
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 38; 2026 > Article
- Original Article Occupational Diseases in Mongolia: A Retrospective Analysis (1975–2023) with a 30-Year Trend Study
-
Sansartsetseg Tsendjav1
 , Myagmarchuluun Sainnyambuu1, Otgonbayar Damdinbazar2, Ulzii-Orshikh Ragchaabazar3, Gantugs Yundendorj4,*
, Myagmarchuluun Sainnyambuu1, Otgonbayar Damdinbazar2, Ulzii-Orshikh Ragchaabazar3, Gantugs Yundendorj4,* -
Annals of Occupational and Environmental Medicine 2026;38:e12.
DOI: https://doi.org/10.35371/aoem.2026.38.e12
Published online: March 24, 2026
1Department of Environmental Health, School of Public Health, Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia
2Division for Science, Technology and Innovation, Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia
3Occupational Health and Safety Center, Occupational Medical Hospital, Ulaanbaatar, Mongolia
4Department of Health Policy, School of Public Health, Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia
- *Corresponding author: Gantugs Yundendorj Department of Health Policy, School of Public Health, Mongolian National University of Medical Sciences, S.Zorig Street, 48/111, Ulaanbaatar, 14210, Mongolia E-mail: gantugs@mnums.edu.mn
• Received: January 25, 2026 • Revised: March 19, 2026 • Accepted: March 20, 2026
© 2026 Korean Society of Occupational & Environmental Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,809 Views
- 42 Download
Abstract
-
Background Occupational diseases represent a significant global public health challenge, yet reliable data from transitioning economies remain limited. This study aimed to analyze newly confirmed occupational disease cases in Mongolia over a 50-year period (1975–2023), identifying long-term trends and the prevalence of leading disease categories.
-
Methods A retrospective, record-based study was conducted using quantitative data from 10,233 officially confirmed and compensated cases of occupational diseases resulting in an officially certified loss of labor capacity. Incidence rates per 100,000 workers were calculated for the 1992–2023 period. Leading diseases were classified by organ system, with focused analyses on respiratory diseases, occupational poisonings, and neurological disorders.
-
Results Dust- and particulate-induced respiratory diseases accounted for the largest proportion of cases (57.4%), followed by occupational neurological disorders (16.2%) and occupational poisonings (8.0%). From 1992 to 2023, incidence rates among male workers were consistently 3–7 times higher than those among female workers. Analysis of exposure duration showed mean durations of 13.6 ± 4.9 years for silicosis (J62) and 20.7 ± 10.7 years for inorganic substance poisoning (T57). While respiratory diseases were predominant historically, occupational neurological diseases demonstrated an increasing trend after 2015.
-
Conclusions Occupational neurological disorders are showing an increasing trend in Mongolia, reflecting a shift in the national occupational disease pattern. However, as the registry is based on the national compensation framework, these findings likely reflect recognized cases rather than the true epidemiological incidence, suggesting potential underreporting. Strengthening surveillance beyond the compensation system and improving diagnostic capacity for a broader range of work-related conditions are essential for effective prevention and policy development.
BACKGROUND
The International Labour Organization (ILO) defines occupational diseases as conditions resulting from exposure to hazardous factors in the workplace.1 Globally, occupational exposures remain a major public health concern. It is estimated that approximately 1.9 million individuals die each year due to work-related causes, with nearly 7,500 deaths occurring daily. Among these, about 6,500 deaths are attributable to occupational diseases and 1,000 to industrial accidents.2,3 According to the World Health Organization, workplace risk factors contribute to 37% of back pain cases, 16% of hearing loss, 13% of chronic obstructive pulmonary disease, 9% of lung cancer, and 2% of hematologic malignancies worldwide.4
In 2010, the ILO classified occupational diseases into four major groups based on exposure to risk factors and listed a total of 194 conditions.5 These classifications provide an important international framework for the identification, surveillance, and prevention of occupational diseases.
In Mongolia, a legal and institutional framework for recognizing disability due to occupational diseases has existed since the 1940s, largely modeled on the experience of the former Soviet Union. Medical-labor assessment commissions were established to determine work capacity loss related to occupational diseases.6 Regulatory, therapeutic, nursing, and rehabilitation services for occupational diseases were formally introduced in 1972. Between 1972 and 2023, a total of 12,103 occupational disease cases were officially registered nationwide.7
Mongolia experienced a major socioeconomic transition in 1990, shifting from a centrally planned economy to a market-oriented system. This transition led to substantial structural changes in the industrial sector, including privatization, restructuring, and the closure of many state-owned enterprises. Prior to 1990, the national economy was predominantly state-controlled under centralized planning. However, during the 1990s the economy faced a prolonged period of stagnation while the private sector gradually expanded.
Beginning in the early 2000s, particularly after 2002, Mongolia entered a period of economic recovery characterized by sustained growth in gross domestic product and improvements in living standards. During this period, small and medium-sized enterprises expanded rapidly, and the mining and construction sectors experienced significant growth. Consequently, the size of the workforce increased substantially. Alongside these developments, increasing attention was directed toward occupational health and safety, particularly regarding workers’ exposure to occupational risk factors in rapidly developing industries.
Within the national health system, a total of 4,914 healthcare institutions were operating in Mongolia as of 2025. Healthcare facilities are classified according to the type of medical services provided and include Family Health Centers, Soum and Village Health Centers, Palliative and Nursing Care Centers, Clinics, Maternity Hospitals, Public Health Centers, General Hospitals, Sanatoriums, Emergency Care Centers, Specialized Hospitals, Specialized Centers, and Nursing Centers.8
Under the Ministry of Family, Labor and Social Protection, the Occupational Safety and Health Center operates a specialized hospital responsible for the diagnosis, registration, monitoring, and treatment of occupational diseases. Within this institution, occupational disease cases are evaluated by a multidisciplinary committee consisting of ten members, including six specialized physicians led by a representative physician from the Social Insurance Authority, along with representatives of employers, persons with disabilities, and labor unions. This committee is responsible for confirming occupational disease diagnoses and determining the degree and duration of work capacity impairment.9
Located in Ulaanbaatar, this institution functions as the national referral center for occupational diseases, providing diagnostic services, case registration and surveillance, outpatient medical care, and rehabilitation services across the country.
In 1995, Mongolia enacted a comprehensive Social Insurance Law package that established the national social insurance framework. The system comprises five major schemes: pension insurance, social benefit insurance, unemployment insurance, insurance for industrial accidents and occupational diseases, and health insurance. Enrollment in this system is mandatory for all employed individuals.10
Under a government resolution, enterprises are categorized by occupational risk level, with differentiated employer contribution rates of 0.5%, 1.5%, and 2.5% applied to insurance for industrial accidents and occupational diseases. This risk-based contribution system serves as an important financial mechanism for compensation and management of occupational diseases.11
The national list of occupational diseases has undergone several revisions since its initial adoption in 1972. As of 2023, the list includes 42 occupational diseases classified into nine organ-system-based categories for diagnostic purposes.12 Diagnostic standards and guidelines are applied for respiratory diseases caused by dust and toxic exposures, including chronic bronchitis, asthma, pneumoconiosis, anthracosis, silicosis, silicotuberculosis, and anthracosilicosis.13
According to recent national data, the Occupational Disease Department of the Center for Occupational Safety and Health currently monitors 2,593 patients who have lost work capacity due to occupational diseases. Among these patients, 51.4% are affected by dust and particle-induced respiratory diseases, 26.1% by neurological disorders, 9.5% by toxic exposures, and the remaining cases involve ear, nose, and throat disorders, skin allergies, radiation-related conditions, and eye diseases.14
In 2008, Mongolia adopted its first stand-alone Occupational Safety and Health Law, together with supporting regulations and standards, establishing a comprehensive legal and administrative framework for occupational health management.15 Workers who lose 30% or more of their work capacity due to occupational diseases are eligible to receive disability pensions.16 Additional support mechanisms include medical rehabilitation services, prosthetics, orthotics, and other rehabilitative care.17 However, mechanisms for job reassignment and long-term social reintegration remain limited.
This study aimed to analyze trends in occupational diseases in Mongolia over the past 30 years and to provide a detailed assessment of newly reported cases, the prevalence of major conditions, and potential future trends in occupational health.
METHODS
Nationwide, the Center for Occupational Safety and Health of Mongolia maintains an occupational disease registry in which occupational diseases are diagnosed, the degree and duration of work capacity loss are assessed, and cases are systematically recorded.18 Using these records, we collected quantitative data on 10,233 new cases of occupational diseases with confirmed work capacity losses between 1975 and 2023. The dataset included personal information (identification number, age, sex, education, and affiliation), occupational information (profession, workplace, years of service, and years of exposure to hazardous conditions), and details of primary and comorbid diagnoses.
Since 1992, Mongolia has maintained records of the total workforce,19 enabling calculation of the incidence of occupational diseases per 100,000 workers over the 30-year period from 1992 to 2023. Leading occupational diseases were classified by organ system, and analyses focused on occupational respiratory diseases, occupational toxicities, occupational neurological disorders, occupational ear, nose, and throat (ENT) disorders, and occupational musculoskeletal disorders.
Prolonged exposure to industrial dust and particulate matter can cause primary chronic inflammation of the bronchi and lungs, leading to irreversible structural changes.20 Diagnosed occupational respiratory diseases included dust-induced anthracosis (J60), asbestosis (J61), silicosis (J62), siderosis and cementosis (J63), pneumoconiosis (J64), silicotuberculosis (J65), byssinosis (J66), chronic bronchitis (J68), and asthma (J68.4).
Acute exposure to highly toxic chemicals in the workplace can cause rapid onset of poisoning, whereas chronic exposure leads to bioaccumulation and cellular damage.21 Occupational toxicities included poisoning from organic compounds (T52), aromatic compounds (T53), heavy metals (T56), inorganic compounds (T57), acute carbon monoxide (CO) (T58), irritant or asphyxiant chemicals (T59), and pesticides (T60).
Work involving prolonged or repetitive forceful movements, awkward postures, unfavorable environmental conditions, or vibration exposure may result in spinal and lumbosacral disorders (G54).22 Other occupational neurological conditions included vibration-related neuropathies (T75) and radiation-induced neurological disorders (W85).
Noise exposure in the workplace caused hearing loss (H83.3), and vocal organ disorders (J38) and upper respiratory tract disorders due to dust, particulates, or chemicals (J31) were also documented.
Repetitive work and awkward postures contributed to occupational lower limb, abdominal, and pelvic venous dilation (I83), occupational elbow joint motion disorders (M21.2), occupational upper limb injuries and repetitive strain disorders (M67.8), and occupational flatfoot (M21.4).
Other occupational conditions included chemical-induced contact dermatitis (L23), corneal inflammation (H17), secondary glaucoma (H40), retinal disorders (H35), radiation-induced hematologic diseases (W88–W91), and occupational cancers.
Data were analyzed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). Continuous variables were summarized using means and standard deviations, and categorical variables were described using frequencies and percentages. Differences in means among three or more independent groups were assessed using one-way analysis of variance (one-way ANOVA). Pearson’s correlation coefficient was used to evaluate the associations between two continuous variables. Statistical significance was set at p < 0.05. Linear regression analysis was performed to assess the relationships between two continuous variables, and the coefficient of determination (R2) was calculated.
The research methodology was discussed and approved by the Academic Council of the School of Public Health at the Mongolian National University of Medical Sciences on 29 May 2024 (meeting No. 24/13). The requirement for informed consent was waived due to the retrospective design of the study and the use of anonymized, de-identified registry data.
Ethical approval to conduct the research and the research methodology was further reviewed and approved during the meeting of the Research Ethics Review Committee of the Mongolian National University of Medical Sciences on 14 June 2024, and research permission (2024/3-06) was issued.
RESULTS
A total of 10,233 occupational diseases were recorded between 1975 and 2023. Newly confirmed cases from selected years at 10-year intervals were analyzed, and the distribution of predominant diseases by organ system showed that dust- and particulate-induced respiratory diseases accounted for 57.4% of cases; occupational neurological disorders, 16.2%; occupational toxicities, 8.0%; occupational musculoskeletal disorders, 7.5%; and occupational ENT disorders, 4.2%.
The number of newly diagnosed cases was 382 in 1975, 176 in 1985, 203 in 1995, and 379 in 2005 but declined sharply to 27 in 2015, representing a 14-fold reduction. The incidence of newly diagnosed occupational diseases per 100,000 workers was 26.4 in 1995, increased to 39.1 in 2005, and subsequently declined to 2.3 in 2015.
The incidence of newly diagnosed dust- and particulate-induced respiratory diseases was 1.0 per 100,000 workers in 2015 and increased to 1.4 in 2023. Similarly, the incidence of occupational neurological disorders rose from 0.7 in 2015 to 2.9 in 2023. In contrast, the incidence of occupational toxicities decreased from 0.3 in 2015 to 0.1 in 2023 (Table 1).
Between 1992 and 2023, the number of newly diagnosed occupational disease cases declined from 564 in 1992 to 301 in 2002 and 45 in 2012, representing a 12-fold decrease from 1992 and a 7-fold decrease from 2002. When calculated per 100,000 workers, the incidence of new cases was 70 in 1992, 32.4 in 2002 (a 2.1-fold decrease), 45.9 in 2003, and 3.3 in 2013 (a 14-fold decrease compared with the previous decade). By 2023, the incidence of newly diagnosed cases had increased slightly to 4.6 per 100,000 workers, an absolute increase of 1.3 compared with 2013. Prior to 1992, workforce statistics in Mongolia were maintained exclusively in paper archives. Electronic labor force records became available beginning in 1992, allowing incidence rates of occupational diseases to be calculated per 100,000 working population from that year onward. Before 1990, Mongolia operated under a centrally planned economy, with over 80% of the working-age population formally employed. The subsequent transition to a market economy led to the closure of numerous inefficient enterprises, resulting in higher unemployment and, concurrently, increased reporting and diagnosis of occupational diseases (Fig. 1).
Analysis of the 5-year trends in the incidence of newly diagnosed occupational diseases per 100,000 workers between 1992 and 2023 revealed that the incidence ranged from 28.2 to 32.4 during 1993–1997, 34.6 to 50.2 during 1998–2002, 27.9 to 45.9 during 2003–2007, 4.3 to 26.8 during 2008–2012, 3.3 to 5.5 during 2013–2017, and 3.0 to 4.6 during 2018–2023, indicating a declining trend since 2009. During the same period, the incidence among male workers was three to seven times higher than that among female workers. From 2002 onward, sustained economic growth with an average annual GDP increase of approximately 7.5% improved overall living standards.23
By 2007, household income had risen by roughly 30%, elevating Mongolia from a low-income to a lower-middle-income country. In addition, the enactment of the first Law on Occupational Safety and Health in 2008 improved workplace conditions across enterprises. The combined effect of these socioeconomic and legislative changes contributed to a declining trend in newly diagnosed occupational disease cases from 2009 onward (Fig. 2).
In Mongolia, predominant occupational diseases are categorized into three organ system groups: dust- and particulate-induced respiratory diseases, occupational neurological disorders, and occupational toxicities. When examining new cases according to years of exposure to hazardous conditions, the mean duration of exposure for dust- and particulate-induced respiratory diseases was 13.6 ± 4.9 years for silicosis (J62) and 17.4 ± 5.4 years for siderosis and cementosis (J63). Among occupational toxicities, acute carbon monoxide poisoning (T58) had the shortest exposure duration of 9.3 ± 5.7 years, while inorganic compound poisoning (T57) had the longest exposure duration of 20.7 ± 10.7 years. Among the occupational neurological disorders, lumbar and lumbosacral spine disorders (G54) were the most frequently diagnosed, with a mean exposure duration of 17.7 ± 5.6 years.
The most frequently diagnosed conditions between 1992 and 2023 were chronic bronchitis of the bronchi (J68, 4,027 cases), anthracosis (J60, 1,049 cases), silicosis (J62, 659 cases), and lumbar/lumbosacral spine disorders (G54, 1,622 cases) (Table 2). The relatively low number of reported occupational toxicity cases may reflect underreporting, rather than a truly low incidence.
Analysis of dust- and particulate-induced respiratory diseases at 10-year intervals between 1975 and 2023 revealed that the proportion of anthracosis (J60) cases due to coal dust was 52.1% in 1975, 16.3% in 1985, 3.2% in 1995, 2.2% in 2005, and 5.9% in 2023. In contrast, silicosis (J62) caused by crystalline silica dust accounted for 31.6% in 1975, 1.1% in 1995, 50% in 2015, and 35.3% in 2023. The incidence of chronic bronchitis of the bronchi (J68) fluctuated over the same period (Table 3).
Between 1975 and 2015, respiratory diseases represented the largest proportion of occupational diseases, with chronic bronchitis of the bronchi (J68), silicosis (J62), and anthracosis (J60) being the most frequent. Since 2015, the incidence of occupational neurological disorders has demonstrated a significant increasing trend (Fig. 3). This increasing trend in occupational neurological disorders reflects a shift in the pattern of occupational disease occurrence over time.
DISCUSSION
This study analyzed registry data on confirmed occupational disease cases in Mongolia from 1975 to 2023, offering a unique longitudinal perspective across two distinct socioeconomic systems. The ILO convention states that “workers should be protected against diseases, infectious conditions, and accidents arising in connection with their employment.”24 Between 1975 and 2015, dust- and particulate-induced respiratory diseases were the predominant occupational diseases. However, since 2015, occupational neurological disorders have shown an increasing trend, consistent with previous findings on the Mongolian occupational landscape.25 The incidence was notably higher among male workers, with statistically significant associations observed among those exposed to hazardous conditions for 15–20 years.
During the 1990s, Mongolia’s transition to a market economy and the resulting closure of state-owned enterprises influenced reporting patterns.26 This period of workforce restructuring, similar to transitions observed in Eastern Europe, coincided with significant fluctuations in the incidence of occupational diseases.27 Following the enactment of the first stand-alone Law on Occupational Safety and Health in 2008, a declining trend in newly diagnosed cases has been observed (see Supplementary Table 1 and Supplementary Fig. 1 for detailed legal framework comparisons and the diagnostic process flow). However, as noted internationally, underreporting and limited diagnostic capabilities remain common challenges in reflecting the true disease burden.28
In the context of Mongolia, several institutional and systemic barriers likely contribute to this underreporting. Our findings primarily reflect cases captured within the national compensation framework, which may not represent the true epidemiological burden. The surveillance system is intrinsically linked to the social insurance scheme; consequently, workers in the informal sector often lack formal coverage and are effectively excluded from official registries. Furthermore, limited diagnostic capacity and the restrictive nature of the national occupational disease list, which currently excludes common conditions like herniated nucleus pulposus, further hamper the full identification of cases. These factors suggest that the actual incidence of occupational diseases in Mongolia is likely higher than the officially recorded figures. Expanding the scope of recognized occupational conditions and establishing standardized clinical guidelines, diagnostic criteria, and reporting systems for work-related diseases are essential to strengthen occupational health surveillance and support the development of evidence-based prevention policies.
Our study found a marked increase in occupational neurological disorders since 2015, a trend that mirrors patterns observed in European registries, where respiratory and vibration-related disorders have declined while neurological conditions have increased.4 Globally, chronic obstructive pulmonary disease (COPD) due to dust and chemical exposure accounts for a major portion of occupational mortality;29 however, the absence of COPD in our dataset highlights a critical gap in current diagnostic frameworks.
Regarding the broader health impact, the average loss of 8.05 years of life relative to the general life expectancy emphasizes the severity of occupational morbidity in Mongolia.30 Although the national list of occupational diseases has undergone six revisions since 1972 to improve diagnostic criteria, there is still no standardized national framework for diagnosing broader work-related diseases.31,32 Establishing such a framework and expanding the scope of recognized conditions are essential steps toward strengthening surveillance and developing evidence-based prevention policies.
These findings highlight the importance of strengthening the institutional and professional capacity of the occupational health system in Mongolia. Improving workforce training, expanding diagnostic expertise, and ensuring equitable access to quality healthcare services are essential for enhancing case detection and surveillance. The observed trends likely reflect not only changes in disease occurrence but also variations in healthcare infrastructure, diagnostic capacity, and professional competency. In addition, broader legal, administrative, and economic contexts may substantially influence occupational disease reporting patterns and long-term trends.
CONCLUSIONS
This 50-year longitudinal analysis provides a comprehensive and unprecedented mapping of occupational disease patterns across Mongolia’s shifting industrial landscape. The observed trends reflect a complex interplay between actual disease occurrence and the evolution of healthcare infrastructure and diagnostic capacity. By documenting transitions across two distinct socioeconomic systems, this study offers critical evidence for the international research community on the long-term impact of industrial transformation in a transitioning economy.
Abbreviations
COPD
chronic obstructive pulmonary disease
ENT
ear, nose, and throat
ILO
International Labour Organization
-
Competing interests
The authors declare that they have no competing interests.
-
Author contributions
Conceptualization: Yundendorj G, Tsendjav S. Data curation: Tsendjav S, Yundendorj G. Methodology/formal analysis/validation: Tsendjav S, Yundendorj G, Sainnyambuu M. Project administration: Tsendjav S. Funding acquisition: Tsendjav S. Writing - original draft: Yundendorj G, Tsendjav S. Writing - review & editing: Tsendjav S, Sainnyambuu M, Damdinbazar O, Ragchaabazar UO, Yundendorj G.
NOTES
SUPPLEMENTARY MATERIAL
Supplementary Table 1.
First stand-alone Occupational Safety and Health Law 2008.
Supplementary Fig. 1.
The process for assessing occupational diseases.
Fig. 1.
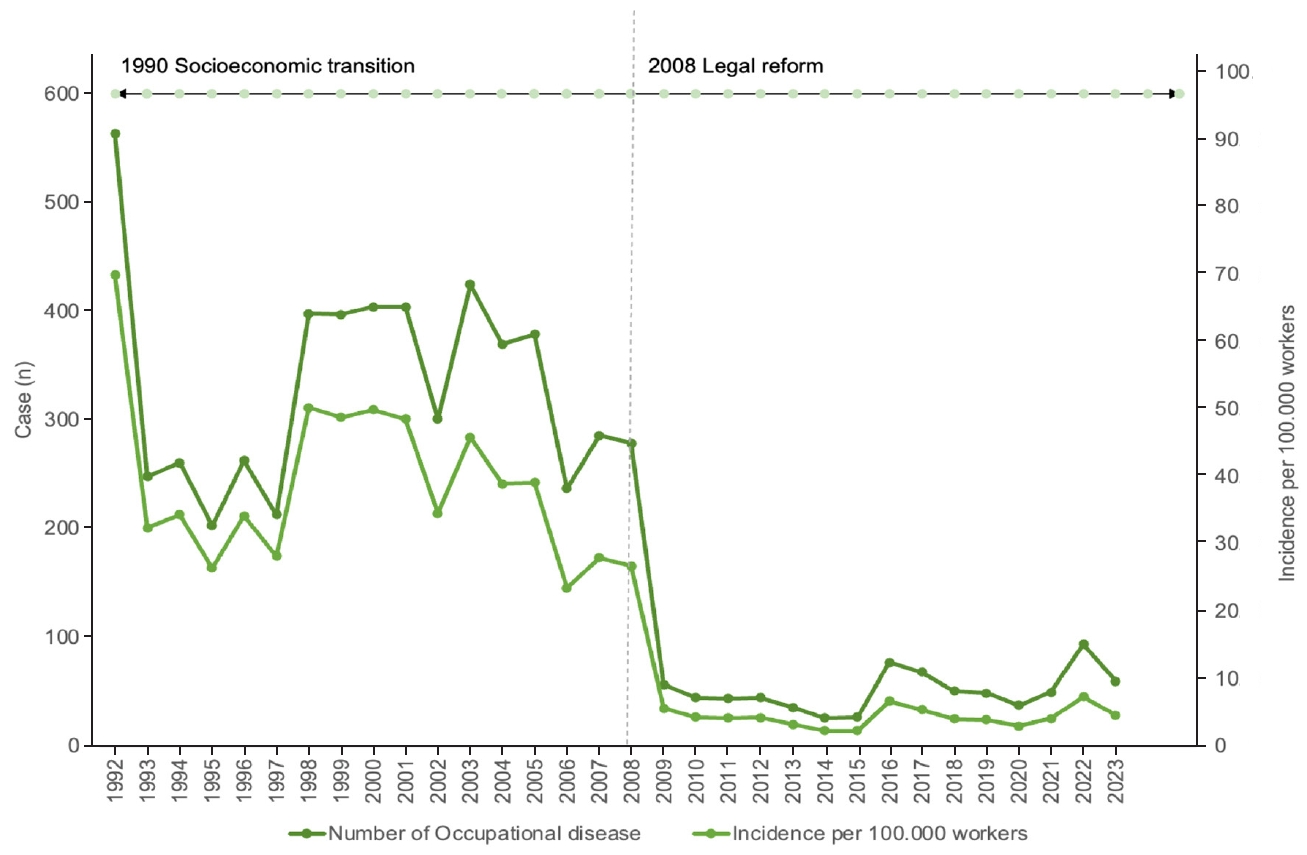
Number and incidence per 100,000 workers of newly diagnosed occupational disease cases, 1992–2023.
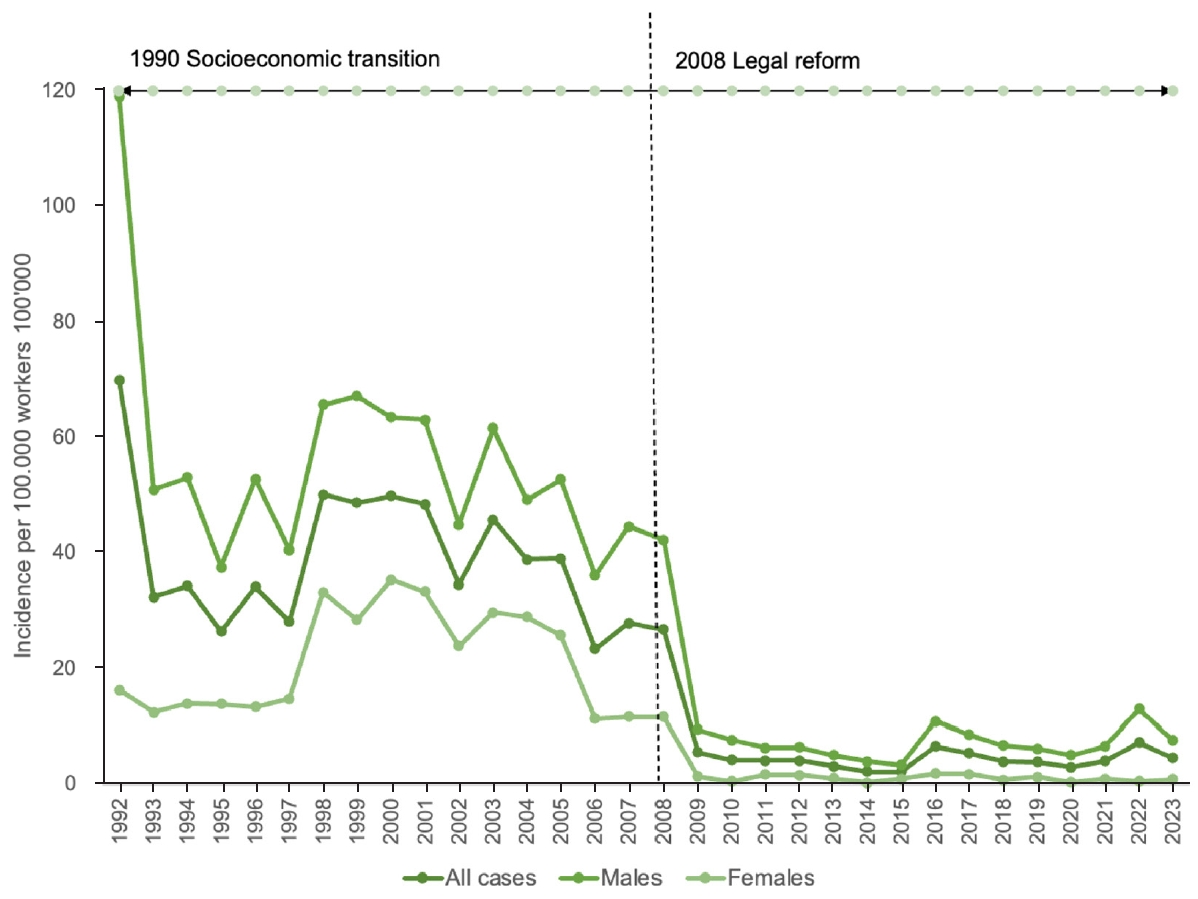
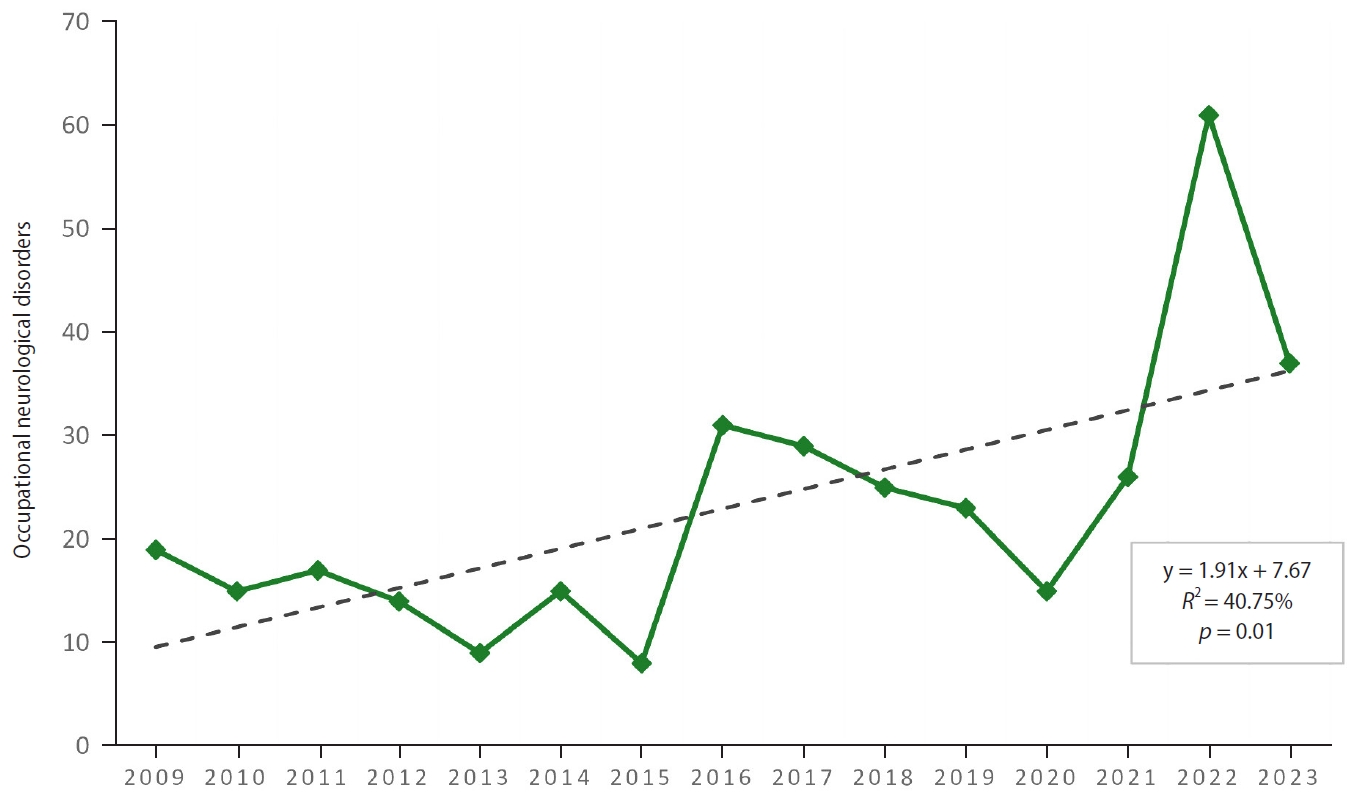
Table 1.
Distribution of predominant occupational diseases by organ system, 1975–2023
| New cases, n (%) | Incidence per 100,000 workersa | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1975-2023b | 1975 | 1985 | 1995 | 2005 | 2015 | 2023 | 1975-2023 | 1995 | 2005 | 2015 | 2023 | |
| Dust- and particulate-induced respiratory diseases | 5,873 (57.4) | 263 | 141 | 94 | 135 | 12 | 17 | 453.6 | 12.2 | 13.9 | 1 | 1.4 |
| Occupational neurological disorders | 1,659 (16.2) | 16 | 3 | 27 | 113 | 8 | 37 | 128.1 | 3.5 | 11.7 | 0.7 | 2.9 |
| Occupational toxicity | 815 (8.0) | 22 | 13 | 19 | 27 | 3 | 1 | 62.9 | 2.5 | 2.8 | 0.3 | 0.1 |
| Occupational musculoskeletal disorders | 767 (7.5) | 28 | 1 | 36 | 37 | 0 | 0 | 59.2 | 4.7 | 3.8 | 0 | 0 |
| Occupational ear, nose, and throat (ENT) disorders | 433 (4.2) | 6 | 1 | 14 | 22 | 2 | 3 | 33.4 | 1.8 | 2.3 | 0.2 | 0.2 |
| Other occupational diseases | 686 (6.7) | 47 | 17 | 13 | 45 | 2 | 1 | 53 | 1.7 | 4.6 | 0.2 | 0.1 |
| Totalb | 10,233 (100) | 382 (3.7) | 176 (1.7) | 203 (2) | 379 (3.7) | 27 (0.2) | 59 (0.6) | 790.3 | 26.4 | 39.1 | 2.3 | 4.6 |
Table 2.
Comparison of confirmed occupational disease cases by years of exposure to hazardous conditions, 1992–2023
Table 3.
Dust- and particulate-induced respiratory disease cases, 1975–2023
- 1. International Labour Organization. Diagnostic and Exposure Criteria for Occupational Diseases: Guidance Notes for Diagnosis and Prevention of the Diseases in the ILO List of Occupational Diseases (Revised 2010). Geneva, Switzerland: International Labour Organization; 2010.
- 2. World Health Organization; International Labour Organization. WHO/ILO Joint Estimates of the Work-Related Burden of Disease and Injury, 2000-2016: Global Monitoring Report. Geneva, Switzerland: World Health Organization; 2017.
- 3. International Labour Organization. Safety and Health at the Heart of the Future of Work. Geneva, Switzerland: International Labour Organization; 2019.
- 4. Kudasz F, Nagy K, Nagy I. Occupational diseases in Belgium, the Czech Republic and Hungary: a comparison. Cent Eur J Occup Environ Med 2017;23(1-2):32–49.
- 5. International Labour Organization. List of Occupational Diseases. International Labor Conference Recommendation 194. Geneva, Switzerland: International Labour Organization; 2010.
- 6. Ministry of Labour and Social Protection of Mongolia. Occupational Health Status Report. Ulaanbaatar, Mongolia: Ministry of Labour and Social Protection of Mongolia; 2018.
- 7. Center for Occupational Safety and Health. Occupational Disease Registry Statistics, 1967-2023. Ulaanbaatar, Mongolia: Center for Occupational Safety and Health; 2023.
- 8. Law of Mongolia. On Health. Article 13.1, 15.1. Ulaanbaatar, Mongolia: Law of Mongolia; 2011.
- 9. General Authority for Social Insurance. Regulation on the Operation of the Labor Medical Assessment Sub-Council. Ulaanbaatar, Mongolia: General Authority for Social Insurance; 2022.
- 10. Law of Mongolia. General Law of Social Insurance. Article 6. Ulaanbaatar, Mongolia: Law of Mongolia; 2023.
- 11. Government of Mongolia. Resolution A/471. Ulaanbaatar, Mongolia: Government of Mongolia; 2023.
- 12. Ministry of Health, Labor and Social Protection. Joint Order A/152, A/388: List of Occupational Diseases, Approval of Proportions and Duration. Ulaanbaatar, Mongolia: Ministry of Health. Labor and Social Protection; 2023.
- 13. Standards and Metrology Agency. MNS 6336-1:2012 Diagnosis of Occupational Byssinosis; 6336-2:2012 Chronic Bronchial Diseases due to Dust; 6336-3:2012 Pulmonary Dust Diseases; 6336-4:2012 Silicosis Diagnosis and Treatment. Ulaanbaatar, Mongolia: Standards and Metrology Agency; 2012.
- 14. Center for Occupational Safety and Health. Annual Report of Occupational Disease Hospital. Ulaanbaatar, Mongolia: Center for Occupational Safety and Health; 2023.
- 15. Ministry of Labour and Social Protection of Mongolia. Occupational Safety and Health Law Implementation Survey. Ulaanbaatar, Mongolia: Ministry of Labour and Social Protection of Mongolia; 2016.
- 16. Government of Mongolia. Social Insurance Package Law. Ulaanbaatar, Mongolia: Government of Mongolia; 2023.
- 17. General Authority for Social Insurance. Procedures for Labor Assessment Commission. Ulaanbaatar, Mongolia: General Authority for Social Insurance; 2023.
- 18. Government of Mongolia. Resolution A/448. Rules of the Health Assessment Council. Ulaanbaatar, Mongolia: Government of Mongolia; 2023.
- 19. National Statistics Office of Mongolia. Statistical Records and Data. Ulaanbaatar, Mongolia: National Statistics Office of Mongolia; 2023.
- 20. Milde JJ. Guidelines for Occupational Medical Examination: Prophylaxis in Occupational Medicine. Stuttgart, Germany: Gentner Verlag; 2007.
- 21. Smedley J, Dick F. Oxford Handbook of Occupational Health. 2nd ed. Oxford, UK: Oxford University Press; 2013.
- 22. Center for Occupational Safety and Health. Occupational Diseases Caused by Chemical Substances. Ulaanbaatar, Mongolia: Center for Occupational Safety and Health; 2021.
- 23. Asian Development Bank. Economic Outlook of Mongolia: 1990-2020. Manila, Philippines: Asian Development Bank; 2020, 14–16.
- 24. International Labour Organization. Introduction to International Labour Standards. Geneva, Switzerland: International Labour Organization; 2019.
- 25. Oyunbileg S, Sumberzul N, Oyuntogos L, Javzmaa J, Wang JD. Analysis of incidence rates of occupational diseases from 1986-2006. Int J Occup Environ Health 2011;17:31–7.ArticlePubMed
- 26. Bank of Mongolia. Mongolian Economy: 30 Years of Lessons and Solutions. Research Compilation. Ulaanbaatar, Mongolia: Bank of Mongolia; 2020.
- 27. Szeszenia-Dabrowska N, Wilczynska U. Occupational diseases in Poland: an overview of current trends. Int J Occup Med Environ Health 2013;26(3):457–70.ArticlePubMed
- 28. Takala J, Hamalainen P, Nenonen N, Takahashi K, Chimed-Ochir O, Rantanen J. Comparative analysis of the burden of injury and illness at work in selected countries and regions. Cent Eur J Occup Environ Med 2017;23(1-2):6–31.
- 29. GBD 2016 Occupational Risk Factors Collaborators. Global and regional burden of disease and injury in 2016 arising from occupational exposures: a systematic analysis for the Global Burden of Disease Study 2016. Occup Environ Med 2020;77(3):133–41.ArticlePubMedPMC
- 30. Otgonnasan A, Damdinbazar O, Damiran N, Erdenebayar E, Yundendorj G. Diseases-attributable disability-adjusted life years in copper and molybdenum ore workers in Mongolia: 1999-2019. Int J Environ Health Res 2023;33:661–9.ArticlePubMed
- 31. Davoodi S, Haghighi KS, Kalhori SR, Hosseini NS, Mohammadzadeh Z, Safdari R. Occupational disease registries: characteristics and experiences. Acta Inform Med 2017;25(2):136–40.ArticlePMC
- 32. Kang SK, Kim EA. Occupational diseases in Korea. J Korean Med Sci 2010;25(Suppl):S4–12.ArticlePubMedPMC
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteOccupational Diseases in Mongolia: A Retrospective Analysis (1975–2023) with a 30-Year Trend Study
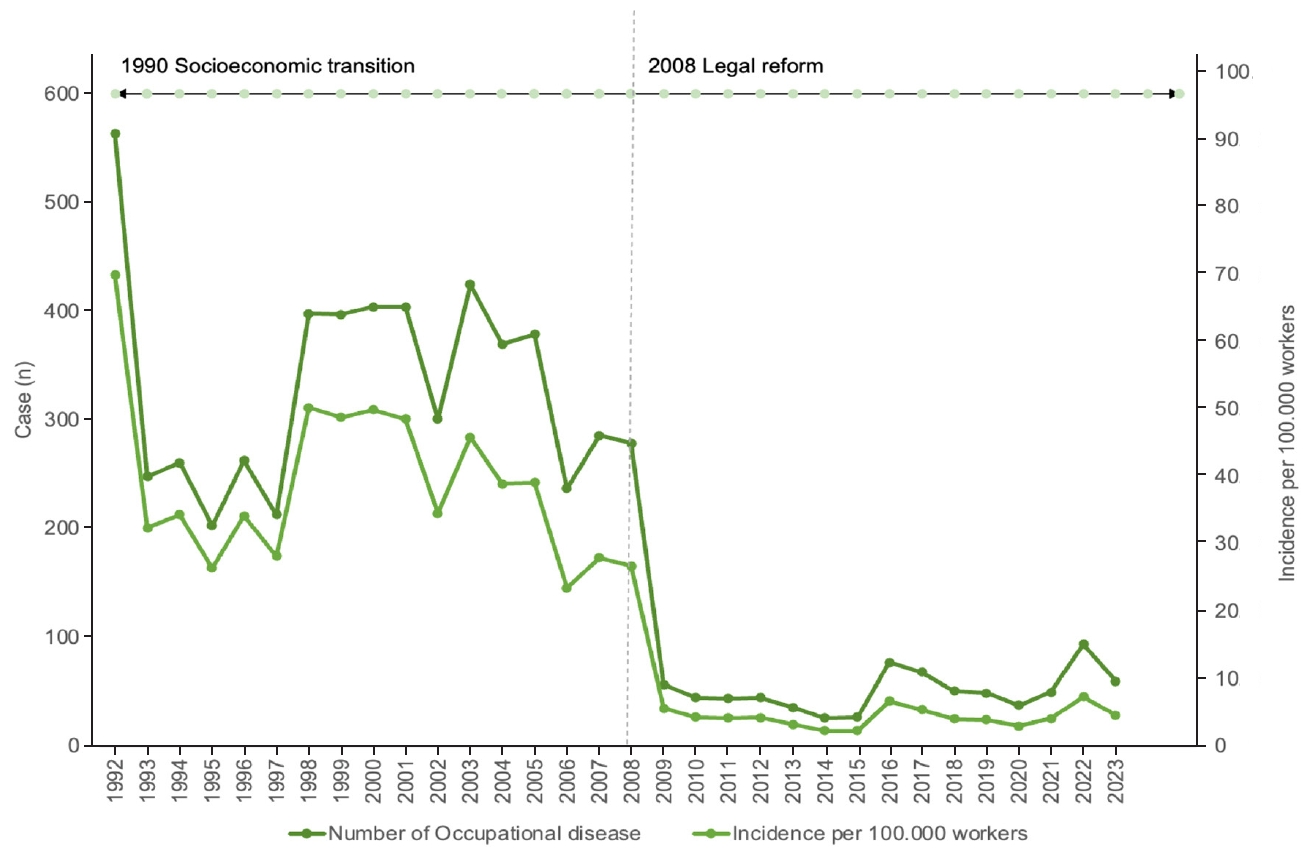
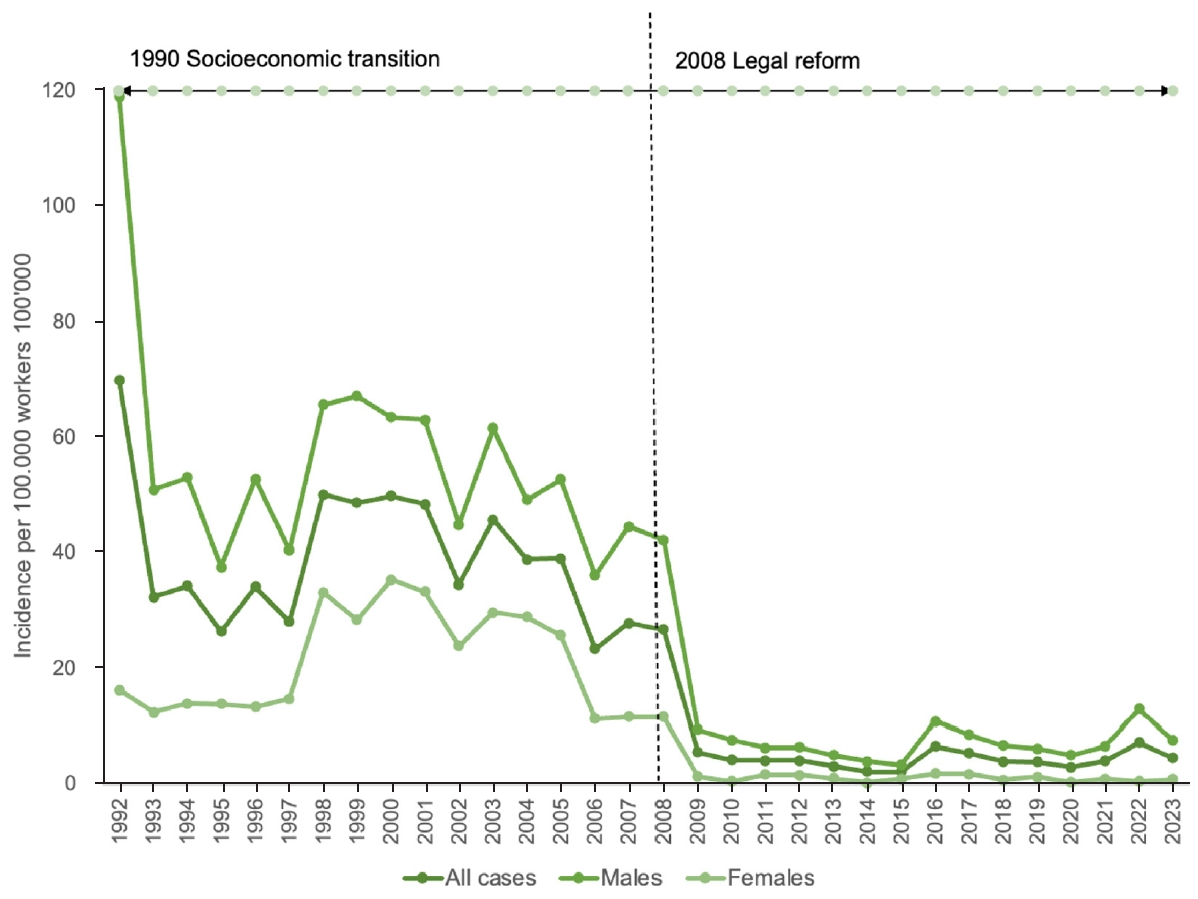
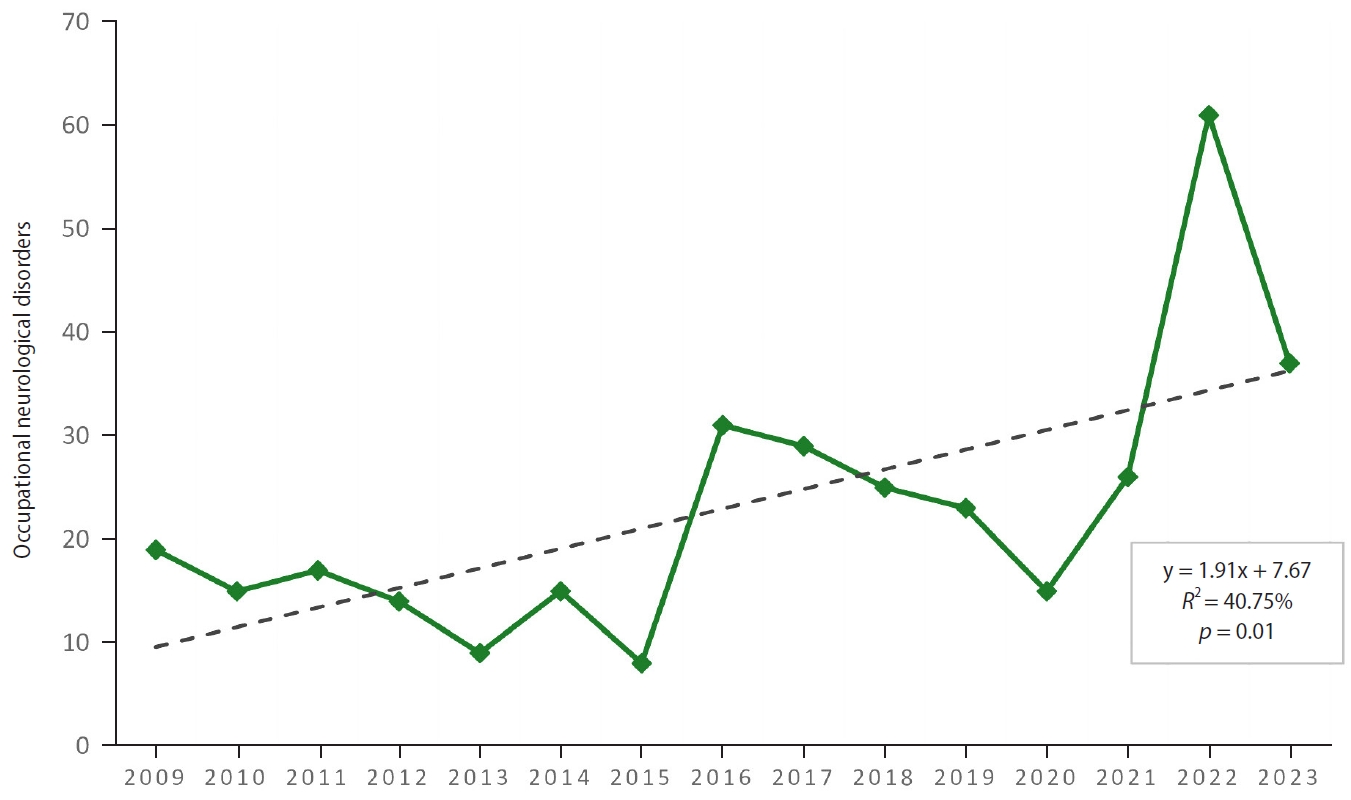
Fig. 1. Number and incidence per 100,000 workers of newly diagnosed occupational disease cases, 1992–2023.
Fig. 2. Incidence of newly diagnosed occupational disease cases by gender, 1992–2023.
Fig. 3. Occupational neurological disorder cases, 2009–2023.
Fig. 1.
Fig. 2.
Fig. 3.
Occupational Diseases in Mongolia: A Retrospective Analysis (1975–2023) with a 30-Year Trend Study
| New cases, n (%) | Incidence per 100,000 workers |
|||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1975-2023 |
1975 | 1985 | 1995 | 2005 | 2015 | 2023 | 1975-2023 | 1995 | 2005 | 2015 | 2023 | |
| Dust- and particulate-induced respiratory diseases | 5,873 (57.4) | 263 | 141 | 94 | 135 | 12 | 17 | 453.6 | 12.2 | 13.9 | 1 | 1.4 |
| Occupational neurological disorders | 1,659 (16.2) | 16 | 3 | 27 | 113 | 8 | 37 | 128.1 | 3.5 | 11.7 | 0.7 | 2.9 |
| Occupational toxicity | 815 (8.0) | 22 | 13 | 19 | 27 | 3 | 1 | 62.9 | 2.5 | 2.8 | 0.3 | 0.1 |
| Occupational musculoskeletal disorders | 767 (7.5) | 28 | 1 | 36 | 37 | 0 | 0 | 59.2 | 4.7 | 3.8 | 0 | 0 |
| Occupational ear, nose, and throat (ENT) disorders | 433 (4.2) | 6 | 1 | 14 | 22 | 2 | 3 | 33.4 | 1.8 | 2.3 | 0.2 | 0.2 |
| Other occupational diseases | 686 (6.7) | 47 | 17 | 13 | 45 | 2 | 1 | 53 | 1.7 | 4.6 | 0.2 | 0.1 |
| Total |
10,233 (100) | 382 (3.7) | 176 (1.7) | 203 (2) | 379 (3.7) | 27 (0.2) | 59 (0.6) | 790.3 | 26.4 | 39.1 | 2.3 | 4.6 |
| No. of new cases | Years of exposure, mean ± SD | p-value | |
|---|---|---|---|
| Occupational respiratory diseases | <0.001 | ||
| Anthracosis, anthracosilicosis (J60) | 1,049 | 15.1 ± 5.3 | |
| Silicosis (J62) | 659 | 13.6 ± 4.9 | |
| Siderosis and cementosis (J63) | 67 | 17.4 ± 5.4 | |
| Silicotuberculosis (J65) | 29 | 14.9 ± 6.5 | |
| Chronic bronchitis (J68) | 4,027 | 15.3 ± 5.4 | |
| Asthma (J68.4) | 41 | 14.9 ± 5.9 | |
| Occupational toxicities | <0.001 | ||
| Poisoning by organic solvents (T52) | 381 | 17.1 ± 6.3 | |
| Poisoning by aromatic compounds (T53) | 2 | 14 ± 2.8 | |
| Poisoning by heavy metals (T56) | 146 | 17.7 ± 6.5 | |
| Poisoning by inorganic compounds (T57) | 7 | 20.7 ± 10.7 | |
| Acute carbon monoxide poisoning (T58) | 222 | 9.3 ± 5.7 | |
| Poisoning by irritant and asphyxiant gases (T59) | 52 | 18.8 ± 7.4 | |
| Pesticide poisoning (T60) | 2 | 15 ± 1.4 | |
| Occupational neurological disorders | 0.597 | ||
| Vibration-induced disorder (T75) | 28 | 16.9 ± 5.7 | |
| Radiation-induced neurological disorder (W85) | 9 | 16.3 ± 6.2 | |
| Lumbar and lumbosacral spine disorders (G54) | 1,622 | 17.7 ± 5.6 |
| Occupational respiratory diseases | 1975 | 1985 | 1995 | 2005 | 2015 | 2023 |
|---|---|---|---|---|---|---|
| Anthracosis, anthracosilicosis | 137 (52.1) | 23 (16.3) | 3 (3.2) | 3 (2.2) | 0 (0) | 1 (5.9) |
| Silicosis | 83 (31.6) | 26 (18.4) | 1 (1.1) | 0 (0) | 6 (50.0) | 6 (35.3) |
| Siderosis and cementosis | 4 (1.5) | 0 (0) | 0 (0) | 1 (0.7) | 1 (8.3) | 1 (5.9) |
| Silicotuberculosis | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 2 (16.7) | 0 (0) |
| Chronic bronchitis | 28 (10.6) | 92 (65.2) | 90 (95.7) | 131 (97.0) | 3 (25.0) | 8 (47.1) |
| Asthma | 11 (4.2) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (5.9) |
Table 1. Distribution of predominant occupational diseases by organ system, 1975–2023
Incidence per 100,000 workers calculated for selected years 1995, 2005, 2015, 2023; Values in parentheses indicate the percentage of total cases (n = 10,233), calculated based on the overall study population across all years.
Table 2. Comparison of confirmed occupational disease cases by years of exposure to hazardous conditions, 1992–2023
SD: standard deviation.
Table 3. Dust- and particulate-induced respiratory disease cases, 1975–2023
Values are presented as number (%).

