiol Anat 2019;41(12):1489–1495. 31520108.ArticlePubMedPDF
- 25. Kohn MD, Sassoon AA, Fernando ND. Classifications in brief: Kellgren-Lawrence classification of osteoarthritis. Clin Orthop Relat Res 2016;474(8):1886–1893. 26872913.ArticlePubMedPMCPDF
- 26. Altman RD, Gold GE. Atlas of individual radiographic features in osteoarthritis, revised. Osteoarthritis Cartilage 2007;15(Suppl A):A1–A56. 17320422.ArticlePubMed
- 27. Wright RW. MARS Group. Osteoarthritis classification scales: interobserver reliability and arthroscopic correlation. J Bone Joint Surg Am 2014;96(14):1145–1151. 25031368.ArticlePubMedPMC
- 28. Colebatch AN, Hart DJ, Zhai G, Williams FM, Spector TD, Arden NK. Effective measurement of knee alignment using AP knee radiographs. Knee 2009;16(1):42–45. 18790641.ArticlePubMed
- 29. Lasam MP, Lee KJ, Chang CB, Kang YG, Kim TK. Femoral lateral bowing and varus condylar orientation are prevalent and affect axial alignment of TKA in Koreans. Clin Orthop Relat Res 2013;471(5):1472–1483. 23011845.ArticlePubMedPMC
- 30. Jeong CH, Noh JH. Clinical and radiological analysis of angular deformity of lower extremities. J Korean Fract Soc 2017;30(3):156–166.ArticlePDF
- 31. Luo CF, Zeng BF, Koshino T. Transepicondylar line and condylar line as parameters for axial alignment in knee arthroplasty. Knee 2004;11(3):213–217. 15194098.ArticlePubMed
- 32. Cooke D, Scudamore A, Li J, Wyss U, Bryant T, Costigan P. Axial lower-limb alignment: comparison of knee geometry in normal volunteers and osteoarthritis patients. Osteoarthritis Cartilage 1997;5(1):39–47. 9010877.ArticlePubMed
- 33. Lu Y, Zheng Z, Chen W, Lv H, Lv J, Zhang Y. Dynamic deformation of femur during medial compartment knee osteoarthritis. PLoS One 2019;14(12):e0226795. 31860687.ArticlePubMedPMC
- 34. Song MH, Yoo SH, Kang SW, Kim YJ, Park GT, Pyeun YS. Coronal alignment of the lower limb and the incidence of constitutional varus knee in Korean females. Knee Surg Relat Res 2015;27(1):49–55. 25750894.ArticlePubMedPMC
- 35. Nagamine R, Miura H, Bravo CV, Urabe K, Matsuda S, Miyanishi K, et al. Anatomic variations should be considered in total knee arthroplasty. J Orthop Sci 2000;5(3):232–237. 10982663.ArticlePubMed
- 36. Mullaji AB, Marawar SV, Mittal V. A comparison of coronal plane axial femoral relationships in Asian patients with varus osteoarthritic knees and healthy knees. J Arthroplasty 2009;24(6):861–867. 18701244.ArticlePubMed
- 37. Yau WP, Chiu KY, Tang WM, Ng TP. Coronal bowing of the femur and tibia in Chinese: its incidence and effects on total knee arthroplasty planning. J Orthop Surg (Hong Kong) 2007;15(1):32–36. 17429114.ArticlePubMedPDF
- 38. Esposito S, Leonardi A, Lanciotti L, Cofini M, Muzi G, Penta L. Vitamin D and growth hormone in children: a review of the current scientific knowledge. J Transl Med 2019;17(1):87. 30885216.ArticlePubMedPMCPDF
- 39. Chung YS, Chung DJ, Kang MI, Kim IJ, Koh JM, Min YK, et al. Vitamin D repletion in Korean postmenopausal women with osteoporosis. Yonsei Med J 2016;57(4):923–927. 27189286.ArticlePubMedPMCPDF
- 40. Bhan A, Rao AD, Rao DS. Osteomalacia as a result of vitamin D deficiency. Endocrinol Metab Clin North Am 2010;39(2):321–331. 20511054.ArticlePubMed
- 41. Zhang Y, Hunter DJ, Nevitt MC, Xu L, Niu J, Lui LY, et al. Association of squatting with increased prevalence of radiographic tibiofemoral knee osteoarthritis: the Beijing Osteoarthritis Study. Arthritis Rheum 2004;50(4):1187–1192. 15077301.ArticlePubMed
- 42. Shanb AA, Youssef EF. The impact of adding weight-bearing exercise versus nonweight bearing programs to the medical treatment of elderly patients with osteoporosis. J Family Community Med 2014;21(3):176–181. 25374469.ArticlePubMedPMC

 , Chul Gab Lee1
, Chul Gab Lee1

 Cite
Cite