
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 36; 2024 > Article
- Original Article Impact of neck posture and insulating stick use on neck disability in Korean line workers: a cross-sectional study
-
Bounggyun Ju
 , Jaehoo Lee, Hye-min Kim, Chul Gab Lee, Hansoo Song
, Jaehoo Lee, Hye-min Kim, Chul Gab Lee, Hansoo Song -
Annals of Occupational and Environmental Medicine 2024;36:e11.
DOI: https://doi.org/10.35371/aoem.2024.36.e11
Published online: April 15, 2024
Department of Occupational and Environmental Medicine, Chosun University Hospital, Gwangju, Korea.
- Correspondence: Hansoo Song. Department of Occupational and Environmental Medicine, Chosun University Hospital, Gwangju, 365 Pilmun-daero, Dong-gu, Gwangju 61453, Korea. oemsong@chosun.ac.kr
• Received: January 31, 2024 • Revised: March 29, 2024 • Accepted: April 9, 2024
Copyright © 2024 Korean Society of Occupational & Environmental Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background Occupational neck disability is a prevalent issue, especially among line workers, who are often exposed to elevated levels of cervical ergonomic stress. The aim of this study was to investigate the impact of neck posture and insulating stick use on neck disability in a specific occupational group in Korea.
-
Methods This cross-sectional study was conducted among 483 line workers in Gwangju and Jeonnam, Korea. Data were collected using the Neck Disability Index, Cervical Degenerative Index, and a structured questionnaire focusing on demographic and occupational factors. Logistic regression analysis was applied to determine the adjusted odds ratio (OR) and 95% confidence interval (CI) for neck posture and factors related to neck disability.
-
Results Neck disability prevalence was 17.2% among the participants. Multivariate logistic regression analysis showed that factors related to neck disability included age over 60 years (adjusted OR: 3.08; 95% CI: 1.63–5.83), depression (adjusted OR: 8.33; 95% CI: 3.85–18.00), a history of cervical trauma (adjusted OR: 2.13; 95% CI: 1.04–4.40), and radiological degenerative changes in the cervical spine (adjusted OR: 2.33; 95% CI: 1.26–4.33). In particular, the adjusted OR of neck disability among live-line workers was 2.10 (95% CI: 1.12–3.92) when compared with support workers (model 1). Other analysis models showed that use of insulating sticks for more than 10 hours per week (adjusted OR: 2.46; 95% CI: 1.32–4.61) and higher neck extension (adjusted OR: 2.98; 95% CI: 1.14–3.46) were significant work-related risk factors (model 2,3).
-
Conclusions Neck posture, age, depression, cervical trauma history, degenerative changes in the cervical spine, and use of insulating sticks are significant risk factors for neck disability among line workers in Korea. These findings highlight the need to improve the working environment and reduce the burden of cervical ergonomic stress among line workers.
BACKGROUND
Neck disability is a significant health issue affecting various populations, with implications on quality of life, functional capabilities, and psychological well-being.1 In occupational settings, neck disability is important due to its economic impact, including direct medical costs and indirect costs such as loss of productivity and compensation claims.2 Notably individuals with professions that require repetitive movements, heavy lifting, or prolonged static postures, are at an increased risk of neck disability.3,4,5,6,7
Among them, line workers, also called linemen, powerline workers, electric utility line workers, or electric power industry workers, who are responsible for constructing and maintaining electric transmission and distribution facilities, stand out. Their occupation is notorious for its high injury and fatality rates.8,9 These workers are exposed to unique challenges, such as working at high heights and using heavy equipment.10 Some studies have reported high neck injury rates in this occupation due to these strenuous conditions.11,12
In the past, line workers handled live electricity wearing insulated gloves. This method is known for its high electric shock rate. To reduce this risk, an indirect method that involves the use of insulating sticks was proposed.13 The stick is known by names such as high voltage hot stick, telescopic hot stick, and smart stick. Although the method has significantly led to a reduction in electric shock incidences, it has created new problems. Insulating sticks are heavy and difficult to handle, causing workers to hyperextend their cervical spine while working.
Studies on occupational risk factors of neck pain or disability have mainly been conducted among office workers14,15 and healthcare workers.16,17 These factors include inappropriate neck posture, long working hours, and job stress. However, research on neck pain or disability among manual workers is relatively lacking. Specifically, only a few studies have been carried out on occupations that require an upward-looking posture. Therefore, the aim of this study was to investigate the characteristics and occupational risk factors of neck disorders among Korean line workers with relatively evident cervical spine burdens. Particularly, there was a focus on the impact of using insulating sticks, reflecting recent changes in the uninterrupted technique (Fig. 1).

METHODS
A cross-sectional design was used to investigate the association between work-related factors and neck disability among line workers in Korea. A sample of 483 line workers, representing approximately 58.2% of the total membership of 830 individuals, was sourced from the Gwangju Jeonnam Construction Labor Union for this study. In addition to line workers, support workers (assistants, heavy vehicle operators, and supervisors) served as the control group for comparison. Line workers were further categorized into dead- and live-line workers to assess the impact of different work conditions on cervical ergonomic stress. Dead-line workers worked on de-energized lines, meaning electrical power is turned off during maintenance or repair activities. Conversely, live-line workers worked on energized lines, often at high heights, and used specialized equipment, such as insulating sticks or insulated aerial lifts. The dependent variable in this study was neck disability, defined as a dichotomous variable. Independent variables were divided into general factors and occupational factors. General factors included age, depression, and neck trauma history. Occupational factors included job type, insulating stick use, and neck ergonomic hazard.
The participants completed a questionnaire that included items related to their subjective symptoms, work history, and demographic variables (age, job type, and neck trauma history). Neck disability was quantified using the Neck Disability Index (NDI).18 The NDI consists of 10 items measured on a 5-point Likert scale asking about neck pain and disability in daily living. The reliability and validity of the Korean version of the NDI are adequate.19 The NDI score ranges from 0 to 50, with a score ≥ 35 indicating complete disability. In this study, neck disability was defined as scoring ≥ 15 points, which is the standard for moderate disability. Survey questions were used to evaluate intensity and frequency by applying Quick Exposure Check (QEC) list to assess ergonomic risk factors.20 Frequency was classified as none, infrequent, frequent, and very frequent (almost continuous movement) according to the QEC D-question. Intensity was classified as not at all, mildly, moderately, and very stressful according to the QEC Q-question. Frequency and intensity of work tasks were scored on a scale of 0–3. The resultant “exposure score” was calculated by multiplying these scores, with a score ≥ 6 considered indicative of high-risk work (Supplementary Table 1). Depression was assessed using the Korean version of Patient Health Questionnaire-2 (PHQ-2).21 The PHQ-2 consists of two questionnaires assessing the frequency of decreased interest and depressed mood over the past two weeks. The PHQ-2 score ranges from 0 to 6, with a score ≥ 3 indicating depression.
Physical examinations such as range of motion limitation, Spurling’s test, Lhermitte’s test, and tenderness of the upper trapezius, levator scapulae, and splenius capitis were performed among the participants. A positive result for range of motion limitation is indicated when asymmetry is observed in the amount of rotation, side bending, or insufficiency in the angle of flexion and extension. A positive Spurling's test result is indicated when arm symptoms are provoked with the neck in extension, lateral flexion, and axial compression.22 A positive Lhermitte's test result is indicated when a transient electric shock-like sensation extends exclusively down the extremities due to neck flexion. Tenderness is considered positive when pressure applied with a standardized finger force of 2 kg causes pain in the affected area.23
Two independent readers (A and B) evaluated the cervical radiographs of the study participants using the Picture Archiving and Communication System. The findings, as summarized in Supplementary Table 2, include a detailed assessment of the Cervical Degenerative Index across different cervical levels (C2-3, C3-4, C4-5, C5-6, and C6-7).24 The table categorizes degenerative changes as none, mild, moderate, or severe, and provides additional information on disc space narrowing, osteophyte formation, and sclerosis. In this study, a joint was considered to exhibit degenerative changes if rated as moderate or severe at any level.25,26,27 The presence of one or more joints with such changes was considered indicative of degenerative change. The agreement level between the readers was evaluated using the kappa statistic (0.691) for binary classification of degenerative changes, and discrepancies were resolved through consensus.23,24
Data analysis was conducted using STATA version 18.0 (StataCorp, College Station, TX, USA). A χ2 test was performed to identify the variables significantly associated with neck disability. A multiple logistic regression analysis was used to assess the association between the variables and neck disability. Three analysis results were presented according to occupational factors: job type, use of insulating sticks, neck posture factors, considering the possibility of multicollinearity between factors.
This study was approved by the Institutional Review Board of Chosun University Hospital (approval No. CHOSUN 2021-07-044). This study was conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants, and data confidentiality was maintained throughout the study.
RESULTS
In total, 483 line workers from the Gwangju and Jeonnam Construction Labor Unions participated in this study. The participant’s average age was 49.0 (standard deviation: 10.7; range: 23–72) years. The majority of the participants were live-line workers (44.9%, n = 217), followed by dead-line workers (26.1%, n = 126), assistants (13.0%, n = 63), heavy vehicle operators (9.7%, n = 47), and supervisors (6.2%, n = 30) (Table 1).
Table 1
Participant characteristics by job types
Values are presented as number (%). p-value by χ2 test.
SD: standard deviation.
aDepression: Patient Health Questionnaire-2 score 3 or higher; bDegenerative change: children's depression inventory score of moderate or higher in more than one cervical joint; cExposure score: low—exposure score below 6, high—exposure score 6 or higher; dNeck disability: Neck Disability Index score moderate or higher.
Regarding health history, 10.4% of the participants reported cervical trauma history, and 7.7% exhibited depressive symptoms, scoring ≥ 3 points on the PHQ-2 questionnaire. Neck ergonomic exposure revealed that 17.8% of the participants were involved in high-risk work requiring neck flexion, 52.2% in high-risk work requiring neck extension. Regarding the use of insulating sticks, 52.4% did not use them, 24.2% used them for less than 10 hours per week, and 23.4% used them for more than 10 hours per week.
Neck disability prevalence, defined by a score ≥ 15 on the NDI, was 17.2% (Table 2). This prevalence was highest among live-line workers (22.6%). Univariate analysis showed several factors significantly associated with neck disability, including being over 60 years of age (odds ratio [OR]: 3.05; 95% confidence interval [CI]: 1.77–5.28), having depressive symptoms (OR: 8.13; 95% CI: 4.02–16.43), and a history of cervical trauma (OR: 3.53; 95% CI: 1.88–6.63). Other significant variables included degenerative changes in the cervical spine (OR: 2.35; 95% CI: 1.36–4.07), being a live-line worker (OR: 1.56; 95% CI: 0.90–2.73), spending ≥ 10 hours per week using insulating sticks (OR: 2.12; 95% CI: 1.21–3.71), engaging in work requiring neck flexion (OR: 2.22; 95% CI: 1.28–3.83), and engaging in work requiring neck extension (OR: 2.31; 95% CI: 1.39–3.81). The multivariate analysis was organized into three models, underscoring the multifaceted nature of occupational risk factors. Model 1 revealed that live-line workers had an increased risk of neck disability (adjusted OR: 2.10; 95% CI: 1.12–3.92). Model 2 showed that insulating stick use for ≥ 10 hours per week was a significant risk factor (adjusted OR: 2.46; 95% CI: 1.32–4.61). Model 3 identified high rate of work requiring neck extension as a risk factor (adjusted OR: 1.98; 95% CI: 1.14–3.46). Across these models, age ≥ 60 years (adjusted OR: 2.26; 95% CI: 1.22–4.16), depression (adjusted OR: 7.22; 95% CI: 3.36–15.51), cervical trauma history (adjusted OR: 2.37; 95% CI: 1.17–4.82), and degenerative changes in the cervical spine (adjusted OR: 2.34; 95% CI: 1.27–4.33) consistently showed strong correlations with neck disability (Table 3).
Table 2
Prevalence of neck disabilitya
Values are presented as number (%). p-value by χ2 test.
aNeck disability: moderate to high Neck Disability Index score; bDepression: Patient Health Questionnaire-2 score 3 or higher; cDegenerative change: children's depression inventory score of moderate or higher in more than one cervical joint; dExposure score: low—exposure score below 6, high—exposure score 6 or higher.
Table 3
Logistic regression analysis of relative factors for neck disabilitya
Bolds are presented as statistically significance.
OR: odds ratio; CI: confidence interval.
aNeck disability: moderate to high Neck Disability Index score; bDepression: Patient Health Questionnaire-2 score 3 or higher; cDegenerative change: children's depression inventory score of moderate or higher in more than one cervical joint; dExposure score: low—exposure score below 6, high—exposure score 6 or higher.
DISCUSSION
In our study, we found that neck disability prevalence was particularly high among live-line workers but lower among dead-line workers. The duration of insulating stick use showed a dose-response relationship with neck disability. Among awkward neck postures, only the extension posture showed a significant correlation. Live-line workers often use insulating sticks. As a result, both the frequency and intensity of cervical extension increased in live-line workers compared with other workers (Supplementary Table 1).
Several studies have been carried out regarding neck disorders among surgeons using endoscopes.28,29,30,31 These studies serve as meaningful analogies for our research. In the past, line workers handled high voltage electric lines with insulated gloves, but recently, they have been using insulating sticks. This parallels the transition from surgeons depending on their own manual dexterity to surgeons utilizing indirect equipment. Among both line workers and surgeons, the use of indirect equipment was an independent risk factor for neck disability, even after adjusting for psychosocial stress.
Line workers have ergonomic risks similar to those of construction workers or grape growers.3 Examples of occupations that require working with an awkward neck posture include dentistry, construction work, and farming. A study on neck disorders among dentists indicated that awkward postures and repeated movements, such as bending and twisting of the cervical spine, were related to neck disorders.32,33 In a study on the occurrence of surgically treated cervical spondylosis in construction workers, occupational exposure to non-neutral neck postures, working with hands above shoulders, and carrying heavy loads emerged as risk factors.6 A study carried out to compare neck disorders among grape growers and eggplant growers suggested that neck extension movement was a risk factor.3
As expected, age was related to neck disability, as neck disability prevalence was higher among patients aged > 60 years than among those aged < 60 years. We hypothesized that age-related degenerative changes in the cervical spine could explain neck disability.34,35 It is difficult to determine the severity of cervical degenerative changes in line workers compared with the general population. However, despite adjusting for degenerative changes in the cervical spine, age remained an independent factor associated with neck disability. This indicates that the effect of age cannot be explained solely by the degenerative changes in the cervical spine. Compared with the findings of Tao et al.,34 the prevalence of moderate-to-severe degenerative changes in C5/C6 among line workers was similar to that in the general population. However, the average age of the participants in this study was 3.3 years younger than that of our study. These results suggest that cervical degenerative changes may progress more rapidly in line workers than in the general population.
In this study, depression was highly correlated with neck disabilities. This result is consistent with those of existing studies. Musculoskeletal disorders of the neck have a higher correlation with mental health than those of other parts of the body.36,37,38 The strong correlation between depression and neck pain suggests an interplay between physical and psychological factors in the development of musculoskeletal disorders.2
When interpreting our study's findings, some caveats and limitations of this study should be considered. It is important to note that other workers sometimes use insulating sticks. This is because there are cases where dead-line and support workers replace or assist the task of live-line workers. Because cervical spine disorder rarely occurs before the age of 50 years, the number of cases was too small to compare between those younger and older than 50 years. Disability has inherent limits to objectification. Social or occupational limitations may lead to greater disability.39 In this study, neck disability was compared with a physician's objective assessment to understand the extent to which objectivity can be achieved. As a result, when there were two or more positive findings in the physical examinations, the neck disability OR was 11.56 (95% CI: 4.65–28.74). Therefore, although the NDI is a subjective evaluation, it also showed high agreement with the objective evaluation (Supplementary Table 3). Time and distance constraints reduced the willingness of line workers to visit the hospital. However, since the workers visited together, it is difficult to believe that the sample disproportionately consisted of symptomatic individuals.
As this was a cross-sectional study, the ability to establish temporal relationships was limited. However, a history of neck injury, radiologically degenerative changes in the cervical spine, and recent cervical strain surgeries can be used to infer temporal sequences. The control group in our study comprised those doing support work. Support workers experience a relatively low level of cervical strain; however, the level of cervical strain may be higher than that in the general population. This indicates that the relative risk ratio in this study may have been underestimated. Additionally, the control group may have included people previously working as live-line workers. However, being healthy survivors may also have an effect.
Despite these limitations, this study is meaningful because, to our knowledge, it is the first to address the impact of insulating stick use as an occupational risk factor for neck disability among line workers.
CONCLUSIONS
This study shows that live-line workers who mainly use insulating sticks experience a high level of cervical strain and have a high neck disability prevalence. Additionally, dead-line workers, who work without insulating sticks, have a lower neck disability prevalence. Insulating sticks were introduced to reduce the risk of electric shock among workers while allowing for uninterrupted techniques. However, the use of insulating sticks can cause neck disabilities among workers. Uninterrupted techniques in electrical maintenance allow continued electricity use for citizens but can negatively impact the safety and health of line workers.
Acknowledgments
The authors thank the Gwangju Jeonnam Construction Labor Union.
Abbreviations
CI
confidence interval
NDI
Neck Disability Index
OR
odds ratio
PHQ-2
Patient Health Questionnaire-2
QEC
Quick Exposure Check
-
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
-
Competing interests: The authors declare that they have no competing interests.
-
Author Contributions:
NOTES
SUPPLEMENTARY MATERIALS
Supplementary Table 3
Logistic regression analysis of neck disability with positive physical exam count
- 1. Hoy D, March L, Woolf A, Blyth F, Brooks P, Smith E, et al. The global burden of neck pain: estimates from the global burden of disease 2010 study. Ann Rheum Dis 2014;73(7):1309–1315. 24482302.ArticlePubMed
- 2. Côté P, van der Velde G, Cassidy JD, Carroll LJ, Hogg-Johnson S, Holm LW, et al. The burden and determinants of neck pain in workers: results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. Spine (Phila Pa 1976) 2008;33(4):Suppl. S60–S74. 18204402.PubMed
- 3. Takamiya Y, Nagata K, Fukuda K, Shibata A, Ishitake T, Suenaga T. Cervical spine disorders in farm workers requiring neck extension actions. J Orthop Sci 2006;11(3):235–240. 16721522.ArticlePubMed
- 4. Thetkathuek A, Meepradit P, Sa-Ngiamsak T. A cross-sectional study of musculoskeletal symptoms and risk factors in Cambodian fruit farm workers in eastern region, Thailand. Saf Health Work 2018;9(2):192–202. 29928534.ArticlePubMedPMC
- 5. Lee YC, Hong X, Man SS. Prevalence and associated factors of work-related musculoskeletal disorders symptoms among construction workers: a cross-sectional study in South China. Int J Environ Res Public Health 2023;20(5):4653. 36901662.ArticlePubMedPMC
- 6. Jackson JA, Liv P, Sayed-Noor AS, Punnett L, Wahlström J. Risk factors for surgically treated cervical spondylosis in male construction workers: a 20-year prospective study. Spine J 2023;23(1):136–145. 36028215.ArticlePubMed
- 7. Hunting KL, Welch LS, Cuccherini BA, Seiger LA. Musculoskeletal symptoms among electricians. Am J Ind Med 1994;25(2):149–163. 8147388.ArticlePubMed
- 8. Vergara X, Bhatnagar M, Fordyce T. Exploratory narrative text analysis to characterize tasks associated with injuries among electric utility line workers: EPRI Occupational Health and Safety Database 1995–2013. Am J Ind Med 2021;64(3):198–207. 33373058.ArticlePubMedPDF
- 9. Fordyce TA, Kelsh M, Lu ET, Sahl JD, Yager JW. Thermal burn and electrical injuries among electric utility workers, 1995–2004. Burns 2007;33(2):209–220. 17116371.ArticlePubMed
- 10. Moriguchi CS, Carnaz L, Alencar JF, Miranda Júnior LC, Granqvist L, Hansson GÅ, et al. Postures and movements in the most common tasks of power line workers. Ind Health 2011;49(4):482–491. 21697620.ArticlePubMed
- 11. Padmanathan V, Joseph L, Omar B, Nawawi R. Prevalence of musculoskeletal disorders and related occupational causative factors among electricity linemen: a narrative review. Int J Occup Med Environ Health 2016;29(5):725–734. 27518883.ArticlePubMed
- 12. Fordyce TA, Morimoto L, Coalson J, Kelsh MA, Mezei G. Neck injuries among electric utility workers, 1995–2007. J Occup Environ Med 2010;52(4):441–449. 20357677.ArticlePubMed
- 13. Bottauscio O, Arduino A, Bavastro D, Capra D, Guarneri A, Parizia AA, et al. Exposure of live-line workers to magnetic fields: a dosimetric analysis. Int J Environ Res Public Health 2020;17(7):2429. 32252473.ArticlePubMedPMC
- 14. Jun D, Zoe M, Johnston V, O’Leary S. Physical risk factors for developing non-specific neck pain in office workers: a systematic review and meta-analysis. Int Arch Occup Environ Health 2017;90(5):373–410. 28224291.ArticlePubMedPDF
- 15. Ye S, Jing Q, Wei C, Lu J. Risk factors of non-specific neck pain and low back pain in computer-using office workers in China: a cross-sectional study. BMJ Open 2017;7(4):e014914.ArticlePubMedPMC
- 16. Yuan S, Li Y, Zhang L, Wang H. The relationship between the NSP and the individual and work organizational variables: a cross-sectional study. Front Public Health 2022;10:726826. 35433581.ArticlePubMedPMC
- 17. Onda A, Onozato K, Kimura M. Clinical features of neck and shoulder pain (Katakori) in Japanese hospital workers. Fukushima J Med Sci 2022;68(2):79–87. 35660659.PubMedPMC
- 18. Vernon H. The Neck Disability Index: state-of-the-art, 1991–2008. J Manipulative Physiol Ther 2008;31(7):491–502. 18803999.ArticlePubMed
- 19. Song KJ, Choi BW, Choi BR, Seo GB. Cross-cultural adaptation and validation of the Korean version of the neck disability index. Spine (Phila Pa 1976) 2010;35(20):E1045–E1049. 20436378.ArticlePubMed
- 20. David G, Woods V, Li G, Buckle P. The development of the Quick Exposure Check (QEC) for assessing exposure to risk factors for work-related musculoskeletal disorders. Appl Ergon 2008;39(1):57–69. 17512492.ArticlePubMed
- 21. Jo M, Koo HY, Cho IY, Lee Y, Yoon S, Yang Y, et al. Usefulness of the patient health questionnaire-2 in screening for depression. Korean J Fam Pract 2019;9(4):336–340.Article
- 22. Thoomes EJ, van Geest S, van der Windt DA, Falla D, Verhagen AP, Koes BW, et al. Value of physical tests in diagnosing cervical radiculopathy: a systematic review. Spine J 2018;18(1):179–189. 28838857.ArticlePubMed
- 23. Andersen LL, Hansen K, Mortensen OS, Zebis MK. Prevalence and anatomical location of muscle tenderness in adults with nonspecific neck/shoulder pain. BMC Musculoskelet Disord 2011;12(1):169. 21777478.ArticlePubMedPMCPDF
- 24. Ofiram E, Garvey TA, Schwender JD, Denis F, Perra JH, Transfeldt EE, et al. Cervical degenerative index: a new quantitative radiographic scoring system for cervical spondylosis with interobserver and intraobserver reliability testing. J Orthop Traumatol 2009;10(1):21–26. 19384631.ArticlePubMedPMCPDF
- 25. Walraevens J, Liu B, Meersschaert J, Demaerel P, Delye H, Depreitere B, et al. Qualitative and quantitative assessment of degeneration of cervical intervertebral discs and facet joints. Eur Spine J 2009;18(3):358–369. 19005690.ArticlePubMedPDF
- 26. Kettler A, Rohlmann F, Neidlinger-Wilke C, Werner K, Claes L, Wilke HJ. Validity and interobserver agreement of a new radiographic grading system for intervertebral disc degeneration: part II. Cervical spine. Eur Spine J 2006;15(6):732–741. 16614855.ArticlePubMedPMCPDF
- 27. Choi SH, Lee H, Cho JH, Jung JI, Lee DH. Radiological parameters of undegenerated cervical vertebral segments in a Korean population. Clin Orthop Surg 2017;9(1):63–70. 28261429.ArticlePubMedPMCPDF
- 28. Norheim EP, Black MH, Ngor EW, Shi JM, Safran MR, Navarro RA. Cervical spine disease in surgeons performing arthroscopy or laparoscopy. Arch Environ Occup Health 2019;74(4):206–214. 29035681.ArticlePubMed
- 29. Wyatt RW, Lin CC, Norheim EP, Przepiorski D, Navarro RA. Occupation-related cervical spine disease in orthopaedic surgeons. J Am Acad Orthop Surg 2020;28(17):730–736. 32324708.ArticlePubMed
- 30. Acharya H, Patel P, Shetty GM, Shah M, Bamb H, Nene A. Prevalence and risk factors of neck pain in spine surgeons - Are we our own patients? J Clin Orthop Trauma 2022;33:102012. 36110511.ArticlePubMedPMC
- 31. Abolfotouh SM, Alnori O, Choma T, Moore D, Abolfotouh MA. Epidemiology of work-related neck pain among spine surgeons. Global Spine J 2022.ArticlePDF
- 32. Soo SY, Ang WS, Chong CH, Tew IM, Yahya NA. Occupational ergonomics and related musculoskeletal disorders among dentists: a systematic review. Work 2023;74(2):469–476. 36278379.ArticlePubMed
- 33. Rahmani N, Amiri M, Mohseni-Bandpei MA, Mohsenifar H, Pourahmadi MR. Work related neck pain in Iranian dentists: an epidemiological study. J Back Musculoskeletal Rehabil 2013;26(1):9–15.Article
- 34. Tao Y, Galbusera F, Niemeyer F, Samartzis D, Vogele D, Wilke HJ. Radiographic cervical spine degenerative findings: a study on a large population from age 18 to 97 years. Eur Spine J 2021;30(2):431–443. 33025192.ArticlePubMedPDF
- 35. Lv Y, Tian W, Chen D, Liu Y, Wang L, Duan F. The prevalence and associated factors of symptomatic cervical Spondylosis in Chinese adults: a community-based cross-sectional study. BMC Musculoskelet Disord 2018;19(1):325. 30205836.ArticlePubMedPMCPDF
- 36. Xie Y, Coombes BK, Thomas L, Johnston V. Time course and risk profile of work-related neck disability: a longitudinal latent class growth analysis. Phys Ther 2022;102(6):pzac050. 35485191.ArticlePubMedPMCPDF
- 37. Sawada T, Matsudaira K, Muto Y, Koga T, Takahashi M. Potential risk factors for onset of severe neck and shoulder discomfort (Katakori) in urban Japanese workers. Ind Health 2016;54(3):230–236. 26829974.ArticlePubMedPMC
- 38. Johnston V, Jull G, Souvlis T, Jimmieson NL. Interactive effects from self-reported physical and psychosocial factors in the workplace on neck pain and disability in female office workers. Ergonomics 2010;53(4):502–513. 20309746.ArticlePubMed
- 39. Perenboom RJ, Wijlhuizen GJ, Garre FG, Heerkens YF, van Meeteren NL. An empirical exploration of the relations between the health components of the International Classification of Functioning, Disability and Health (ICF). Disabil Rehabil 2012;34(18):1556–1561. 22239620.ArticlePubMed
REFERENCES
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Effects of dry needling on functioning and pain relief in patients with chronic nonspecific neck pain: a systematic review and meta-analysis of randomized controlled trials
Alessandro de Sire, Nicola Marotta, Maria Sgro, Isabella Bartalotta, Roberta Zito, Dario Calafiore, Francesco Agostini, Michele Vecchio, Umile Giuseppe Longo, Antonio Ammendolia
Disability and Rehabilitation.2026; 48(1): 51. CrossRef - List of occupational diseases among farmers in Korea: a literature review
Hansoo Song, Seok-Ju Yoo, Won-Ju Park, Seunghyeon Cho, Ki Soo Park, Joo Hyun Sung, Sang Jin Park, Seong-yong Yoon, Kyeongsoo Kim, Dong-phil Choi, Hye-min Kim, Bounggyun Ju, Kanwoo Youn
Ann Occup Environ Med.2025; 37: e2. CrossRef - Dry needling in alleviating pain and enhancing function in neck pain: a scoping review
Isabella Bartalotta, Nicola Marotta, Roberta Zito, Maria Sgro, Dario Calafiore, Francesco Agostini, Michele Vecchio, Umile Giuseppe Longo, Antonio Ammendolia, Alessandro de Sire
International Journal of Bone Fragility.2025; 5(5): 46. CrossRef
 Cite
CiteImpact of neck posture and insulating stick use on neck disability in Korean line workers: a cross-sectional study
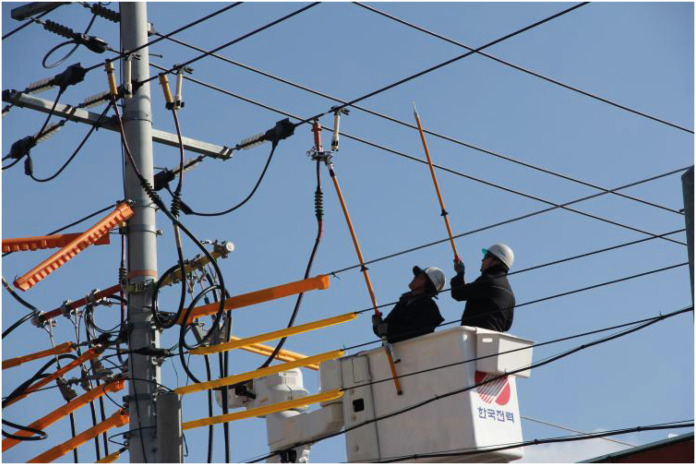
Fig. 1 Line workers (photo by Gwangju Jeonnam Construction Labor Union).
Fig. 1
Impact of neck posture and insulating stick use on neck disability in Korean line workers: a cross-sectional study
| Factors | Group | Support | Dead-line | Live-line | Total | |
|---|---|---|---|---|---|---|
| Age | < 60 | 111 (79.3) | 99 (78.6) | 195 (89.9) | 405 (83.9) | 0.005 |
| ≥ 60 | 29 (20.7) | 27 (21.4) | 22 (10.1) | 78 (16.1) | ||
| Mean ± SD | 49.3 ± 12.0 | 47.6 ± 12.1 | 49.8 ± 8.9 | 49.0 ± 10.7 | ||
| Career | < 10 | 53 (37.9) | 57 (45.2) | 27 (12.4) | 137 (28.4) | < 0.001 |
| ≥ 10 | 87 (62.1) | 69 (54.8) | 190 (87.6) | 346 (71.6) | ||
| Mean ± SD | 18.5 ± 13.3 | 18.3 ± 14.5 | 24.5 ± 10.2 | 21.1 ± 12.7 | ||
| Depressiona | No | 127 (90.7) | 119 (94.4) | 200 (92.2) | 446 (92.3) | 0.517 |
| Yes | 13 (9.3) | 7 (5.6) | 17 (7.8) | 37 (7.7) | ||
| Neck trauma history | No | 124 (88.6) | 118 (93.7) | 191 (88.0) | 433 (89.6) | 0.226 |
| Yes | 16 (11.4) | 8 (6.3) | 26 (12.0) | 50 (10.4) | ||
| Cervical degenerative changeb | No | 115 (82.1) | 105 (83.3) | 180 (82.9) | 400 (82.8) | 0.965 |
| Yes | 25 (17.9) | 21 (16.7) | 37 (17.1) | 83 (17.2) | ||
| Neck flexionc | Low | 125 (89.3) | 104 (82.5) | 168 (77.4) | 397 (82.2) | 0.017 |
| High | 15 (10.7) | 22 (17.5) | 49 (22.6) | 86 (17.8) | ||
| Neck extensionc | Low | 83 (59.3) | 70 (55.6) | 78 (35.9) | 231 (47.8) | < 0.001 |
| High | 57 (40.7) | 56 (44.4) | 139 (64.1) | 252 (52.2) | ||
| Insulating stick use/week | None | 136 (97.1) | 110 (87.3) | 7 (3.2) | 253 (52.4) | < 0.001 |
| < 10 hours | 3 (2.1) | 13 (10.3) | 101 (46.5) | 117 (24.2) | ||
| ≥ 10 hours | 1 (0.7) | 3 (2.4) | 109 (50.2) | 113 (23.4) | ||
| Neck disabilityd | No | 118 (84.3) | 114 (90.5) | 168 (77.4) | 400 (82.8) | 0.007 |
| Yes | 22 (15.7) | 12 (9.5) | 49 (22.6) | 83 (17.2) |
| Factors | Group | Neck disability | ||
|---|---|---|---|---|
| No | Yes | |||
| Age | < 60 | 348 (85.9) | 57 (14.1) | < 0.001 |
| ≥ 60 | 52 (66.7) | 26 (33.3) | ||
| Career | < 10 | 131 (95.6) | 6 (4.4) | < 0.001 |
| ≥ 10 | 269 (77.8) | 77 (22.2) | ||
| Depressionb | No | 384 (86.1) | 62 (13.9) | < 0.001 |
| Yes | 16 (43.2) | 21 (56.8) | ||
| Neck trauma history | No | 369 (85.2) | 64 (14.8) | < 0.001 |
| Yes | 31 (62.0) | 19 (38.0) | ||
| Cervical degenerative changec | No | 341 (85.2) | 59 (14.8) | 0.002 |
| Yes | 59 (71.1) | 24 (28.9) | ||
| Neck flexiond | Low | 338 (85.1) | 59 (14.9) | 0.004 |
| High | 62 (72.1) | 24 (27.9) | ||
| Neck extensiond | Low | 205 (88.7) | 26 (11.3) | 0.001 |
| High | 195 (77.4) | 57 (22.6) | ||
| Insulating stick use/week | None | 219 (86.6) | 34 (13.4) | 0.028 |
| < 10 hours | 96 (82.0) | 21 (18.0) | ||
| ≥ 10 hours | 85 (75.2) | 28 (24.8) | ||
| Factors | Group | Unadjusted OR (95% CI) | Adjusted OR (95% CI) | ||
|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | |||
| Age | < 60 | 1 | 1 | 1 | 1 |
| ≥ 60 | 3.05 (1.77–5.28) | 3.08 (1.63–5.83) | 2.80 (1.49–5.26) | 2.26 (1.22–4.16) | |
| Depressionb | No | 1 | 1 | 1 | 1 |
| Yes | 8.13 (4.02–16.43) | 8.33 (3.85–18.00) | 8.13 (3.80–17.40) | 7.22 (3.36–15.51) | |
| Neck trauma history | No | 1 | 1 | 1 | 1 |
| Yes | 3.53 (1.88–6.63) | 2.13 (1.04–4.40) | 2.34 (1.15–4.76) | 2.37 (1.17–4.82) | |
| Degenerative changec | No | 1 | 1 | 1 | 1 |
| Yes | 2.35 (1.36–4.07) | 2.33 (1.26–4.33) | 2.16 (1.17–4.01) | 2.34 (1.27–4.33) | |
| Job types | Support | 1 | 1 | - | - |
| Dead-line | 0.57 (0.27–1.19) | 0.62 (0.28–1.39) | - | - | |
| Live-line | 1.56 (0.90–2.73) | 2.10 (1.12–3.92) | - | - | |
| Insulating stick use/week | None | 1 | - | 1 | - |
| < 10 hours | 1.41 (0.78–2.55) | - | 1.73 (0.90–3.34) | - | |
| ≥ 10 hours | 2.12 (1.21–3.71) | - | 2.46 (1.32–4.61) | - | |
| Neck flexion workd | Low (< 6) | 1 | - | - | 1 |
| High (≥ 6) | 2.22 (1.28–3.83) | - | - | 1.45 (0.77–2.72) | |
| Neck extension workd | Low (< 6) | 1 | - | - | 1 |
| High (≥ 6) | 2.31 (1.39–3.81) | - | - | 1.98 (1.14–3.46) | |
Table 1 Participant characteristics by job types
Values are presented as number (%).
SD: standard deviation.
aDepression: Patient Health Questionnaire-2 score 3 or higher; bDegenerative change: children's depression inventory score of moderate or higher in more than one cervical joint; cExposure score: low—exposure score below 6, high—exposure score 6 or higher; dNeck disability: Neck Disability Index score moderate or higher.
Table 2 Prevalence of neck disabilitya
Values are presented as number (%).
aNeck disability: moderate to high Neck Disability Index score; bDepression: Patient Health Questionnaire-2 score 3 or higher; cDegenerative change: children's depression inventory score of moderate or higher in more than one cervical joint; dExposure score: low—exposure score below 6, high—exposure score 6 or higher.
Table 3 Logistic regression analysis of relative factors for neck disabilitya
Bolds are presented as statistically significance.
OR: odds ratio; CI: confidence interval.
aNeck disability: moderate to high Neck Disability Index score; bDepression: Patient Health Questionnaire-2 score 3 or higher; cDegenerative change: children's depression inventory score of moderate or higher in more than one cervical joint; dExposure score: low—exposure score below 6, high—exposure score 6 or higher.

