
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 35; 2023 > Article
-
[Special Collection] Working hours as a social determinants of workers' health
Special Article Problems and suggested improvement plans for occupational health service in Korea -
Dongmug Kang1,2,3

-
Annals of Occupational and Environmental Medicine 2023;35:e10.
DOI: https://doi.org/10.35371/aoem.2023.35.e10
Published online: May 11, 2023
1Department of Preventive, and Occupational & Environmental Medicine, School of Medicine, Pusan National University, Busan, Korea.
2Department of Occupational and Environmental Medicine, Pusan National University Yangsan Hospital, Yangsan, Korea.
3Research Institute for Convergence of Biomedical Science and Technology, Pusan National University Yangsan Hospital, Yangsan, Korea.
- Correspondence: Dongmug Kang, MD, MPH, PhD. Department of Preventive, and Occupational & Environmental Medicine, School of Medicine, Pusan National University, 49 Busandaehak-ro, Mulgeum-eup, Yangsan 50612, Korea. kangdm@pusan.ac.kr
• Received: April 3, 2023 • Revised: April 19, 2023 • Accepted: May 1, 2023
Copyright © 2023 Korean Society of Occupational & Environmental Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
- The purpose of this paper was to review the problems relating to Korea’s occupational health services and suggest ways to improve them. Korea can be classified as a welfare state type of conservative corporatism partially interwoven with liberalism. While experiencing compressed economic growth, the economic sectors of developed (excess areas) and developing (deficient areas) countries are interwoven. Therefore, it is necessary to perfect conservative corporatism along with a complementary reinforcement of liberal contents and to apply a multilayered approach focusing on complementing the deficient areas. It is essential to form a national representative indicator related to occupational health, and a strategy for selection and concentration is needed. The proposed central indicator is the occupational health coverage rate (OHCR), which is the number of workers who have applied for mandatory occupational health services under the Occupational Safety and Health Act in the numerator with the total working population in the denominator. This paper proposes ways to raise the OHCR, which is currently at the level of 25%–40%, to 70%–80%, which is the level of Japan, Germany, and France. To achieve this target, it is necessary to focus on small businesses and vulnerable workers. This is an area of market failure and requires the active input of community-oriented public resources. For access to larger workplaces, the marketability of services should be strengthened and personal intervention using digital health resources should be actively attempted. Taking a national perspective, work environment improvement committees with tripartite (labor, management, and government) participation for improvement of the working environment need to be established at the center and in the regions. Through this, prevention funds linked to industrial accident compensation and prevention could be used efficiently. A national chemical substance management system must be established to monitor the health of workers and the general public.
The occupational health system is a framework of laws, institutions, and services. The author intends to review the major issues relating to Korea’s occupational health system and services from an overall perspective and propose methods for improvement.1 To help readers understand this manuscript better, the Korean version paper (Supplementary Data 1) and the presentation file (Supplementary Data 2) presented in a policy forum are attached.1
STATUS AND MAJOR ISSUES WITH THE KOREAN OCCUPATIONAL HEALTH SERVICE
The content and form of the Korean occupational health system could be defined by the type of national welfare regime. If Korea is categorized according to the Esping-Anderson classification of welfare states,2 it would fall under the Southern European conservative corporatism category partially interwoven with liberalism. Given that the development of a welfare state is path-dependent, Korea’s occupational health system has also developed in a path-dependent manner, and it is highly likely that its future direction will also be the same. On the other hand, Korea’s economic growth has progressed in a very compressed manner. This has resulted in the country having an unorganized mix of the developing and developed aspects of society. This confusion due to the compressed growth can be seen in the occupational health system, too. From this point of view, the problem of the Korean occupational health system could be summarized as being a mixture of the characteristics of developing and advanced economic sectors along with the incomplete growth of conservative corporatism which is a leading part of the Korean welfare state type, and further compounded with a dash of liberalism. This situation was not the result of adding liberal elements to address the structural problems of the system while fulfilling institutional fidelity through the high-quality growth of conservative corporatism. There could be a strong tendency to avoid the problem by squeezing the balloon which merely shifts the problem rather than solving it. Also, although various stages of development coexist without problem-solving, the system has a strong tendency to cover up the need for problem-solving in other stages by foregrounding one stage of development. Therefore, it is important to improve the completeness of conservative corporatism, not as an alternative, but as a complement to the introduction of liberal systems. Also, a multilayered approach is needed, and a universal single approach is inappropriate as a problem-solving method. Layered methods with traditional occupational health approaches for the developing economic sectors (deficient areas) in combination with advanced techniques for the developed economic sectors (excess areas) are needed. To take up another aspect, governance consists of the state (government), the market, and civil society, and the problems of the current occupational health system would have areas of government failure, market failure, and civil society (expert) failure.
The term industrial health began to be widely used in the late 19th century to promote health and hygiene for industrial workers. The focus was on the primary and secondary industries. The first International Congress on Industrial Health was held in Milan, Italy in 1910.3 Subsequently, in 1919, the International Labor Organization (ILO) began to create labor standards related to industrial hygiene and occupational health, and the term industrial medicine began to be widely used in the 1920s and 30s. Since the 1980s, the ILO has shifted its focus from industrial hygiene to occupational health in an attempt to include a wider range of problems seen in the workplace. Since then, the recommendations of the ILO Conventions 161 (1985) and 171 (1995) on occupational health service organizations and delivery have all used the term occupational health. Recently in 2007, the World Health Organization (WHO) used the term ‘workers’ health’ in its global plan of action (GPA) to address a wider range of issues. On the other hand, in Korea, the term ‘industrial health’ in the Korean language still shows a regressive tendency to limit the scope to the traditional industrial field. It continues to focus on primary and secondary industry problems without accepting changes in concepts that have been developed historically while expanding the scope. Specifically, it is necessary to improve the terms used at present when the scope and boundaries of traditional employers have become ambiguous; such as the current expansion of platform labor. The terms ‘workers’ health’ or ‘occupational health’ would be the minimally acceptable terms at this point.
The author believes that among the relatively recent strategies implemented in countries across the world, the shortcomings in the Korean occupational health services may be described as follows: The GPA includes the following clauses: Clause16: Integrating occupational health services into national health strategies, setting targets to increase the coverage of the working population receiving occupational health services, and creating mechanisms for delivering occupational health services; Clause17: Establishing organs at the central and local levels, respectively. The BOHS stipulates that occupational health services need to meet regional needs and conditions to make them available to all workers (including self-employed and precarious workers). As mentioned above, a multilayer approach should be applied rather than merely focusing on a universal approach based on stages I, II, III, or IV of the BOHS. Small businesses and vulnerable workers need to be covered in stage I with public resources. It is also worth noting that Stage I’s resources comprise nurses and hygienists but not physicians.
Compared to the national occupational safety and health system model proposed by the ILO, Korea’s occupational health services lack design, production, import, and control over suppliers (Fig. 1).4 Also, they are deficient in the areas of research, academic base, and supervisory authority. The administration of these services involves tripartite cooperation between labor, management, and the government, which is also insufficient, resulting in a lack of reporting, recording (monitoring), and statistics (production and presentation) of accident/disease data. Compared to indicators such as those used by the European Union (EU), the International Social Security Association (ISSA), WHO, and ILO, Korea is deficient in the following areas: 1) Punishment in the legal/supervisory area (average fine, number of convictions), labor supervisors per 1,000 people. 2) Management participation in the leadership area. 3) Number of complaints, and number of work stoppages in the area of employee participation. 4) Industrial accidents in the area of results: ratio of compensation for 30 days or more of sick leave. 5) The number of statistics, surveys, and research institutions in the area of infrastructure. 6) Loss due to disasters, investment costs, etc. in the area of prevention costs. 7) Subcontract management in the area of contracts, etc. These are mainly related to the legislation and enforcement of laws, which were based on the concepts of conservative corporatism. Thus, the majority of these problems could be solved by the faithful implementation of conservative corporatism. The industrial accident status is the representative index of Korea’s occupational health in the e-country index. This indicator suffers from the deficiency that preventability, reliability, and usability are low and it is difficult to use in the field. Chemical substance management indicators (carcinogenic, mutagenic, reprotoxic [CMR], substance distribution and material safety data sheets [MSDS], etc.) have been proposed in relation to the environmental improvement of the workplace, and it is necessary to form a national central index and strengthen research institutes with the responsibility for monitoring and feedback.
There are a few studies that have reviewed the overall content and budget of Korean occupational health services.5 According to them, Korea's industrial accident prevention investment by gross domestic product (GDP) is higher than that of the United States and Japan, but smaller than that of Germany. However, Korea’s industrial accident prevention loan program to finance industrial accident prevention facilities has the major task of preventing industrial accidents but is merely an optical illusion without actual achievements. There are many types of government and public occupational health services, but there are no goal-based strategies, and there is also no system to regularly monitor the relevant indicators and provide feedback to the Ministry of Economy and Finance.
Small workplaces in Korea account for 98% of the total number of workplaces, 51% of employment insurance subscribers, 77% of industrial accidents, and 62% of industrial accident deaths. Despite this importance, it is estimated that in Korea, the occupational health coverage rate (OHCR), which is the ratio of the number of workers who have applied for mandatory occupational health services under the Occupational Safety and Health Act in the numerator with the total working population in the denominator, is 80% for workplaces with 50 or more employees, compared to 25% to 40% for small workplaces. What is more problematic is that the systematic collection of information on vulnerable workers is not being carried out. Government-supported projects for small workplaces in Korea include support for the creation of clean workplaces, loans to industrial accident prevention facilities, work environment measurement and reimbursement of special health examination costs, and operation of workers' health centers. In addition, small-scale workplace safety management and chemical accident prevention, construction site disaster prevention, and health management technology are supported through private-sector transfers. However, as mentioned above, the problem with these measures is their lack of relevance. Also, this is not an approach that can solve the problems of small businesses but merely a means to increase the count of beneficiaries as required by the law. When the required count is reached, the measures are terminated. Hence continuous and in-depth support is not possible. These measures lack planning and evaluation, feedback, and course correction.
Among the current occupational health services in workplaces identified through a survey,6 the areas highlighted as the most inadequate were the tasks to be carried out by the Occupational Safety and Health Commission, the selection of workplace designs and machines, work plans and organizational recommendations, participation in work implementation programs, and evaluation of new tools. Medical checkups were an area of market failure as they offered one-sided products that were not based on the needs of consumers in the workplace and involved only checkups without interventions. A marketable product is one that a supplier sells based on the demand of the consumer, and cheap and high-quality products sell well. While the health checkup system functions as a product of the market, the reality is that consumers are not sensitive to the quality of the products supplied, and regard them as just the clearance costs necessary to run their businesses. In addition, there is little differentiation between tertiary acute general hospitals and clinic-level services. The Dutch slogan “no intervention, no screening!” is highly applicable, and it is necessary to introduce interventions that address workers’ health issues as proposed by the GPA. Problems with the work environment monitoring system include the lack of uniform services, limited available expertise, lack of independence from employers, exclusion of certain parties, regulatory dependence, and inefficient management systems. To overcome this, total work environment management which includes improvement activities has been proposed. Alternatives include measures to strengthen integrated health management (including environmental monitoring, special health check-ups, and health management) proposed at the 2018 meeting of the Ministry of Employment and Labor. This would secure the reliability of work environment monitoring and the pursuit of integrated health management and ensure that the worker's right to know is respected. In addition, workplace intervention to improve the working environment is also an important issue.
PROPOSAL FOR IMPROVEMENT MEASURES
We live in the era of the 4th industrial revolution. The core of future medical care can be summarized as 4Ps (prediction, prevention, precision, participation). Therefore, prevention, a core area of occupational health, can be implemented using prediction with precision based on participation. In other words, if public health has been targeting groups so far, public health in the future needs to implement personalized precision public health measures in addition to group measures, which means that group and individual interventions must be performed at the same time. In the field of occupational health, it is necessary to combine interventions at the workplace centered on the improvement of the working environment with individually tailored interventions that include precision and addressing in real-time personal life habits such as alcohol drinking, smoking, exercise, diet, and maintaining a lifelog that specifies the characteristics of individuals. One of the problems of Korea’s health care delivery system so far has been the lack of community-based primary care, but by using digital health combined with community resources such as public health centers, it is possible to strengthen primary care and make the delivery system more efficient. Several possibilities are opening up in this regard. In the field of occupational health, when data is generated through digital health equipment for local workplaces and workers and sent to the joint cloud center in real time, tertiary institutions can create content through research, education, and guidance. Primary and secondary agencies can provide services to workplaces and individual workers. In this case, interventions for both groups and individuals are possible. If personal intervention techniques using digital health are developed in the field of occupational health, it would become necessary to create a health insurance fee for service items.
Chemical substance management in Korea is conducted in accordance with the Chemicals Registration and Evaluation Act and the Chemicals Management Act, which are under the jurisdiction of the Ministry of Environment. The Occupational Safety and Health Act, which is under the jurisdiction of the Ministry of Employment and Labor, also has a chemical management system, but it is applied only to the inside of the workplace. If the MSDS is incorrect, there may be a situation where employers are not even aware that a problem exists. The case of D Chem, which occurred in 2022, is such an example. Considering that the current statistics on carcinogen consumption at the national level in Korea are announced by the Ministry of Environment, not the Ministry of Employment and Labor, the cooperation of the Ministry of Environment is required for the national management of chemical substances. To identify and prevent the exposure of field workers to chemical substances and the health problems of the people who are actual users of the chemical products, management at the national level must be linked to workplace management. It is known that the Ministry of Environment and the Ministry of Employment and Labor are currently discussing the introduction of a lower-level employer as well as a producer or importer liability system. Therefore, at least the production, distribution, and consumption of chemicals containing CMR substances must be managed comprehensively at the national, workplace, and end-user levels to prevent worker exposure and monitor the health of the end users.
The main contents are presented in Table 1.
Aspects of traditional occupational health
Occupational health services currently implemented in Korea include the measurement of the work environment, examination of worker health, risk assessment, musculoskeletal hazard survey, cardiovascular disease prevention, job stress, and emotional labor management. In addition to these projects, more services are needed as follows: 1) Assessment of the suitability for work. 2) Assessment of the suitability to return to work. 3) Participation of the occupational physician (or occupational health personnel) in production/process/work and machine/equipment/substance introduction management. 4) 1st, 2nd, and 3rd care for prolonged work/stress/mental health prevention. 5) Employment/fitness for work for the disabled. 6) Integrated management of measurement/examination/health management, etc.
Aspects relating to workers’ health
So far, Korea has lacked the approach to workers' health recommended by the WHO in the GPA. In the future, this area will occupy a very large part of the total services. Therefore, it is necessary to preemptively prepare for the content and delivery method for these services. Specifically, the following need to be addressed: 1) Approval/management of sick leave. 2) Management of cancer patients (many non-occupational cancer cases). 3) Management of mental health, and 4) Chronic disease management and intervention.
Perfecting institutional conservative corporatism
As Korea is based on conservative corporatism, the most important task would be to improve the level of implementation. The main countries based on conservative corporatism are Germany, France, and Japan, and it is necessary to raise Korea to the levels achieved by these countries as the main goal. The requirements for this are as follows: 1) Expansion of the scope of labor inspectors, improvement of professionalism, and tight law enforcement. 2) Improvement of occupational health coverage (Germany 90%, France 90%, Japan 75%). 3) Strengthening of the authority of occupational physicians (OP, in Italy, it is the employer's legal duty to accept the OP’s recommendation). 4) Guarantee of professional independence of the OP by law (France, Japan). 5) Appointment of community-based occupational health practitioners for small businesses (for all workers) (Japan). 6) Right to participate in worker/labor unions (Italy).
Institutional supplementation of the aspect of liberalism
Representative liberal occupational health services implemented in Korea are covered by the Risk Assessment and Serious Disaster Punishment Act. As mentioned earlier, the basis of Korea’s occupational health system is conservative corporatism. To address the deficiencies in this system, it is necessary to introduce another system to supplement it while enhancing the completeness of the foundation, rather than changing to another system altogether. It should be noted that otherwise, drifting between different types of institutional systems may end up avoiding problems. The scope of system supplementation from the liberal aspect is as follows: 1) Ensuring the effectiveness of risk assessment, strengthening the status of risk assessment in connection with the expansion of the influence of the Chemical Substances Evaluation Act. 2) Spreading the social culture of prevention through the Serious Disaster Punishment Act. 3) Implementing good occupational health guidelines (e.g., Finland, Netherlands).
Implementation at the national, government level
The challenges to be addressed at the national level include the following: 1) Establishing occupational health improvement as a key national task: financing and allocation of the necessary resources, and index and indicator management based on long-term goals. 2) Establishment of an integrated management system for hazardous substances: management of CMR substance handling workplaces based on production/distribution/handling/consumption supply chains. 3) National regional organization establishment: delivery system according to the level of service difficulty. 4) Establishment of statistics generating, policy implementing, evaluation, and feedback systems, and expansion of independent research institutes. 5) Connection between prevention and compensation: If experts determine that work environment improvement is necessary on their workplace visits for an accident investigation or for permitting a return to work, a system should be implemented that links such decisions to the clean workplace creation support project or the safety and health technology support project by Korea Occupational Safety and Health Agency.
The main contents are presented in Fig. 2.
An occupational health service delivery system can be established according to the difficulty of the task or based on the risk involved. As mentioned above, Korea’s occupational health services operate on a single format without taking into account the existing diversity in the vulnerable classes and sizes of corporations caused by the country’s compressed economic growth. For this reason, large corporations with their own systems feel that the level of medical check-ups and work environment monitoring is low. On the other hand, the underprivileged and small businesses do not benefit at all. Therefore, active intervention from the public sector is required for small businesses or vulnerable workers whose access to occupational health services is limited. Given that there are 256 public health centers in each region across the country, it is possible to establish the same number of occupational health community support centers to provide public access to small-scale and vulnerable workers. These regional support centers could be operated by nurses and hygienists, who are the primary units of the BOHS and can be managed by placing a higher-level guidance unit. This is also a way for senior guidance units to strengthen workers' health centers. On the other hand, the field of occupational health services needs to strengthen its market function through the creation of marketable products that sell well in the private sector. Here, a qualitative improvement could be induced in response to the demand at the workplace. This could be done by focusing on individual intervention with a precision public health approach using digital health, and adopting high-quality products through market competition. Occupational health services based on digital health will be split into roles such as big data analysis, preparation of service content and provision of guidelines by tertiary institutions, and service provision by the primary and secondary institutions.
To create a structure that includes workplace intervention and the linkage of industrial accident compensation and prevention, it is necessary to establish central and local workplace improvement intervention committees based on tripartite participation by labor, management, and the government. These workplace improvement intervention committees can use industrial accident data to determine the priority of distribution of prevention-related finances, such as the industrial accident fund. For this nationwide financial distribution and prioritization, the priority selection of data such as chemical distribution data and industrial accident statistics, and feedback mechanisms should be strengthened. A central research institute should be established for national data analysis which may assist the workplace intervention committees.
Abbreviations
BOHS
Basic Occupational Health Services
CMR
carcinogenic, mutagenic, reprotoxic
EU
European Union
GDP
gross domestic product
GPA
global plan of action
ILO
International Labor Organization
MSDS
material safety data sheets
OHCR
occupational health coverage rate
WHO
World Health Organization
-
Funding: This research was supported by a 2-year Research Grant of Pusan National University.
-
Competing interests: The authors declare that they have no competing interests.
NOTES
SUPPLEMENTARY MATERIALS
- 1. Ku JW, Kim HR, Kang DM, Lee JI, Ryu HC, Yoon GW, et al. A Study on Countermeasures According to Changes in the Industrial Health Environment (Policy Forum). Ulsan, Korea: Korea Occupational Safety and Health Agency; 2022, 1–132.
- 2. Esping-Andersen G. Three political economies of the welfare state. Int J Sociol 1990;20(3):92–123.
- 3. Harrison WJ. The historical development of industrial hygiene. Am J Public Health (N Y) 1913;3(6):540–546.
- 4. Cho YH. Study on Development of National Occupational Safety and Health Indicators. Ulsan, Korea: Korea Occupational Safety and Health Agency; 2021, 1–161.
- 5. Yoon JD, Park YS, Ko BI, Jung YH, Jeon KJ. A Study on the Present Condition of the National Safety Budget and the Analysis of the Outcome of the Main Projects of Occupational Accident Prevention in Other Countries. Ulsan, Korea: Korea Occupational Safety and Health Agency; 2015, 1–216.
- 6. Lee SI. A Survey of Actual Condition of Occupational Health Services in Manufacturing Industry. Ulsan, Korea: Korea Occupational Safety and Health Agency; 2008, 1–285.
REFERENCES
REFERENCES
Fig. 1
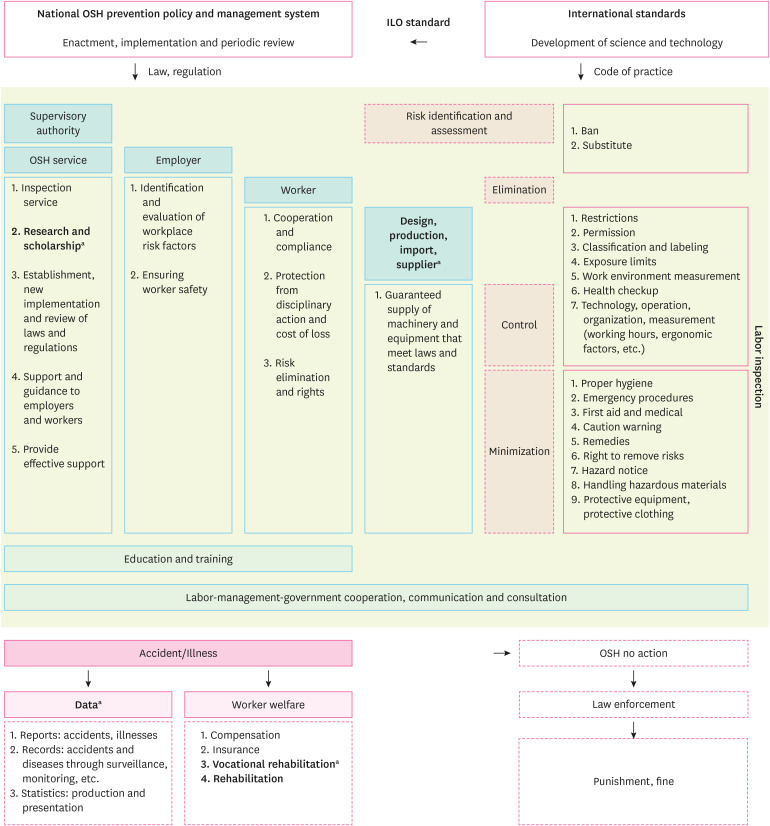
Proposed occupational health service delivery system.
OSH: Occupational Safety and Health; ILO: International Labor Organization.
aDeficient areas in Korea.
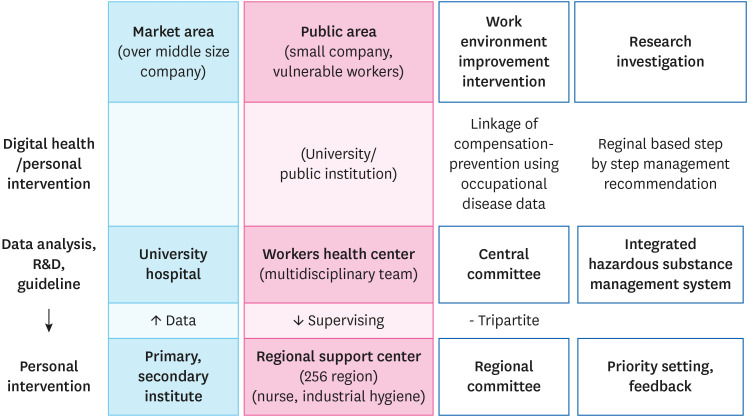
Table 1
Proposed Items to improve occupational health services in Korea
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Assessing Quality Gap of the Employee Critical Illness Mutual Aid Fund Using the SERQUAL Model
Lin Lu, Hui Sun, Weixin Zhang, Hannah Wesley
Advances in Public Health.2026;[Epub] CrossRef - Perspectives from the new president of the Korean Society of Occupational and Environmental Medicine: future strategies for occupational and environmental medicine
Sang Baek Ko
Ann Occup Environ Med.2025; 37: e1. CrossRef - Occupational disease monitoring by the Korea Occupational Disease
Surveillance Center: a narrative review
Dong-Wook Lee, Inah Kim, Jungho Hwang, Sunhaeng Choi, Tae-Won Jang, Insung Chung, Hwan-Cheol Kim, Jaebum Park, Jungwon Kim, Kyoung Sook Jeong, Youngki Kim, Eun-Soo Lee, Yangwoo Kim, Inchul Jeong, Hyunjeong Oh, Hyeoncheol Oh, Jea Chul Ha, Jeehee Min, Chul
The Ewha Medical Journal.2025;[Epub] CrossRef - Challenges from 14 years of experience at Workers' Health
Centers in basic occupational health services for micro and small enterprises in
Korea: a narrative review
Jeong-Ok Kong, Yeongchull Choi, Seonhee Yang, Kyunghee Jung-Choi
The Ewha Medical Journal.2025;[Epub] CrossRef - Association of Precarious Employment With Unmet Healthcare Needs and Health Checkup Participation
Seong-Uk Baek, Jin-Ha Yoon
American Journal of Preventive Medicine.2025; 68(6): 1120. CrossRef - Association Between Precarious Employment and Cognitive Decline: A Longitudinal Study of Middle-Aged and Older Workers in Korea
Seong-Uk Baek, Jin-Ha Yoon
Journal of General Internal Medicine.2025; 40(10): 2292. CrossRef - Precarious Employment Typologies and Psychotropic Medication Use and Misuse
Seong-Uk Baek, Jin-Ha Yoon
American Journal of Preventive Medicine.2025; 69(6): 108064. CrossRef - Precarious employment and the onset of depressive symptoms and problematic alcohol use in middle-aged or older workers: A Korean longitudinal study (2006–2022)
Seong-Uk Baek, Yu-Min Lee, Jong-Uk Won, Jin-Ha Yoon
Social Science & Medicine.2024; 357: 117170. CrossRef - Association of precarious employment with depressive symptoms and suicidal ideation among female workers: Findings from a nationwide longitudinal study in Korea
Seong-Uk Baek, Yu-Min Lee, Jin-Ha Yoon
Journal of Affective Disorders.2024; 351: 931. CrossRef - Association between precarious employment and the onset of depressive symptoms in men and women: a 13-year longitudinal analysis in Korea (2009–2022)
Seong-Uk Baek, Jong-Uk Won, Yu-Min Lee, Jin-Ha Yoon
Epidemiology and Psychiatric Sciences.2024;[Epub] CrossRef - Association between life satisfaction, self-esteem, and health checkup participation: A population-based longitudinal study in South Korea
Seong-Uk Baek, Jin-Ha Yoon
Preventive Medicine.2024; 189: 108127. CrossRef - Multidimensional typologies of precarious employment and their relationships with mental well-being in Korean wageworkers: A latent class analysis based on the Korean Working Conditions Survey (2020–2021)
Seong-Uk Baek, Jong-Uk Won, Jin-Ha Yoon
Preventive Medicine.2023; 177: 107787. CrossRef
 Cite
CiteProblems and suggested improvement plans for occupational health service in Korea
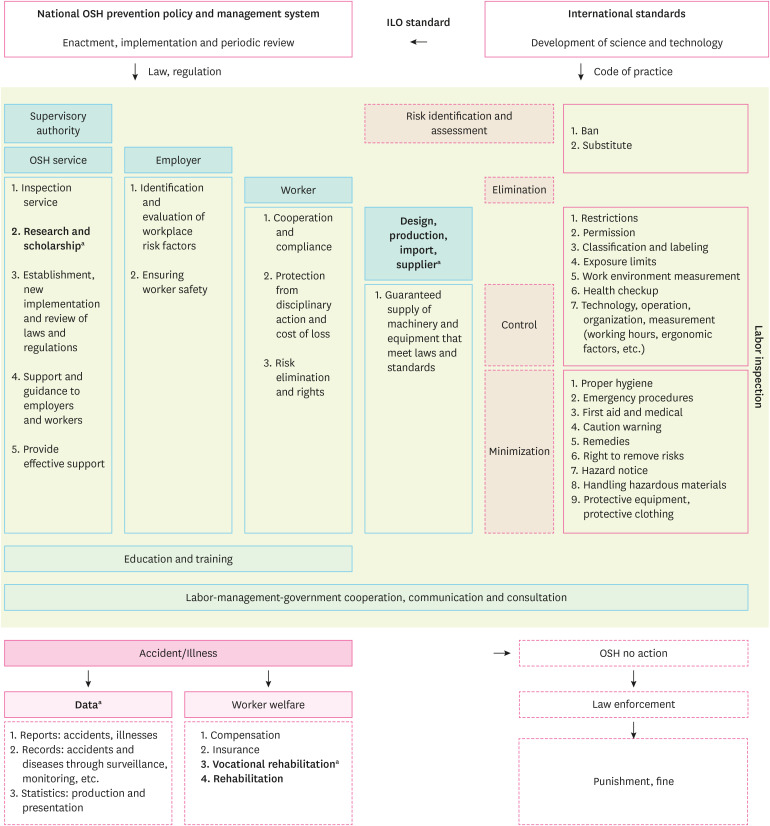
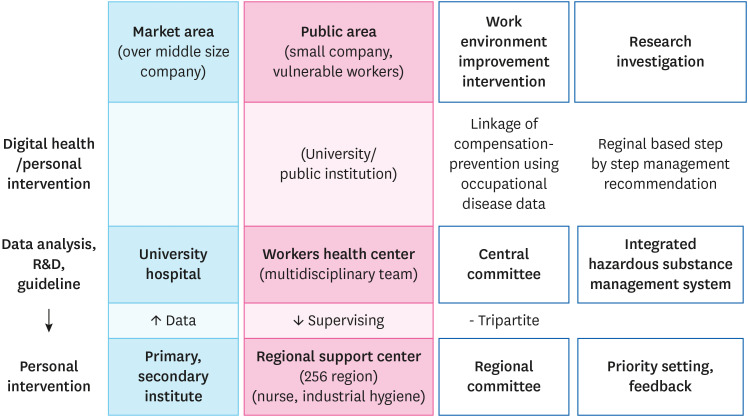
Fig. 1 Proposed occupational health service delivery system.OSH: Occupational Safety and Health; ILO: International Labor Organization.aDeficient areas in Korea.
Fig. 2 Proposed Korean occupational health service delivery system.
Fig. 1
Fig. 2
Problems and suggested improvement plans for occupational health service in Korea
| Occupational health aspect | Workers health aspect | Work & health aspect | Improvement of institutional implementation of conservative-corporatism | Institutional supplementation of the liberal aspect | Government level |
|---|---|---|---|---|---|
| ① Fit for work (evaluation and intervention) | ① Approval/management of sick leave | ① Monitoring of changes in labor patterns | ① Expanding the scope of labor supervisors and enhancing professionalism, tighter law enforcement | ① Ensuring the effectiveness of risk assessment: strengthening the status of risk assessment in conjunction with expanding the influence of the Act on the Registration and Evaluation of Chemical Substances | ① Entry into key areas of the country: based on long-term goals fiscal concentration and indicator management |
| ② Return to work (evaluation and intervention) | ② Cancer patient care (health, fitness, return) | ② Platform (online aspect) | ② Increasing occupational health coverage rate (France 90, Germany 90, Japan 75) | ② Spreading social culture through the Serious Disaster Punishment Act | ② Establishment of an integrated hazardous substance management system: production/distribution/handling/consumption/supply chain |
| ③ Production/Process/Work & introduction of machinery/equipment/materials/participation in management | ③ Mental health (OECD recommendations) | ③ Regional unit service-providing resources (offline aspect) | ③ Strengthening of workplace intervention authority (obligation to implement occupational physician recommendations): Italy | ③ Good OH Guidelines (Finland, Netherlands, etc.) | ③ Establishment of regional organizations nationwide: establishment of a delivery system |
| ④ Prolonged work /stress/mental health (1/2/3) Prevention, Interview (Japan) | ④ Chronic disease management and intervention | ④ Act to ensure occupational physician’s professional independence (France, Japan) | ④ Establishment of statistics, policies, evaluation, and feedback systems: expansion of independent research institutes | ||
| ⑤ Disabled employment/adjustment | ⑤ Appointment of regional occupational healthcare for all workers (Japan) | ⑤ Occupational disease gatekeeping system | |||
| ⑥ Integrated management of environmental monitoring, health screening, management | ⑥ Workers/labor union participation (Italy) | ⑥ Linkage of prevention and compensation |
Table 1 Proposed Items to improve occupational health services in Korea

