
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 28; 2016 > Article
- Research Article The effect of long working hours on 10-year risk of coronary heart disease and stroke in the Korean population: the Korea National Health and Nutrition Examination Survey (KNHANES), 2007 to 2013
- Dong-Wook Lee1, Yun-Chul Hong1,2, Kyoung-Bok Min1, Tae-Shik Kim1, Min-Seok Kim1, Mo-Yeol Kang1,2
-
Annals of Occupational and Environmental Medicine 2016;28:64.
DOI: https://doi.org/10.1186/s40557-016-0149-5
Published online: November 15, 2016
1Department of Preventive Medicine, College of Medicine, Seoul National University, 103 Daehangno, Jongno-gu, Seoul, 110-799 Republic of Korea
2Institute of Environmental Medicine, Seoul National University Medical Research Center, 103 Daehangno, Jongno-gu, Seoul, 110-799 Republic of Korea
• Received: May 18, 2016 • Accepted: November 7, 2016
© The Author(s). 2016
Open AccessThis article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Abstract
-
Background Recently, the emergence of long working hours and the associated conditions such as coronary heart disease (CHD) and stroke have gained attention. The aim of this study was to investigate the association between long working hours and the 10-year-risk of CHD and stroke, estimated by Jee’s health risk-appraisal model for ischemic heart disease.
-
Methods We analyzed data from Koreans who randomly enrolled in Korean National Health and Nutrition Examination Survey 2008–2012 and finally included 13,799 participants. The participants were classified as per their working hours: 0–30 h/week, 31–39 h/week, 40 h/week, 41–50 h/week, 51–60 h/week, 61–70 h/week, 71–80 h/week, and >80 h/week. The risks for CHD and stroke were determined using Jee’s health risk-appraisal model. Multiple logistic regression was used to analyze the association between working hours and 10-year risk for CHD.
-
Results The 10-year risks for CHD and stroke were significantly and positively associated with working hours in both men and women. Furthermore, higher risks for CHD and stroke were associated with longer working hours in women.
-
Conclusion Long working hours are significantly associated with the risks of CHD and stroke, estimated by Jee’s health risk-appraisal model. This study suggests the need for proper management of working hours to reduce CHD risk and stroke risk in the Korean population.
-
Electronic supplementary material The online version of this article (doi:10.1186/s40557-016-0149-5) contains supplementary material, which is available to authorized users.
Background
Long working hours can cause health problems such as hypertension, musculoskeletal discomfort, diabetes, occupational injury, increased suicide rate, sleep problems, preterm birth, poor psychological health, and unhealthy lifestyle conditions [1, 2]. Recently, the emergence of long working hours and the associated conditions such as coronary heart disease (CHD) and stroke, have gained attention [3–6]. However, the association of long working hours with CHD and stroke has not yet been clearly established. A recently published meta-analysis study reported that long working hours could be associated with CHD, but evidence for a dose-response relationship between working hours and CHD was insufficient, despite sufficient evidence for its association with stroke [7].
In the Korean population, studies have shown that long working hours may increase the risk of CHD, especially in people who work extremely long hours [8]. However, a limitation of this study was the use of the Framingham equation to determine the 10-year risk; this equation is derived from the participants mainly comprising middle-income Caucasians.
However, the risk could be overestimated in Asian population when estimating the risk by the Framingham equation model [9]. Ahn et al. suggested that the Framingham equation model overestimates the risk of ischemic heart disease in the Korean population [10]. Therefore, estimation of the accurate risks of CHD and stroke is warranted to investigate the relationship of long working hours with CHD and stroke in Korea.
To overcome the limitation of the Framingham equation model in Korean populations, Jee et al. developed an individualized health risk-appraisal model for ischemic heart disease and stroke, by using well-known risk factors such as hypertension and hypercholesterolemia, using data derived from the Korean population. Outcomes were ascertained from data on the National Health Insurance Corporation claim and death certificate. They used Cox proportional hazard model when developing health-appraisal model to estimate the 10-year risk for ischemic heart disease and stroke. They applied split-half method that the first half of data was used for developing a model and the rest was used for testing for validity of models. This health-appraisal model accurately predicted the actual rates of events [11, 12]. The actual ischemic heart disease event rates were similar to the event rates predicted by the Korean risk prediction model for ischemic heart disease [13].
The primary aim of this study was to investigate the association between long working hours and risks of CHD and stroke estimated by Jee’s health risk-appraisal model. In this assessment, differences between genders were taken in account. Considering that the risks of CHD and stroke are preventable, it is important to understand the characteristics of these events, specific risk factors, and populations at risk. Therefore, this study also aimed to identify specific risk factors for CHD and stroke, which may be associated with working hours.
Methods
The current study used data derived from the Korean National Health and Nutrition Examination Survey (KNHANES) 2007–2013. The KNHANES is a cross-sectional, nationally representative survey, conducted by the Korean Centers for Disease Control and Prevention (KCDC). Multistage probability sampling, stratified according to geographic location, gender, and age, was used. It collects information about the participants’ socioeconomic status, anthropometric measures, health interview, health examination, and nutrition survey. All participants of the KNHANES used in the current study provided written informed consent. This nationwide survey was approved by the Institutional Review Board (IRB) of the KCDC (IRB: 2007-02-CON-04-P; 2008-04EXP-01-C; 2009-01CON-03-2C; 2010-02CON-21-C; 2011-02CON-06-C; 2012-01EXP-01-2C; 2013-07CON-03-4C).
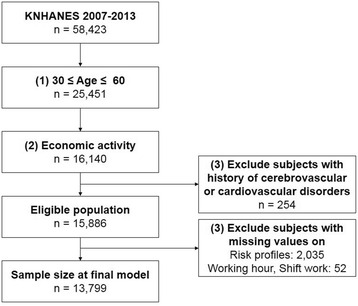
In total, 58,423 individuals (24,871 individuals from the 4th KNHANES, 25,534 individuals from the 5th KNHANES, and 8,018 individuals from the 6th KNHANES) participated in the surveys. For our analysis, we excluded participants who were younger than 30 years of age and older than 60 years of age. Because Jee’s health-appraisal models for CHD and stroke were developed using Korean individuals between the age of 30 years - 60 years of age, we only included those age groups in our analysis (n = 32,972). Subjects who were unemployed or lacked information on economic activity (n = 9,311) as well as subjects with a history of cerebrovascular or cardiovascular disorders (n = 254) were excluded. The risk for CHD was calculated by combining 8 risk factors, and the risk for stroke was calculated by combining 8 risk factors. Subjects with missing values were also excluded (2,035 subjects were eliminated due to absence of one value for these risk factors and 52 subjects were eliminated due to missing information on shift work or working hours). Finally, of 15,886 eligible participants, the final sample size for analysis was 13,799 (7,565 men and 6,234 women) after excluding subjects with missing values (Fig. 1).
The KNHANES survey included questions about a wide array of characteristics. We used the following variables: age, gender, occupation-related variables, chronic disease diagnosis, and health behaviour. Completed questionnaires were reviewed by trained staff and entered into a database.
Working hours were measured as the actual number of hours the respondent worked per week without mealtime at all jobs. According to the Korean labour law, standard working hours are 40 h/week, and the reference group included people who worked 40 h/week. Working-hour groups were defined as 0–30 h/week, 31–39 h/week, 40 h/week, 41–50 h/week, 51–60 h/week, 61–70 h/week, 71–80 h/week, and >80 h/week. Occupations were classified into 6 groups: “managers and professionals,” “office workers,” “service and sales workers,” “agriculture, forestry and fisheries workers,” “craft, device, and machine operators, and assembly workers,” and “manual workers.” Daytime work is a full-time schedule in which subjects usually worked between 6 am and 6 pm, excluding rotators. The shift-work group included any schedule other than daytime work such as day-night shift, fixed night, regular rotation, 24-h shift, split shift, and irregular shifts. Smoking status was categorized as non-smoker, ex-smoker, and current smoker. In order to estimate the risk with Jee’s health-appraisal model, the alcohol consumption level at the interview was calculated as consumed alcohol in grams per day. Physical inactivity was defined as engaging in ≥10 min of mild physical activity less than 5 times per week.
Height and weight were measured during the physical examination. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared. BMI was classified into 2 groups: <25 kg/m2 and ≥25 kg/m2. Blood pressure (BP) was measured in the right arm at the level of the heart using a standard mercury sphygmomanometer (Baumanometer; WA Baum, Copiague, NY, USA) while the subjects were seated and after they had rested for 5 min. The average of 2 systolic and diastolic blood pressure (SBP and DBP, respectively) readings, which were recorded at an interval of 5 min, was used for analysis. After a 12-h overnight fast, blood samples were obtained from the subjects through an antecubital vein. Total cholesterol (TC) and high-density lipoprotein (HDL) were measured using an ADVIA 1650 autoanalizer (Bayer, Tarrytown, NY, USA) from 2007 to 2008, and Hitachi Automatic Analyzer 7600 (Hitachi, Japan) from 2009 to 2012. Therefore, we used the corrected value of HDL by using conversion formula suggested by KCDC. The participants were considered to have diabetes mellitus (DM) if they met one of the following conditions: (1) fasting plasma glucose level ≥ 126 mg/dL, (2) medical diagnosis of DM by a trained medical professional, or (3) treatment with oral hypoglycemic agents or insulin injections.
Individuals’ risk for CHD was determined using Jee’s health risk-appraisal model for ischemic heart disease, which is based on data collected nationwide from health screenings, cause of death statistics, and insurance claims. This is the first CHD risk-prediction model in Korea that incorporated risk predictors of age, TC, HDL, SBP, DBP, smoking status, and diabetes by gender. After development, the model was validated in another random sample representative of the Korean population. Individuals’ 10-year risk for stroke was also estimated using Jee’s health risk-appraisal model for stroke, which is based on similar methods of the model for CHD. This model estimated the 10-year risk of stroke in Koreans by using age, SBP, diabetes, smoking status, physical inactivity, BMI, alcohol consumption, and total cholesterol by gender. To estimate the future risk of CHD and stroke, we calculated the number of points for each risk factor, after which the individual’s 10-year risk was computed using risk functions for Korean men and women, separately. As both model for CHD and model for stroke was validated by comparing actual event and prediction of event according to decile of predicted risk in each sex, we defined cases as high-risk group when the each risk was ≥90 percentile in each sex. To evaluate the association between weekly working hours and high risk for CHD, and weekly working hours and high risk for stroke, the odds ratios (ORs) and 95% confidence intervals (CIs) were calculated after adjustment for household income, employment condition, occupation, and work shift.
The basic characteristics were described by means and standard deviation (SD) or frequencies with percentages for men and women, separately. Risk profiles used for estimating risks for CHD and stroke were presented as means and SD, and categorical values were presented as frequencies and percentage by each gender. First, we performed nonparametric analyses of the associations between weekly working hours and 10-year risks for CHD and stroke to visualize the association. After adjustment for household income, employment condition, occupation, and shift work, generalized additive models considering Poisson distribution were constructed for each outcome using the gam package of R version 2.12.2 (R Foundation for Statistical Computing, Vienna, Austria). Subsequently, the average 10-year risks for CHD and stroke by working-hour schedule were calculated for each gender. Finally, multiple logistic regression was conducted to assess the association between working hours and 10-year risks for CHD and stroke, estimated by Jee’s health risk-appraisal model. As these risks differ according to weekly working hours, we compared the 40 h/week group (reference group) with other working-hour groups. As the risk function used to estimate 10-year risks for CHD and stroke already considered age, SBP, and any other risk profiles, these variables were not used for adjusting variables. After adjustment for household income, employment condition, occupation, work shift, and weekly working hours, multiple logistic regression was performed using PROC LOGISTIC of SAS version 9.3 (SAS Institute, Cary, NC, USA). Two-tailed p-values < 0.05 were considered statistically significant. Additionally, the nonparametric analyses to visualize the association and multiple logistic regression were performed by stratifying 2 age group: <45y and ≥45y.
Results
Table 1 shows the occupational characteristics of the study population. Among the 13,799 participants, 7,565 (54.8%) were men and 6,234 (45.2%) were women. The proportion of paid workers was 61.7% among men and 61.5% among women. In addition, among women, 13.7% were unpaid family workers. In both male and female subjects, <25% of the subjects did shift work, and 25.1% of male and 17.3% of female subjects worked >60 h/week.
Table 1
Characteristics of the study population
A summary of the each component for Jee’s health risk-appraisal model according to weekly working hours for each gender is presented in Table 2. The mean age (SD) of the male and female subjects was 44.56 (±8.43 SD) and 45.22 (±8.26 SD) years. The levels of TC were similar in men and women, while the BP was slightly lower in women. Likewise, the other risk factors for CHD, such as prevalence of diabetes, current smoking, and alcohol consumption were higher among male subjects than among female subjects. Generally, the level of each variable increased as the weekly work hours increased from 40 h/week to >80 h/week, while those who worked 30–40 h/week and <30 h/week showed higher values than those who worked 40 h/week.
Table 2
Cardiovascular and stroke risk profiles
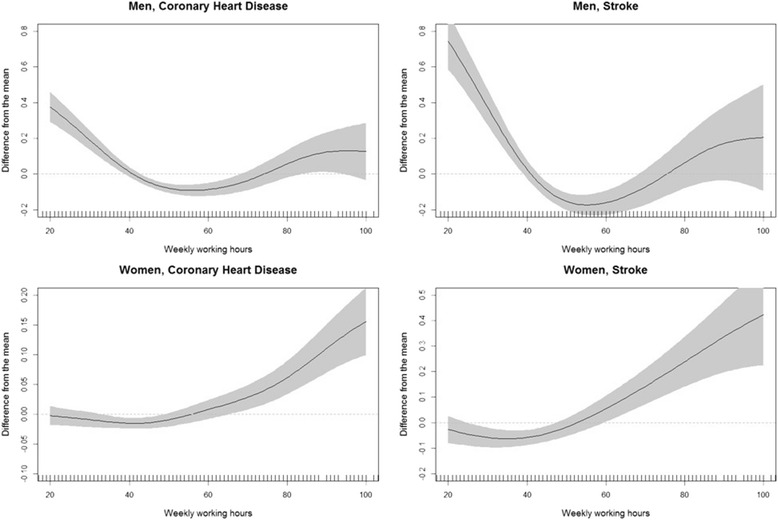
The nonparametric associations between weekly working hours and 10-year risks for CHD and stroke were evaluated for each gender (Fig. 2). Ten-year risks of both CHD and stroke increased with increasing weekly working hours in subjects working >50 h/week, while decreased with increasing weekly working hours in subjects working <40 h/week.
The risk of CHD and stroke, estimated by Jee’s health risk-appraisal model, is presented according to weekly working hours in Table 3. The average risk of CHD predicted by Jee’s model was 1.11% and 0.26% in male and female subjects, respectively, and that of stroke was 1.97% and 1.45% in male and female subjects, respectively. On comparing those who worked 40 h/week and those who worked >80 h/week, the ORs for high risk of CHD were 1.76 (95% CI: 1.23–2.52) in men and 1.63 (95% CI: 1.03–2.58) in women. The ORs for high risk of stroke were 1.49 (95% CI: 1.03–2.16) in women who worked between 50 and 60 h/week and 2.32 (95% CI: 1.46–3.69) in women who worked >80 h/week, as compared to women who worked 40 h/week. Trend tests were performed after excluding participants who worked <40 h/week. A statistically significant dose-response relationship was found between weekly working hours and high risk for stroke among female subjects.
Table 3
Odds ratios for high 10-year risk of CHD and stroke
In stratified analysis by age, the nonlinear association was weaker in younger age group (<45y), while similar in older age group (≥45y) (Additional file 1: Figure S1, S2). Long working hours (80 h/week) were associated with the high risk of CHD in men (OR: 1.85, 95% CI: 1.25–2.75) and associated with the high risk of stroke in women (OR: 1.65, 95% CI: 1.01–2.67) (Additional file 2: Table S1).
Discussion
The results of our study show that the 10-year risks for CHD and stroke were significantly associated with working hours. Furthermore, higher risks for CHD and stroke were associated with longer working hours in women. Among the male participants, compared to those who worked 40 h/week, the longest working-hour group showed statistically significant differences in high risk for CHD. However, no such difference was found high risk for stroke. In addition, among female participants, the longest working-hour group showed higher OR for both CHD and stroke.
After stratified by age group, the nonparametric analyses in older age group (≥45y) were consistent with the analyses in main result, while the nonparametric analyses in younger age group (<45y) show weaker association in younger age group. Among older age group, it was statistically significant that the association between the longest working-hours and the risk of CHD in men and between the longest working-hours and the risk of stroke in women.
In our study, compared to the regular working hours, the ORs of high risk for CHD in the longest working-hour group (≥80 h/week) were 1.76 in men and 1.63 in women and were statistically significant. Although our results shows significant associations only in longest working-hour group, these results are in line with those of previous studies, which reported an association between long working hours and CHD. A meta-analysis study concluded that longer working hours was related with the risk of CHD with an OR of 1.37 [14]. Another meta-analysis of 4 prospective studies reported a relative risk of 1.39 for long working hours on CHD [4]. However, recent meta-analysis of large data performed by Kivimaki et al. reported that there was no statistically significant association between working 55 h per week or longer and coronary heart disease [7]. Further studies to investigate how long working hours is associated with coronary heart disease are necessary.
Although several studies have reported an association between long working hours and CHD risk, only a few studies have investigated the association between long working hours and stroke. For example, in a census-based longitudinal study in the United Kingdom, O’reilly and Rosato reported that those who worked ≥55 h/week showed a higher risk of stroke, but the difference was not statistically significant [5]. In the Korean population, however, a case-control study of 940 cases of incident hemorrhagic stroke concluded that longer regular working time and extended duration of strenuous activity during work could increase the risk of hemorrhagic stroke [15]. Recent multi-national studies using unpublished studies reported that long working hours was associated with stroke in a dose-response relationship. We also found a statistically significant association between long working hours and stroke. The ORs for stroke in the longest working-hour group were remarkable (1.22 in men and 1.48 in women), but statistically significant values were found only in women.
We defined high risks for CHD and stroke when the risk for each disease was higher than or equal to the 90th percentile of risk in each gender while considering differences in the risk-estimating methods and risk profiles, and weekly working hours as per gender. Among women, longer working hours showed a statistically significant association with the risk for stroke and marginally significant association with the risk for CHD (p for trend = 0.01 and 0.06, respectively). However, we did not find any such statistically significant association among men. It is possible that these contrasting findings reflect gender differences in influences on the cardiovascular system according to social role. Incomplete recovery from work is known to be associated with death by cardiovascular disease and the employee’s imbalance between work and family responsibilities. Complete recovery away from the workplace is an important component for preventing CHD and stroke [16, 17]. In eastern countries, married women are expected to do unpaid family work such as childcare, cleaning, preparing meals, and caring for elders, regardless of the individual’s working condition. In these cultures, female employees who work longer hours could be overloaded with unpaid family work. These excessive demands could cause excessive stress or lack of time spent on health promotion.
The results of the generalized additive model to nonlinear association suggest a difference in the direction of the association between participants who worked <40 h/week and those who worked ≥40 h/week. Furthermore, we observed a positive association between reduced working hours (<30 h/week) and risk of CHD and stroke in men, and between reduced working hours and risk of stroke in women. One possible explanation of the result is that the workers working less than 40 h per week, which is legal working hours in the Korea, may have inferior socioeconomic status and working condition comparing to the workers working 40 h or longer. Those who have short working hours per week are probably precarious workers and non-regular workers in the Korea, and they could have relatively large work stress from their position [18]. Another explanation may be that selection process between those who works longer hours and those who works reduced hours. In our study, participants with short working hours had higher SBP, DBP, total cholesterol level, physical inactivity, diabetes prevalence. It means that the possibility that those who reduced working hours had poorer health status than those who works general hours (40 h/week) or long hours. As people who have disease would not work long hours, health problem could affect how long time people works. Unfortunately, our cross-sectional study design cannot identify in which direction the selection process between working hours and risks for CHD and stroke may have occurred. Therefore, further studies with a longitudinal design are needed.
Several studies have suggested that long working hours are positively correlated with risk factors for CHD and stroke. The association between work hours and self-reported hypertension has been reported in California [19]. In Japan, increased BP and heart rate were reported among those who periodically worked overtime [20]. In a meta-analysis, a positive association between longer working hours and type 2 diabetes was reported [21]. An individual’s lifestyle such as smoking or frequent drinking was also associated with longer working hours [22, 23]. In our study, we observed higher SBP and DBP among subjects with longer working hours in both men and women (Table 2). Higher TC, higher prevalence of diabetes, and higher prevalence of smoking were seen in those with longer working hours. Compared to those who worked 40 h/week and those who worked ≥80 h/week, the prevalence of diabetes (8.53% vs. 13.25%, respectively) and the percentage of smokers (43.81% vs. 51.51%, respectively) showed significant differences among men, whereas the TC (184.69 mg/dl vs. 199.32 mg/dl, respectively), body mass index (23.05 kg/m2 vs. 24.50 kg/m2, respectively), and prevalence of diabetes (4.49% vs. 7.11%) showed significant differences among women.
Regarding its association with CHD and stroke, working hours could affect an individual’s health through various mechanisms. First, the person’s physical recovery may remain incomplete. Long working hours are associated with reduced time for recovery and limited relaxation time after work. Chronic health impairment could be caused by incomplete physical recovery due to prolonged exposure to work demands such as long working hours [24]. An effect-recovery model suggested that work effort draws upon one’s resources, thereby causing strain reaction [25]. Considering that long working hours could be associated with high job demands, employees who spend more time in the workplace could be restrained and may not be able to avail of appropriate relaxation time to reduce their strain [26, 27]. Second, work-life imbalance could be caused by long working hours. Bad family relationships are have been shown to be associated with sickness-related absence, psychological distress, and poor health [28]. These associations may be more important to Korean women who tend to be the primary care-giver of the family. As such, long working hours could have a larger effect on women’s health because of the domestic burden. In our study, women showed a dose-response relationship between weekly working hours and risks for CHD and stroke (Table 3). Similarly, in Japan, long working hours was associated with poor social dysfunction and poor general health among female factory employees [29]. Third, long working hours could adversely affect an individual’s health, causing physical inactivity, longer time spent in the sitting position, or risky drinking, which are risk factors for CHD or stroke [30–32].
Our study has some strengths. As the results were derived from a representative sample of the general Korean population, we could investigate the population with better variance by using a large sample size with longer working hours than that used in other studies. In addition, by using Jee’s health-appraisal model that was developed and validated in the Korean population for predicting 10-year risk for CHD and stroke, we could more accurately predict the risk as compared to previous studies. Moreover, accurate measurements of BP, TC, and HDL support the validity of the estimated 10-year risks for CHD and stroke.
Despite these strengths, there are limitations to this study. The results from the cross-sectional data preclude us from commenting on causal inferences. To overcome this issue, a longitudinal study design using established outcomes as recorded CHD or stroke event should be performed. Furthermore, we could not consider other factors that may affect the association between working hours, and CHD and stroke, such as job-demand level, poor mental health, and social support. Considering these limitations, further studies are required to confirm our findings.
Conclusion
Long working hours increase the risks of CHD and stroke. These associations were more significantly observed among women than men, especially for the risk of stroke. These results suggest the need for proper management of working hours to reduce the incidence of CHD and stroke in the Korean population. We hope that this study will contribute to the improvement in labor management and reduce the risks of CHD and stroke that are associated with long working hours.
Acknowledgement
Youn-hee Lim contributed to consultation for analysis of data.
We have nothing to declare.
KNHANES data are available on the KNHANES website (http://knhanes.cdc.go.kr).
D-WL and M-Y K designed the study; D-WL acquired the data; D-W L and M-Y K analyzed data and wrote the manuscript; Y-C H, K-B M, T-SK, M-SK, and M-Y K critically revised the manuscript. All authors read and approved the final manuscript.
The authors declare that they have no competing interests.
Obtained.
All participants of the KNHANES used in the current study provided written informed consent. This nationwide survey was approved by the Institutional Review Board (IRB) of the KCDC (IRB: 2007-02-CON-04-P; 2008-04EXP-01-C; 2009-01CON-03-2C; 2010-02CON-21-C; 2011-02CON-06-C; 2012-01EXP-01-2C; 2013-07CON-03-4C).
Abbreviations
BMI
Body mass index
BP
Blood pressure
CHD
Coronary heart disease
DBP
Diastolic blood pressure
DM
Diabetes mellitus
HDL
High-density lipoprotein
KCDC
Korean centers for disease control and prevention
KNHANES
Korean national health and nutrition examination survey
SBP
Systolic blood pressure
TC
Total cholesterol
- 1.
- 2. Sparks K, Cooper C, Fried Y, Shirom A. The effects of hours of work on health: a meta‐analytic review. J Occup Organ Psychol 1997;70(4):391–408. 10.1111/j.2044-8325.1997.tb00656.x.Article
- 3. Holtermann A, Mortensen OS, Burr H, Søgaard K, Gyntelberg F, Suadicani P. Long work hours and physical fitness: 30-year risk of ischaemic heart disease and all-cause mortality among middle-aged Caucasian men. Heart 2010;96(20):1638–44. 10.1136/hrt.2010.197145. 20820054.ArticlePubMed
- 4. Virtanen M, Heikkilä K, Jokela M, Ferrie JE, Batty GD, Vahtera J, et al. Long working hours and coronary heart disease: a systematic review and meta-analysis. Am J Epidemiol 2012;176(7):586–96. 10.1093/aje/kws139. 22952309.ArticlePubMedPMC
- 5. O’reilly D, Rosato M. Worked to death? A census-based longitudinal study of the relationship between the numbers of hours spent working and mortality risk. Int J Epidemiol 2013;42(6):1820–30. 10.1093/ije/dyt211. 24415615.ArticlePubMed
- 6. Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2013;380(9859):2224–60. 10.1016/S0140-6736(12)61766-8.
- 7. Kivimäki M, Jokela M, Nyberg ST, Singh-Manoux A, Fransson EI, Alfredsson L, et al. Long working hours and risk of coronary heart disease and stroke: a systematic review and meta-analysis of published and unpublished data for 603 838 individuals. Lancet 2015;386(10005):1739–46. 10.1016/S0140-6736(15)60295-1. 26298822.ArticlePubMed
- 8. Kang MY, Cho SH, Yoo MS, Kim T, Hong YC. Long working hours may increase risk of coronary heart disease. Am J Ind Med 2014;57(11):1227–34. 10.1002/ajim.22367. 25164196.ArticlePubMed
- 9. D'Agostino RB Sr, Grundy S, Sullivan LM, Wilson P. Validation of the Framingham coronary heart disease prediction scores: results of a multiple ethnic groups investigation. JAMA 2001;286(2):180–7. 10.1001/jama.286.2.180. 11448281.ArticlePubMed
- 10. Ahn KA, Yun JE, Cho ER, Nam CM, Jang Y, Jee SH. Framingham equation model overestimates risk of ischemic heart disease in Korean men and women. Korean J Epidemiol 2006;28(2):162–70.
- 11. Jee SH, Park JW, Lee S-Y, Nam B-H, Ryu HG, Kim SY, et al. Stroke risk prediction model: a risk profile from the Korean study. Atherosclerosis 2008;197(1):318–25. 10.1016/j.atherosclerosis.2007.05.014. 17586511.ArticlePubMed
- 12. Jee SH, Jang Y, Oh DJ, Oh B-H, Lee SH, Park S-W, et al. A coronary heart disease prediction model: the Korean Heart Study. BMJ Open 2014;4(5):e005025. 10.1136/bmjopen-2014-005025. 24848088.ArticlePubMedPMC
- 13. Jung KJ, Jang Y, Oh DJ, Oh B-H, Lee SH, Park S-W, et al. The ACC/AHA 2013 pooled cohort equations compared to a Korean Risk Prediction Model for atherosclerotic cardiovascular disease. Atherosclerosis 2015;242(1):367–75. 10.1016/j.atherosclerosis.2015.07.033. 26255683.ArticlePubMed
- 14. Kang M-Y, Park H, Seo J-C, Kim D, Lim Y-H, Lim S, et al. Long working hours and cardiovascular disease: a meta-analysis of epidemiologic studies. J Occup Environ Med 2012;54(5):532–7. 10.1097/JOM.0b013e31824fe192. 22576460.PubMed
- 15. Kim BJ, Lee SH, Ryu WS, Kim CK, Chung JW, Kim D, et al. Excessive work and risk of haemorrhagic stroke: a nationwide case‐control study. Int J Stroke 2013;8(A100):56–61. 10.1111/j.1747-4949.2012.00949.x. 23227896.ArticlePubMedPDF
- 16. Kivimäki M, Leino-Arjas P, Kaila-Kangas L, Luukkonen R, Vahtera J, Elovainio M, et al. Is incomplete recovery from work a risk marker of cardiovascular death? Prospective evidence from industrial employees. Psychosom Med 2006;68(3):402–7. 10.1097/01.psy.0000221285.50314.d3. 16738071.ArticlePubMed
- 17. Berg P, Kalleberg AL, Appelbaum E. Balancing work and family: The role of high‐commitment environments. Ind Relat 2003;42(2):168–88. 10.1111/1468-232X.00286.Article
- 18. Jang T-W, Kim H-R, Lee H-E, Myong J-P, Koo J-W. Long work hours and obesity in Korean adult workers. J Occup Health 2013;55(5):359–66. 10.1539/joh.13-0043-OA. 23892643.ArticlePubMedPDF
- 19. Yang H, Schnall PL, Jauregui M, Su T-C, Baker D. Work hours and self-reported hypertension among working people in California. Hypertension 2006;48(4):744–50. 10.1161/01.HYP.0000238327.41911.52. 16940208.ArticlePubMed
- 20. Hayashi T, Kobayashi Y, Yamaoka K, Yano E. Effect of overtime work on 24-hour ambulatory blood pressure. J Occup Environ Med 1996;38(10):1007–11. 10.1097/00043764-199610000-00010. 8899576.ArticlePubMed
- 21. Kivimäki M, Virtanen M, Kawachi I, Nyberg ST, Alfredsson L, Batty GD, et al. Long working hours, socioeconomic status, and the risk of incident type 2 diabetes: a meta-analysis of published and unpublished data from 222 120 individuals. Lancet Diabetes Endocrinol 2015;3(1):27–34. 10.1016/S2213-8587(14)70178-0. 25262544.ArticlePubMedPMC
- 22.
- 23. Cho Y-S, Kim H-R, Myong J-P, Kim HW. Association between work conditions and smoking in South Korea. Saf Health Work 2013;4(4):197–200. 10.1016/j.shaw.2013.09.001. 24422175.ArticlePubMedPMC
- 24.
- 25. Meijman TF, Mulder G, Drenth P, Thierry H. In: Drenth PJD, Thierry H, editors. Psychological aspects of workload. Handbook of work and organizational psychology: Work psychology. 1998, Hove: Psychology Press; 5–33.
- 26. In: Rissler A, editor. Stress reactions at work and after work during a period of quantitative overload. Ergonomics. 1977, London: Taylor & Francis Ltd One Gunpowder Square.
- 27. Spurgeon A, Harrington JM, Cooper CL. Health and safety problems associated with long working hours: a review of the current position. Occup Environ Med 1997;54(6):367–75. 10.1136/oem.54.6.367. 9245942.ArticlePubMedPMC
- 28. Väänänen A, Kevin MV, Ala-Mursula L, Pentti J, Kivimäki M, Vahtera J. The double burden of and negative spillover between paid and domestic work: associations with health among men and women. Women Health 2005;40(3):1–18. 10.1300/J013v40n03_01.Article
- 29. Ezoe S, Morimoto K. Behavioral lifestyle and mental health status of Japanese factory workers. Prev Med 1994;23(1):98–105. 10.1006/pmed.1994.1014. 8016040.ArticlePubMed
- 30. Virtanen M, Jokela M, Nyberg ST, Madsen IE, Lallukka T, Ahola K, et al. Long working hours and alcohol use: systematic review and meta-analysis of published studies and unpublished individual participant data. BMJ 2015;350:g7772. 10.1136/bmj.g7772. 25587065.ArticlePubMedPMC
- 31. Kumar A, Prasad M, Kathuria P. Sitting occupations are an independent risk factor for Ischemic stroke in North Indian population. Int J Neurosci 2014;124(10):748–54. 10.3109/00207454.2013.879130. 24397501.ArticlePubMed
- 32. Schneider S, Becker S. Prevalence of physical activity among the working population and correlation with work-related factors: results from the first German National Health Survey. J Occup Health 2005;47(5):414–23. 10.1539/joh.47.414. 16230835.ArticlePubMedPDF
REFERENCES
Appendix
Additional files
Additional file 1: Figure S1.
Nonlinear association between weekly working hours, risk for CHD, and risk for stroke, stratified by age (<45y). Figure S2. Nonlinear association between weekly working hours, risk for CHD, and risk for stroke, stratified by age (≥45y). (DOCX 463 kb)
Additional file 2: Table S1.
Odds ratios for high 10-year risk of CHD and stroke among participants ≥ 45y. (DOCX 35 kb)
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Dose–response association of total and leisure-time physical activity with the risk of different subtypes of stroke: a systematic-review and meta-analysis
Yujia Liu, Xudong Ya, Linlin Zhou, Tong Chen, Fei Shen, Yu Chen, Xingqi Wang
Journal of Public Health.2025; 47(3): 567. CrossRef - Long Working Hours and Dyslipidemia: A Systematic Review and Meta-analysis
Chan Young Lee, Seung Yeon Jeon, Joonho Ahn, Ji-Hun Song, Mo-Yeol Kang
Safety and Health at Work.2025; 16(3): 268. CrossRef - Tipping the scales: how paid work hours thresholds impact health and gender wage disparities
Sunjin Pak, Amit Kramer, Yun-Kyoung Kim
The International Journal of Human Resource Management.2025; 36(13): 2342. CrossRef - Barriers and enablers of pelvic floor rehabilitation behaviours in pregnant women with stress urinary incontinence: a qualitative analysis using the theoretical domains framework
Ping Xu, Ying Jin, Pingping Guo, Xuefen Xu, Xiaojuan Wang, Wei Zhang, Minna Mao, Suwen Feng
BMC Pregnancy and Childbirth.2023;[Epub] CrossRef - Poor worker’s long working hours paradox: evidence from the Korea National Health and Nutrition Examination Survey, 2013-2018
Min Young Park, Jaeyoung Park, Jun-Pyo Myong, Hyoung-Ryoul Kim, Dong-Wook Lee, Mo-Yeol Kang
Annals of Occupational and Environmental Medicine.2022;[Epub] CrossRef - Primary Exploration of Efficacy of Community-Family Management Mode under Internet-Based Mobile Terminal Monitoring in Elderly Patients with Stable Coronary Heart Disease
Xiang Li, Wenwu Zheng, Jinsong Li, Yibin Gao, Qiang Lin, Jinfeng Yang, Shuiying Huang, Defang Wang, Bin Wang, Bhagyaveni M.A
Journal of Healthcare Engineering.2022; 2022: 1. CrossRef - An Index to Assess Overwork-Related Adverse Effects on Employees Under the Occupational Safety and Health Act in Taiwan
Yu-Cheng Lin, Yu-Wen Lin
Safety and Health at Work.2022; 13(4): 401. CrossRef - Long Working Hours and Risk of Nonalcoholic Fatty Liver Disease: Korea National Health and Nutrition Examination Survey VII
Eyun Song, Jung A. Kim, Eun Roh, Ji Hee Yu, Nam Hoon Kim, Hye Jin Yoo, Ji A. Seo, Sin Gon Kim, Nan Hee Kim, Sei Hyun Baik, Kyung Mook Choi
Frontiers in Endocrinology.2021;[Epub] CrossRef - The combined effect of long working hours and individual risk factors on cardiovascular disease: An interaction analysis
Wanhyung Lee, Jongin Lee, Hyoung-Ryoul Kim, Yu Min Lee, Dong-Wook Lee, Mo-Yeol Kang
Journal of Occupational Health.2021;[Epub] CrossRef - The Contribution of Material, Behavioral, Psychological, and Social-Relational Factors to Income-Related Disparities in Cardiovascular Risk Among Older Adults
Chiyoung Lee, Qing Yang, Eun-Ok Im, Eleanor Schildwachter McConnell, Sin-Ho Jung, Hyeoneui Kim
Journal of Cardiovascular Nursing.2021; 36(4): E38. CrossRef - The effect of exposure to long working hours on depression: A systematic review and meta-analysis from the WHO/ILO Joint Estimates of the Work-related Burden of Disease and Injury
Reiner Rugulies, Kathrine Sørensen, Cristina Di Tecco, Michela Bonafede, Bruna M. Rondinone, Seoyeon Ahn, Emiko Ando, Jose Luis Ayuso-Mateos, Maria Cabello, Alexis Descatha, Nico Dragano, Quentin Durand-Moreau, Hisashi Eguchi, Junling Gao, Lode Godderis,
Environment International.2021; 155: 106629. CrossRef - Occupations Associated With Poor Cardiovascular Health in Women
Bede N. Nriagu, Ako A. Ako, Conglong Wang, Anneclaire J. De Roos, Robert Wallace, Matthew A. Allison, Rebecca A. Seguin, Yvonne L. Michael
Journal of Occupational & Environmental Medicine.2021; 63(5): 387. CrossRef - Maternal working hours and smoking and drinking in adolescent children: based on the Korean National Health and Nutrition Examination Survey VI and VII
Tae-Hwi Park, Yong-Duk Ahn, Jeong-Bae Rhie
Annals of Occupational and Environmental Medicine.2021;[Epub] CrossRef - The interplay of sleep duration, working hours, and obesity in Korean male workers: The 2010–2015 Korea National Health and Nutrition Examination Survey
Mi-Jung Eum, Hye-Sun Jung, Leng Huat Foo
PLOS ONE.2021; 16(3): e0247746. CrossRef - Effect of Long Working Hours on Cardiovascular Disease in South Korean Workers: A Longitudinal Study
Soojung Kim, Youn Jung
Asia Pacific Journal of Public Health.2021; 33(2-3): 213. CrossRef - Association between Occupational Characteristics and Overweight and Obesity among Working Korean Women: The 2010–2015 Korea National Health and Nutrition Examination Survey
Mi-Jung Eum, Hye-Sun Jung
International Journal of Environmental Research and Public Health.2020; 17(5): 1585. CrossRef - A 10-year trend in income disparity of cardiovascular health among older adults in South Korea
Chiyoung Lee, Qing Yang, Eun-Ok Im, Eleanor Schildwachter McConnell, Sin-Ho Jung, Hyeoneui Kim
SSM - Population Health.2020; 12: 100682. CrossRef - Socioeconomic and demographic predictors of high blood pressure, diabetes, asthma and heart disease among adults engaged in various occupations: evidence from India
Sunita Patel, Usha Ram, Faujdar Ram, Surendra Kumar Patel
Journal of Biosocial Science.2020; 52(5): 629. CrossRef - Exploring Public Awareness of Overwork Prevention With Big Data From Google Trends: Retrospective Analysis
Ro-Ting Lin, Yawen Cheng, Yan-Cheng Jiang
Journal of Medical Internet Research.2020; 22(6): e18181. CrossRef - WHO/ILO work-related burden of disease and injury: Protocol for systematic reviews of exposure to long working hours and of the effect of exposure to long working hours on depression
Reiner Rugulies, Emiko Ando, Jose Luis Ayuso-Mateos, Michela Bonafede, Maria Cabello, Cristina Di Tecco, Nico Dragano, Quentin Durand-Moreau, Hisashi Eguchi, Junling Gao, Anne H. Garde, Sergio Iavicoli, Ivan D. Ivanov, Nancy Leppink, Ida E.H. Madsen, Fran
Environment International.2019; 125: 515. CrossRef - The Impact of Working Hours on Cardiovascular Diseases and Moderating Effects of Sex and Type of Work
Wanhyung Lee, Young Joong Kang, Taeshik Kim, Jaesung Choi, Mo-Yeol Kang
Journal of Occupational & Environmental Medicine.2019; 61(6): e247. CrossRef - Long working hours and stroke among employees in the general workforce of Denmark
Harald Hannerz, Karen Albertsen, Hermann Burr, Martin Lindhardt Nielsen, Anne Helene Garde, Ann Dyreborg Larsen, Jan Hyld Pejtersen
Scandinavian Journal of Public Health.2018; 46(3): 368. CrossRef - Cardiovascular disease risk differences between bus company employees and general workers according to the Korean National Health Insurance Data
Ji-Hoo Yook, Dong-Wook Lee, Min-Seok Kim, Yun-Chul Hong
Annals of Occupational and Environmental Medicine.2018;[Epub] CrossRef - The Change of Self-Rated Health According to Working Hours for Two Years by Gender
Jia Ryu, Yeogyeong Yoon, Hyunjoo Kim, Chung won Kang, Kyunghee Jung-Choi
International Journal of Environmental Research and Public Health.2018; 15(9): 1984. CrossRef - Long weekly working hours and ischaemic heart disease: a follow-up study among 145 861 randomly selected workers in Denmark
Harald Hannerz, Ann Dyreborg Larsen, Anne Helene Garde
BMJ Open.2018; 8(6): e019807. CrossRef - Working hours and all-cause mortality in relation to the EU Working Time Directive: a Danish cohort study
Harald Hannerz, Helle Soll-Johanning
European Journal of Public Health.2018; 28(5): 810. CrossRef - Study on association of working hours and occupational physical activity with the occurrence of coronary heart disease in a Chinese population
Yao Ma, Ying-Jun Wang, Bing-Rui Chen, Hao-Jie Shi, Hao Wang, Mohammad Reeaze Khurwolah, Ya-Fei Li, Zhi-Yong Xie, Yang Yang, Lian-Sheng Wang, Carmine Pizzi
PLOS ONE.2017; 12(10): e0185598. CrossRef
 Cite
CiteThe effect of long working hours on 10-year risk of coronary heart disease and stroke in the Korean population: the Korea National Health and Nutrition Examination Survey (KNHANES), 2007 to 2013
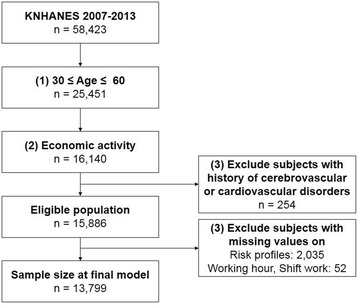
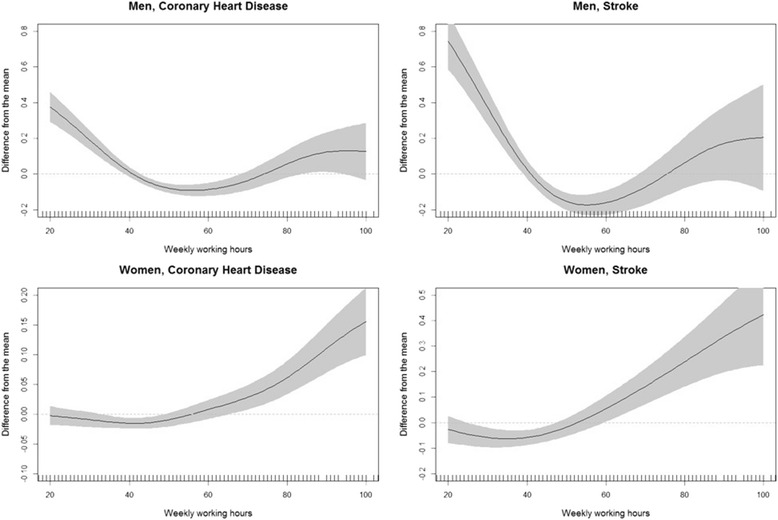
Fig. 1 Schematic diagram of the number of participants
Fig. 2 Nonlinear association between weekly working hours, risk for CHD, and risk for stoke in men and women
Fig. 1
Fig. 2
The effect of long working hours on 10-year risk of coronary heart disease and stroke in the Korean population: the Korea National Health and Nutrition Examination Survey (KNHANES), 2007 to 2013
| Men | Women | |||
|---|---|---|---|---|
| n | % | n | % | |
| Age (years) | ||||
| 30–39 | 2475 | 32.7 | 1785 | 28.6 |
| 40–49 | 2661 | 35.2 | 2249 | 36.1 |
| 50–60 | 2429 | 32.1 | 2200 | 35.3 |
| Education | ||||
| Below elementary school | 546 | 7.2 | 1041 | 16.7 |
| Middle school graduate | 771 | 10.2 | 872 | 14.0 |
| High school graduate | 2802 | 37.0 | 2487 | 39.9 |
| Above college graduate | 3446 | 45.6 | 1834 | 29.4 |
| Income status | ||||
| 1st Quartile | 437 | 5.8 | 545 | 8.7 |
| 2nd Quartile | 1733 | 22.9 | 1573 | 25.2 |
| 3rd Quartile | 2518 | 33.3 | 1993 | 32.0 |
| 4th Quartile | 2877 | 38.0 | 2123 | 34.1 |
| Employment condition | ||||
| Paid worker | 4671 | 61.7 | 3836 | 61.5 |
| Self-employed or employer | 2743 | 36.3 | 1547 | 24.8 |
| Unpaid family worker | 151 | 2.0 | 851 | 13.7 |
| Occupation | ||||
| Managers and professionals | 1822 | 24.1 | 1298 | 20.8 |
| Office workers | 1264 | 16.7 | 819 | 13.1 |
| Service and sales workers | 1193 | 15.8 | 2025 | 32.5 |
| Agriculture, forestry, and fishery workers | 576 | 7.6 | 553 | 8.9 |
| Craft, device, and machine operators and assembly workers | 2188 | 28.9 | 411 | 6.6 |
| Manual workers | 522 | 6.9 | 1128 | 18.1 |
| Work shift | ||||
| Fixed-day schedule | 6392 | 84.5 | 5144 | 82.5 |
| Any schedule other than fixed-day schedule* | 1173 | 15.5 | 1090 | 17.5 |
| Weekly working hours | ||||
| < 30 | 460 | 6.1 | 1357 | 21.8 |
| 30–40 | 649 | 8.6 | 974 | 15.6 |
| 40 | 1406 | 18.6 | 981 | 15.7 |
| 40–50 | 1567 | 20.7 | 1085 | 17.4 |
| 50–60 | 1587 | 21.0 | 757 | 12.1 |
| 60–70 | 1009 | 13.3 | 488 | 7.8 |
| 70–80 | 555 | 7.3 | 367 | 5.9 |
| ≥ 80 | 332 | 4.4 | 225 | 3.6 |
| Total | 7565 | 54.8 | 6234 | 45.2 |
| Weekly working hours | SBP | DBP | TC | HDL | Physical Inactivity | DM | Smoking | BMI | Drinking | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | n | % | n | % | n | % | Mean | SD | n | % | |
| Men | ||||||||||||||||||
| < 30 | 122.33 | 16.1 | 81.90 | 11.4 | 193.37 | 35.4 | 48.62 | 12.7 | 247 | 53.7 | 54 | 11.7 | 230 | 50.0 | 24.50 | 3.1 | 358 | 77.8 |
| 30–40 | 120.90 | 14.6 | 81.88 | 10.3 | 194.21 | 35.3 | 50.03 | 12.0 | 317 | 48.8 | 64 | 9.9 | 318 | 49.0 | 24.44 | 2.9 | 520 | 80.1 |
| 40 | 118.97 | 14.3 | 81.20 | 10.8 | 191.79 | 33.0 | 48.15 | 10.9 | 720 | 51.2 | 120 | 8.5 | 616 | 43.8 | 24.51 | 2.9 | 1164 | 82.8 |
| 40–50 | 119.04 | 14.5 | 80.72 | 10.6 | 193.68 | 36.5 | 49.04 | 11.4 | 783 | 50.0 | 115 | 7.3 | 738 | 47.1 | 24.34 | 3.1 | 1260 | 80.4 |
| 50–60 | 119.06 | 14.2 | 80.77 | 10.4 | 191.08 | 33.6 | 48.75 | 11.3 | 797 | 50.2 | 115 | 7.2 | 775 | 48.8 | 24.35 | 3.1 | 1301 | 82.0 |
| 60–70 | 118.95 | 14.9 | 80.65 | 10.8 | 192.61 | 34.4 | 49.28 | 11.2 | 507 | 50.2 | 77 | 7.6 | 508 | 50.3 | 24.24 | 3.1 | 813 | 80.6 |
| 70–80 | 119.80 | 15.0 | 80.90 | 11.0 | 192.00 | 35.4 | 48.79 | 12.7 | 252 | 45.4 | 49 | 8.8 | 283 | 51.0 | 24.69 | 3.0 | 446 | 80.4 |
| ≥ 0. | 120.77 | 14.9 | 81.50 | 10.6 | 197.04 | 36.3 | 48.17 | 10.2 | 157 | 47.3 | 44 | 13.3 | 171 | 51.5 | 24.37 | 3.1 | 269 | 81.0 |
| Total | 119.51 | 14.7 | 81.03 | 10.7 | 192.69 | 34.7 | 48.85 | 11.5 | 3780 | 50.0 | 638 | 8.4 | 3639 | 48.1 | 24.41 | 3.0 | 6131 | 81.0 |
| Women | ||||||||||||||||||
| < 30 | 112.91 | 15.8 | 74.12 | 10.0 | 190.26 | 35.3 | 55.69 | 12.4 | 717 | 52.8 | 62 | 4.6 | 71 | 5.2 | 23.39 | 3.4 | 544 | 40.1 |
| 30–40 | 113.71 | 16.0 | 74.48 | 10.2 | 190.95 | 35.4 | 55.79 | 12.4 | 492 | 50.5 | 41 | 4.2 | 55 | 5.6 | 23.29 | 3.5 | 433 | 44.5 |
| 40 | 111.85 | 15.0 | 74.00 | 9.7 | 184.69 | 33.9 | 56.17 | 12.2 | 487 | 49.6 | 44 | 4.5 | 45 | 4.6 | 23.05 | 3.2 | 436 | 44.4 |
| 40–50 | 113.69 | 16.4 | 74.83 | 10.8 | 187.96 | 35.4 | 56.25 | 12.5 | 557 | 51.3 | 43 | 4.0 | 58 | 5.3 | 23.27 | 3.3 | 501 | 46.2 |
| 50–60 | 115.42 | 16.7 | 75.18 | 10.1 | 190.20 | 34.0 | 55.34 | 12.4 | 393 | 51.9 | 39 | 5.2 | 53 | 7.0 | 23.62 | 3.3 | 360 | 47.6 |
| 60–70 | 115.38 | 16.3 | 74.89 | 10.4 | 191.65 | 35.2 | 55.69 | 13.2 | 245 | 50.2 | 26 | 5.3 | 35 | 7.2 | 23.74 | 3.3 | 216 | 44.3 |
| 70–80 | 118.29 | 17.9 | 76.83 | 11.1 | 193.66 | 36.9 | 54.60 | 11.6 | 156 | 42.5 | 23 | 6.3 | 28 | 7.6 | 24.02 | 3.4 | 172 | 46.9 |
| 6.8 | 117.88 | 17.0 | 76.57 | 10.1 | 199.32 | 39.7 | 55.43 | 12.6 | 98 | 43.6 | 16 | 7.1 | 14 | 6.2 | 24.50 | 3.2 | 106 | 47.1 |
| Total | 114.00 | 16.2 | 74.72 | 10.3 | 189.72 | 35.3 | 55.76 | 12.4 | 3145 | 50.4 | 294 | 4.7 | 359 | 5.8 | 23.43 | 3.4 | 2768 | 44.4 |
| Weekly working hours | Estimated 10-year CHD risk | ≥90th percentile of estimated risk of CHD | Estimated 10-year stroke risk | ≥90th percentile of estimated risk of stroke | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | mean | SD | n | % | aORa | 95% CI | mean | SD | n | % | aORa | 95% CI | |||
| Men | ||||||||||||||||
| < 30 | 460 | 6.1 | 1.59 | 14.7 | 89 | 19.4 | 1.75 | 1.28 | 2.40 | 1.59 | 14.7 | 97 | 21.1 | 1.77 | 1.29 | 2.42 |
| 30–40 | 649 | 8.6 | 1.25 | 19.3 | 72 | 11.1 | 1.04 | 0.76 | 1.42 | 1.25 | 19.3 | 86 | 13.3 | 1.24 | 0.91 | 1.68 |
| 40 | 1406 | 18.6 | 1.05 | 5.4 | 122 | 8.7 | 1.00 | Reference | 1.05 | 5.4 | 115 | 8.18 | 8.2 | Reference | ||
| 40–50 | 1567 | 20.7 | 1.03 | 13.2 | 137 | 8.7 | 0.89 | 0.69 | 1.16 | 1.03 | 13.2 | 130 | 8.3 | 0.85 | 0.65 | 1.11 |
| 50–60 | 1587 | 21.0 | 1.01 | 36.0 | 137 | 8.6 | 0.87 | 0.67 | 1.12 | 1.01 | 36 | 127 | 8.0 | 0.79 | 0.60 | 1.03 |
| 60–70 | 1009 | 13.3 | 1.06 | 46.0 | 88 | 8.7 | 0.83 | 0.62 | 1.11 | 1.06 | 46 | 93 | 9.2 | 0.87 | 0.65 | 1.17 |
| 70–80 | 555 | 7.3 | 1.13 | 14.4 | 52 | 9.4 | 0.83 | 0.59 | 1.19 | 1.13 | 14.4 | 63 | 11.4 | 0.99 | 0.70 | 1.39 |
| .39 | 332 | 4.4 | 1.37 | 4.9 | 59 | 17.8 | 1.76 | 1.23 | 2.52 | 1.37 | 4.86 | 45 | 13.6 | 1.23 | 0.83 | 1.82 |
| Total | 7565 | 100.0 | 1.11 | 21.8 | 756 | 10.0 | 1.97 | 15 | 756 | 10.0 | ||||||
| p trend | 0.43 | 0.94 | ||||||||||||||
| Women | ||||||||||||||||
| < 30 | 1357 | 21.8 | 0.26 | 18.2 | 136 | 10.0 | 1.11 | 0.81 | 1.54 | 1.45 | 10.2 | 141 | 10.4 | 1.41 | 1.00 | 1.99 |
| 30–40 | 974 | 15.6 | 0.26 | 122.0 | 95 | 9.8 | 1.08 | 0.77 | 1.53 | 1.42 | 6.2 | 96 | 9.9 | 1.34 | 0.94 | 1.93 |
| 40 | 981 | 15.7 | 0.19 | 16.8 | 65 | 6.6 | 1.00 | Reference | 1.14 | 26.5 | 53 | 5.40 | 5.4 | Reference | ||
| 40–50 | 1085 | 17.4 | 0.23 | 106.0 | 88 | 8.1 | 1.01 | 0.71 | 1.43 | 1.33 | 28.8 | 84 | 7.7 | 1.18 | 0.82 | 1.71 |
| 50–60 | 757 | 12.1 | 0.28 | 24.6 | 81 | 10.7 | 1.06 | 0.74 | 1.51 | 1.59 | 10 | 91 | 12.0 | 1.49 | 1.03 | 2.16 |
| 60–70 | 488 | 7.8 | 0.29 | 14.5 | 61 | 12.5 | 1.09 | 0.74 | 1.61 | 1.65 | 10.1 | 60 | 12.3 | 1.31 | 0.87 | 1.98 |
| 70–80 | 367 | 5.9 | 0.33 | 8.5 | 58 | 15.8 | 1.32 | 0.88 | 1.97 | 1.81 | 2.4 | 54 | 14.7 | 1.47 | 0.96 | 2.25 |
| .25 | 225 | 3.6 | 0.4 | 37.3 | 39 | 17.3 | 1.63 | 1.03 | 2.58 | 2.06 | 7.5 | 44 | 19.6 | 2.32 | 1.46 | 3.69 |
| Total | 6234 | 100.0 | 0.26 | 0.3 | 623 | 10.0 | 1.45 | 1.4 | 623 | 10.0 | ||||||
| p trend | 0.06 | 0.01 | ||||||||||||||
Table 1 Characteristics of the study population
*Any schedule other than fixed-day schedule includes day-night shift, fixed night, regular rotation, 24-h shift, split shift, irregular shift, and another schedule
Table 2 Cardiovascular and stroke risk profiles
Table 3 Odds ratios for high 10-year risk of CHD and stroke
aadjusted for household income, employment condition, occupation, work shift, and weekly working hour; values displaying significant differences are given in bold (
*

