
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 30; 2018 > Article
- Research Article Association between serum ferritin and hypertension according to the working type in Korean men: the fifth Korean National Health and nutrition examination survey 2010–2012
-
Dong-Hoon Lee1, Seong-Kyu Kang1,2
 , Won-Jun Choi1,2, Kyeong Min Kwak1, Dukyun Kang1, Sang Ha Lee1, Jun-Hyung Lee1
, Won-Jun Choi1,2, Kyeong Min Kwak1, Dukyun Kang1, Sang Ha Lee1, Jun-Hyung Lee1 -
Annals of Occupational and Environmental Medicine 2018;30:40.
DOI: https://doi.org/10.1186/s40557-018-0251-y
Published online: June 11, 2018
1Department of Occupational and Environmental Medicine, Gachon University Gil Medical Center, 21 Namdong-daero 774 beon-gil, Namdong-gu, Incheon, 21565 Republic of Korea
2Department of Occupational and Environmental Medicine, College of Medicine, Gachon University, 38-13 Dokjeom-ro 3 beon-gil, Namdongogu, Incheon, 21565 Republic of Korea
• Received: March 8, 2018 • Accepted: May 28, 2018
© The Author(s). 2018
Open AccessThis article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Abstract
-
Background Several studies suggest that serum ferritin concentrations reflect systemic inflammation, and high ferritin levels can increase the risk of hypertension in adult men. Shift work is also known to increase the risk of hypertension; however, there has been no study about the relationship between serum ferritin levels and the prevalence of hypertension according to the working type.
-
Methods This cross-sectional study included 4,442 male participants (3,651 daytime workers and 791 shift workers) who participated in the fifth Korean National Health and Nutrition Examination Survey. Hypertension was defined as a systolic blood pressure greater than or equal to 140 mmHg, a diastolic blood pressure greater than or equal to 90 mmHg or the current use of antihypertensive medications regardless of blood pressure values. For the statistical analyses, serum ferritin levels were reclassified into quartiles, and complex sample analyses were used to evaluate the relationship between serum ferritin levels and the prevalence of hypertension according to the working type in this study.
-
Results Serum ferritin and shift work were positively associated with the prevalence of hypertension. The effect of interaction was above multiplicative. When compared to participants in the lowest serum ferritin quartile, the odds ratio for hypertension for participants in the highest serum ferritin quartile was 1.372 (1.027–1.833) in daytime workers and 2.009 (1.042–3.873) in shift workers after adjustment.
-
Conclusions The prevalence of hypertension increased as ferritin levels increased in individuals, especially in shift workers.
Background
Iron plays an important role in maintaining the body’s physiological homeostasis [1, 2]. Serum ferritin is a sensitive parameter used to assess iron status in the body and is a well-known diagnostic biomarker for iron deficiency [3]. In addition, serum ferritin is known to reflect systemic inflammation as an acute phase reaction, and several studies have shown that inadequately elevated iron stores may adversely affect health outcomes [4–6]. Several studies have shown that elevated serum ferritin levels are associated with insulin resistance and type 2 diabetes [7–9], metabolic syndrome [9–11], dyslipidemia [12], and obesity [13, 14]. The relationship between serum ferritin and hypertension has not been well established in women and has been controversial, but reports have found an association between serum ferritin and hypertension in men [15–18].
According to several studies, results are relatively consistent regarding the relationship between shift work and increased blood pressure [19–21]. The underlying mechanism includes changes in lifestyle factors caused by the disruption of circadian rhythms. This disruption can lead to adverse changes in a person’s life such as higher stress levels including psychosocial, behavioral, and physiological stress. Among the mechanisms of stress come from shift work, physiological stress can induce inflammation [22]. This inflammation plays a critical role in the atherosclerotic process, all stages of atheroma formation, and coronary heart disease [23]. Several studies have explored the association between shift work and the atherosclerotic process. Two studies assessed this association using ultrasound measurements to measure the extent of subclinical atherosclerosis of the carotid intima media. One reported an increased risk of atherosclerosis for shift workers over 45 years of age [24]. The other study focused on younger daytime and shift workers (24–39 years old) but found a similar association in men [25]. A study reported the mechanism to explain the association between shift work and the atherosclerotic process; high sensitive C-reactive protein, high leukocyte and lymphocyte counts, and natural killer cell activity have all been implicated in this process [22].
There has been no study about the relationship between serum ferritin and hypertension according to the working type. This study was based on large-scale national data representative of the population of the Republic of Korea. We conducted this research to investigate the association between serum ferritin levels and hypertension according to the type of work.
Methods
We used data from the fifth Korean National Health and Nutrition Examination Survey (KNHANES) conducted by the Korea Centers for Disease Control and Prevention between 2010 and 2012. In the fifth KNHANES, the survey was conducted by extracting 20 households randomly from 192 regions with approximately 100,000 people over the age of one. People were divided to three groups: pediatric (one to 11 years old), adolescents (12 to 18 years), and adults (19 years or older). The survey was composed of a health interview, health examination, and a nutrition survey [26]. Data is opened to public and is freely available for research purposes.
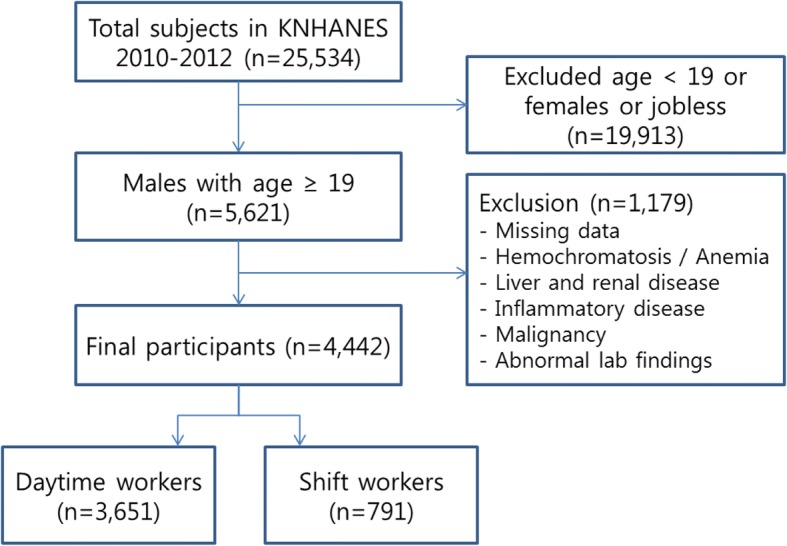
The fifth KNHANES had 25,534 initial participants. We included male workers who were over the age of 19 and who included information on the duty hours section of the health interview survey (n = 5621). We excluded participants if there was missing data on serum ferritin and blood pressure. We also excluded participants who had inflammatory diseases like arthritis, liver cirrhosis, chronic liver disease, chronic renal disease, malignancy or probable hemochromatosis based on serum ferritin levels (> 300 ng/mL for men) [2, 3]. Some participants were excluded if they had anemia or an iron deficiency states; participants with < 13 g/dL hemoglobin (Hb) or < 10 ng/mL ferritin were not included [27]. Participants with serum creatinine (Cr) > 1.4 mg/dL, serum liver enzymes (either aspartate aminotransferase [AST] or alanine aminotransferase [ALT]) > 80 IU/L, or white blood cell (WBC) counts > 10,000 cells/uL was also excluded from the study. After these exclusions, 4442 participants (3651 daytime workers and 791 shift workers) were included in our final analysis (Fig. 1).
The health interview surveys and health examination surveys were completed at mobile health examination centers. The health examination survey assessed body measurements, blood pressure and pulse measurements, various diagnostic examination and etc. The health interview survey assessed various factors such as working hours, disease morbidity, physical impairment, medication use, smoking and alcohol history. Trained medical investigators performed physical examinations following standardized procedures. Height and body weight were measured respectively to the nearest 0.1 cm and 0.1 kg. For the measurements, participants were asked to remove their shoes and dress in disposable examination gowns. Waist circumference (WC) was measured to the nearest 0.1 cm at the midpoint between the lower border of the rib cage and the iliac crest. Body mass index (BMI) was calculated as the ratio of weight/height2 (kg/m2). Blood pressure was measured on the right arm in a sitting position using a standard mercury sphygmomanometer. Blood pressure was measured three times, with a 30s rest between each measurement, and the participant’s blood pressure was calculated as the mean blood pressure of the second and third measurements. Blood samples were obtained from the participants from the antecubital veins after an overnight fast. Serum ferritin concentrations were measured using a 1470 WIZARD gamma-Counter with Immunoradiometric Assay (PerkinElmer/Finland). Total cholesterol (TC), triglycerides, fasting blood sugar (FBS), hemoglobin, total iron binding capacity (TIBC), WBC counts, creatinine, vitamin D (VitD) and liver enzymes (AST and ALT) were also recorded [26]. Alcohol consumption was categorized by frequency of drinking; non-drinkers and occasional drinkers were categorized as those who consumed alcohol ≤1 day/month), and regular drinkers were categorized as those who consumed alcohol ≥2 days/month. Smoking status was categorized as current smoker, former smoker, and never smoker.
Hypertension was defined as a systolic blood pressure (SBP) greater than or equal to 140 mmHg, or a diastolic blood pressure (DBP) greater than or equal to 90 mmHg. Those taking antihypertensive medications were also considered to have hypertension regardless of blood pressure values.
The two working types were classified as “daytime workers” and “shift workers” using the duty hour information collected in the interview. Those who worked from 6 am to 6 pm were consider daytime workers while those who worked from either 2 pm to 12 pm in the evening or 9 pm to 8 am overnight were considered shift workers. Those who indicated that they worked “shift work,” “day and night regular shifts,” “24 hour work shifts,” “split work,” or “irregular shift work” were categorized as shift workers.
Complex sample analyses were used for the KNHANES data for weighting all values following the guidance of statistics from the Korea Centers for Disease Control and Prevention in this study [26]. The data were sorted into quartiles based on serum ferritin concentrations for participants: quartile 1, ≤ 66.82 ng/mL; quartile 2, 66.83–100.78 ng/mL; quartile 3, 100.79–149.13 ng/mL; and quartile 4, > 149.13 ng/mL. General characteristics of participants were derived by a descriptive method for continuous variables and Chi-square test for categorical variables after data weighting. A general linear model was applied to compare continuous variables according to the quartiles of serum ferritin. The interaction of serum ferritin and working type on the prevalence of hypertension was evaluated by logistic regression analysis after adjustment for age, FBS, TC, TIBC, BMI, smoking status and alcohol consumption. In addition, a logistic regression analysis with adjustment was conducted to examine the association between serum ferritin and the prevalence of hypertension after stratifying the working type into daytime workers and shift workers. Data were analyzed using SPSS 20.0 (SPSS, Chicago, IL) to account for the complex sampling design.
Results
The general and clinical characteristics of the study participants according to the quartile groups of serum ferritin levels are presented in Table 1. Prevalence of hypertension increased as the serum ferritin quartile increased. The TIBC concentrations and age tended to decrease with increasing serum ferritin quartiles. There were no significant differences in VitD and SBP.
Table 1
General and clinical characteristics according to the quartiles of serum ferritin
Data are presented as the mean (standard deviation), or numbers (percentages)
SBP systolic blood pressure, DBP diastolic blood pressure, WC waist circumference, BMI body mass index, FBS fasting blood sugar, TC total cholesterol, AST aspartate transaminase, ALT alanine transaminase, Hb hemoglobin, TIBC total iron-binding capacity, Cr creatinine, WBC white blood cell, VitD vitamin D
Table 2 presents the odds ratio (OR) and 95% confidence interval (CI) for the prevalence of hypertension according to the interaction of serum ferritin and working type after adjustment for age, FBS, TC, TIBC, BMI, alcohol consumption and smoking status. The reference group consisted of daytime workers who were found to have the lowest quartile of baseline serum ferritin levels. Comparing to the reference group which was the lowest quartile of serum ferritin levels, the OR and 95% CI for hypertension of the highest quartile of serum ferritin levels in daytime workers was 1.426 (95% CI 1.066–1.906). In addition, the OR and 95% CI for hypertension were evaluated with the highest quartile of serum ferritin levels in shift workers comparing to the reference group, and the value was 1.696 (95% CI 1.083–2.658).
Table 2
Odds ratios (95% CI) for the prevalence of hypertension according to the interaction of serum ferritin and working type
| Variables | Odds ratio (95% confidence intervals)a | |
|---|---|---|
| Quartile 1 (≤ 66.82) | Quartile 4 (> 149.13) | |
| Daytime workers | 1.000 (ref.) | 1.426 (1.066–1.906) |
| Shift workers | 1.035 (0.680–1.576) | 1.696 (1.083–2.658) |
Table 3 shows that OR and 95% CI for the prevalence of hypertension according to the quartile groups of serum ferritin levels in the daytime workers and shift workers. With unadjusted variables, only serum ferritin levels correlated with the prevalence of hypertension. After all variables were adjusted, the adjusted ORs for hypertension comparing the highest quartile of baseline serum ferritin level with the lowest quartile were 1.372 (95% CI 1.027–1.833) in daytime workers, and 2.009 (95% CI 1.042–3.873) in shift workers, respectively.
Table 3
Odds ratios (95% CI) for the prevalence of hypertension according to the quartile groups of serum ferritin levels in each daytime workers and shift workers
Discussion
This cross-sectional study was conducted to determine the association between serum ferritin level and hypertension according to the type of work in male, using large-scale national data representative of the population. This study showed the risk of having hypertension was greater in shift workers than in daytime workers as serum ferritin levels increased.
Some studies have consistently reported significant associations between hypertension and serum ferritin level in men [15–18]. Two of these studies were cross-sectional studies [15, 17], and others were longitudinal studies [16, 18]. According to a recent study, 7104 healthy Korean men who visited a health examination center were surveyed to assess hypertension incidence from 2005 to 2010. An elevated serum ferritin level was found to be independently associated with the incidental risk for hypertension [18].
There is insufficient evidence to explain the underlying mechanism. There are several possible mechanisms about the association between serum ferritin levels and hypertension. One of which includes the development of atherosclerosis by elevated ferritin levels. Ferritin is a ubiquitous intracellular protein that is the key to controlling iron homeostasis and is a widely used biomarker for the diagnosis of iron deficiency [1–3]. Serum ferritin concentrations reflect not only body iron stores but also systemic inflammation [4–6]. Inadequately elevated body iron as oxidative stress can convert less reactive free radicals to more reactive hydroxyl radicals. Elevated body iron can also cause damage to cellular membranes, lipids, proteins, and deoxyribonucleic acid (DNA) [28]. Elevation of ferritin causes oxidative stress, which leads to inflammation, endothelial damage and consequently atherosclerosis. Atherosclerosis process follows after, and then risk of hypertension can be increased. Experimental studies have shown that hypertension is associated with oxidative stress that can contribute to endothelial dysfunction and leads to BP elevation [29].
Many reports and studies over the past several decades have suggested that the endogenous circadian rhythm can collapse due to the effects of shift work on health and ultimately to the destruction of biological homeostasis [22, 30–32]. In a review article, it was reported that the disruption of the circadian rhythm by shift work can lead to psychosocial, behavioral, and physiological stress, which are associated with an increased risk of cardiovascular diseases such as metabolic syndrome, diabetes, and hypertension [22].
Inflammation has a relationship with prevalent and/or incident hypertension and is also related to the ferritin level, which is also known as a positive inflammatory marker [16]. Furthermore, physiological stress due to circadian disruption among shift workers can aggravate inflammation, which is related to cardiovascular disease [22]. We hypothesized that interactions between shift work and serum ferritin would have an impact on the prevalence of hypertension. Our results showed that the OR for hypertension increased in shift workers with the highest quartile of serum ferritin levels when compared to daytime workers with the lowest quartile of serum ferritin levels as expected. After stratification, the OR for prevalence of hypertension was found to be higher in shift worker than in daytime worker according to ferritin level increasing. These results suggest that serum ferritin and shift work together have an effect on the development of hypertension. Further studies are needed to evaluate the underlying mechanism.
This study has some important strengths. First, this study was conducted using a representative sample of the general South Korean population. In addition, complex sample analyses for weighting instead of simple statistical analyses, and strict quality controls have been applied to the study procedures in KNHANES. Second, to our best knowledge, this is the first study investigating the association of serum ferritin levels and prevalence of hypertension according to the working type.
There are some limitations in this study. First, our study population was composed of only men. The level of serum ferritin can change dramatically before and after menopause. Ferritin levels are generally low in women of childbearing age due to iron lost during menstruation, and then the levels increase after menopause. In addition, serum ferritin concentrations in women are difficult to study because they are affected by many variables such as pregnancy, hormone therapy, and gynecological diseases. Therefore, it is unclear whether our results can be extrapolated to women. Second, our study was conducted cross-sectionally, so it was insufficient to clarify the causative relationship between serum ferritin levels and working type on the development of hypertension. Third, our study is an epidemiological study that used existing data from the National Health and Nutrition Survey and therefore we could not assess all known variables related to our research topic. For example, considering the health effects of shift work, the working duration could be an important variable [19, 20, 33, 34], but the working duration was not applicable because it was not assessed in the survey items.
Conclusions
In conclusion, this study showed that the prevalence of hypertension in male increased according to incremental increases in ferritin levels, especially in shift workers. In addition, serum ferritin levels can also be used as a subsidiary indicator to evaluate hypertension on high variant blood pressure checks.
The datasets analyzed during the current study are available in the [Korean National Health and Nutrition Examination Survey] repository, [https://knhanes.cdc.go.kr/knhanes/sub03/sub03_02_02.do].
Abbreviations
ALT
Alanine aminotransferase
AST
Aspartate aminotransferase
BMI
Body mass index
CI
Confidence interval
DBP
Diastolic blood pressure
FBS
Fasting blood sugar
Hb
Hemoglobin
KNHANES
Korean National Health and Nutrition Examination Survey
OR
Odds ratio
SBP
Systolic blood pressure
TC
Total cholesterol
TIBC
Total iron binding capacity
VitD
Vitamin D
WBC
White blood cell
WC
Waist circumference
- 1. Naito Y, Hirotani S, Sawada H, Akahori H, Tsujino T, Masuyama T. Dietary iron restriction prevents hypertensive cardiovascular remodeling in dahl salt-sensitive rats. Hypertension 2011;57:497–504. 10.1161/HYPERTENSIONAHA.110.159681. 21263124.ArticlePubMed
- 2. Dominguez-Rodriguez A, Tome MC-P, Hernandez-Garcia C, Arroyo-Ucar E, Juarez-Prera R, Blanco-Palacios G, et al. Serum ferritin and acute coronary syndrome: a strong prognostic factor? Int J Cardiol 2011;152:129–130. 10.1016/j.ijcard.2011.07.052. 21856027.ArticlePubMed
- 3. Whittington C, Kowdley K. Haemochromatosis. Aliment Pharmacol Ther 2002;16:1963–1975. 10.1046/j.1365-2036.2002.01371.x. 12452931.ArticlePubMedPDF
- 4. Gabay C, Kushner I. Acute-phase proteins and other systemic responses to inflammation. N Engl J Med 1999;340:448–454. 10.1056/NEJM199902113400607. 9971870.ArticlePubMed
- 5. Kalantar-Zadeh K, Don BR, Rodriguez RA, Humphreys MH. Serum ferritin is a marker of morbidity and mortality in hemodialysis patients. Am J Kidney Dis 2001;37:564–572. 10.1053/ajkd.2001.22433. 11228181.ArticlePubMed
- 6. Kalender B, Mutlu B, Ersöz M, Kalkan A, Yilmaz A. The effects of acute phase proteins on serum albumin, transferrin and haemoglobin in haemodialysis patients. Int J Clin Pract 2002;56:505–508. 12296612.ArticlePubMed
- 7. Jiang R, Manson JE, Meigs JB, Ma J, Rifai N, Hu FB. Body iron stores in relation to risk of type 2 diabetes in apparently healthy women. JAMA 2004;291:711–717. 10.1001/jama.291.6.711. 14871914.ArticlePubMed
- 8. Park SK, Choi WJ, Oh CM, Kim MG, Ham WT, Choi JM, et al. Clinical significance of serum ferritin level as an independent predictor of insulin resistance in Korean men. Diabetes Res Clin Pract 2015;107:187–193. 10.1016/j.diabres.2014.08.022. 25438938.ArticlePubMed
- 9. Lee BK, Kim Y, Kim YI. Association of serum ferritin with metabolic syndrome and diabetes mellitus in the south Korean general population according to the Korean National Health and nutrition examination survey 2008. Metabolism 2011;60:1416–1424. 10.1016/j.metabol.2011.02.008. 21489582.ArticlePubMed
- 10. Kang HT, Linton JA, Shim JY. Serum ferritin level is associated with the prevalence of metabolic syndrome in Korean adults: the 2007–2008 Korean National Health and nutrition examination survey. Clin Chim Acta 2012;413:636–641. 10.1016/j.cca.2011.12.011. 22212623.ArticlePubMed
- 11. Yoo KD, Ko SH, Park JE, Ahn YB, Yim HW, Lee WC, et al. High serum ferritin levels are associated with metabolic risk factors in non-obese Korean young adults: Korean National Health and nutrition examination survey (KNHANES) IV. Clin Endocrinol 2012;77:233–240. 10.1111/j.1365-2265.2011.04248.x.Article
- 12. Williams MJ, Poulton R, Williams S. Relationship of serum ferritin with cardiovascular risk factors and inflammation in young men and women. Atherosclerosis 2002;165:179–184. 10.1016/S0021-9150(02)00233-2. 12208485.ArticlePubMed
- 13. Gillum R. Association of serum ferritin and indices of body fat distribution and obesity in Mexican American men—the third National Health and nutrition examination survey. Int J Obes 2001;25:639. 10.1038/sj.ijo.0801561.ArticlePDF
- 14. Lecube A, Hernandez C, Pelegri D, Simo R. Factors accounting for high ferritin levels in obesity. Int J Obes 2008;32:1665–1669. 10.1038/ijo.2008.154.ArticlePDF
- 15. Choi B, Yeum KJ, Park SJ, Kim KN, Joo NS. Elevated serum ferritin and mercury concentrations are associated with hypertension; analysis of the fourth and fifth Korea national health and nutrition examination survey (KNHANES IV-2, 3, 2008–2009 and V-1, 2010). Environ Toxicol 2015;30:101–108. 10.1002/tox.21899. 23929718.ArticlePubMedPDF
- 16. Kim MK, Baek KH, Song K-H, Kang MI, Choi JH, Bae JC, et al. Increased serum ferritin predicts the development of hypertension among middle-aged men. Am J Hypertens 2012;25:492–497. 10.1038/ajh.2011.241. 22278211.ArticlePubMed
- 17. Piperno A, Trombini P, Gelosa M, Mauri V, Pecci V, Vergani A, et al. Increased serum ferritin is common in men with essential hypertension. J Hypertens 2002;20:1513–1518. 10.1097/00004872-200208000-00013. 12172312.ArticlePubMed
- 18. Ryoo JH, Kim SY, Oh CM, Park SK, Kim E, Park SJ, et al. The incidental relationship between serum ferritin levels and hypertension. Int J Cardiol 2015;183:258–262. 10.1016/j.ijcard.2014.10.152. 25704911.ArticlePubMed
- 19. Ha MN, Kim JY, Park JS, Chung HK. Influence of shiftwork duration on blood pressure and heart rate variability in short rotating 8-hour shiftworkers. Korean J Occup Environ Med 2001;13:180–189.ArticlePDF
- 20. Suwazono Y, Nogawa K. Effect of shift work on blood pressure. Nihon rinsho Jap J Clin Med 2014;72:1497–1502.
- 21. Suwazono Y, Dochi M, Sakata K, Okubo Y, Oishi M, Tanaka K, et al. Shift work is a risk factor for increased blood pressure in Japanese men: a 14-year historical cohort study. Hypertension 2008;52:581–586. 10.1161/HYPERTENSIONAHA.108.114553. 18625889.ArticlePubMed
- 22.
- 23. Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med 2005;352:1685–1695. 10.1056/NEJMra043430. 15843671.ArticlePubMed
- 24. Haupt CM, Alte D, Dörr M, Robinson DM, Felix SB, John U, et al. The relation of exposure to shift work with atherosclerosis and myocardial infarction in a general population. Atherosclerosis 2008;201:205–211. 10.1016/j.atherosclerosis.2007.12.059. 18321520.ArticlePubMed
- 25. Puttonen S, Kivimäki M, Elovainio M, Pulkki-Råback L, Hintsanen M, Vahtera J, et al. Shift work in young adults and carotid artery intima–media thickness: the cardiovascular risk in young Finns study. Atherosclerosis 2009;205:608–613. 10.1016/j.atherosclerosis.2009.01.016. 19215924.ArticlePubMed
- 26. https://knhanes.cdc.go.kr/knhanes/sub03/sub03_02_02.do.
- 27. Sun L, Franco OH, Hu FB, Cai L, Yu Z, Li H, et al. Ferritin concentrations, metabolic syndrome, and type 2 diabetes in middle-aged and elderly chinese. J Clin Endocrinol Metab 2008;93:4690–4696. 10.1210/jc.2008-1159. 18796516.ArticlePubMed
- 28. Fearon IM, Faux SP. Oxidative stress and cardiovascular disease: novel tools give (free) radical insight. J Mol Cell Cardiol 2009;47:372–381. 10.1016/j.yjmcc.2009.05.013. 19481547.ArticlePubMed
- 29. Wang H, Li H, Hou Z, Pan L, Shen X, Li G. Role of oxidative stress in elevated blood pressure induced by high free fatty acids. Hypertens Res 2009;32:152–158. 10.1038/hr.2008.35. 19262475.ArticlePubMedPDF
- 30. Costa G. The problem: shiftwork. Chronobiol Int 1997;14:89–98. 10.3109/07420529709001147. 9095370.ArticlePubMed
- 31. Åkerstedt T. Shift work and disturbed sleep/wakefulness. Occup Med 2003;53:89–94. 10.1093/occmed/kqg046.Article
- 32. Knutsson A. Health disorders of shift workers. Occup Med 2003;53:103–108. 10.1093/occmed/kqg048.Article
- 33. Roh SC. Shiftwork duration and metabolic risk factors of cardiovascular disease. Korean J Occup Environ Med. 2003;15:132–139.ArticlePDF
- 34. Yeom JH, Sim CS, Lee J, Yun SH, Park SJ, Yoo CI, et al. Effect of shift work on hypertension: cross sectional study. Ann Occup Environ Med 2017;29:11. 10.1186/s40557-017-0166-z. 28400961.ArticlePubMedPMCPDF
REFERENCES
Notes
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Ferroptosis in cardiovascular diseases: molecular mechanisms and a novel therapeutic target
Suli Yu, Zhen Pang, Hong Fang, Chi Liu
Molecular Biomedicine.2026;[Epub] CrossRef - Sestrin2 inhibits ferroptosis to alleviate hypertension via AMPK/Nrf2/GPX4 axis activation
Yuan Li, Ju Yan, Fengchao Wu, Yongyong Zhao, Jie Qi, Zhenyu Wang, Yaozhang Guo, Haoyu Wu
European Journal of Medical Research.2026;[Epub] CrossRef - Molecular mechanisms of iron metabolism and ferroptosis in cardiovascular diseases and intervention strategies targeting natural products (Review)
Liangqing Ge, Tianqing Zhang, Jiangbiao Yu, Sijie Xiao, Yu Zhou, Li Luo
Molecular Medicine Reports.2026; 34(2): 1. CrossRef - Baseline characteristics and associated factors for hypertension in children with chronic kidney disease: results from the Korean Cohort Study for Outcome in Patients with Pediatric Chronic Kidney Disease study
Ji Yeon Song, Keum Hwa Lee, Jae Il Shin, Hee Gyung Kang, Yo Han Ahn, Hee Sun Baek, Min Hyun Cho, Jiwon Jung, Joo Hoon Lee, Heeyeon Cho, Kyoung Hee Han, Eujin Park, Eun Mi Yang, Seong Heon Kim
Kidney Research and Clinical Practice.2026; 45(4): 634. CrossRef - Biochemical Profiles in Hypertension: Ferritin, Antioxidant Enzymes, and Mineral Levels in Blood Serum
Mohamed Salem, James Robenson
Cureus.2025;[Epub] CrossRef - Higher serum ferritins are associated with higher blood pressure: A cross-sectional study
Shaoli Li, Feilong Chen, Tao Li, Yijing Cheng, Guimin Huang, Dongqing Hou, Wenqian Liu, Tao Xu, Junting Liu
Medicine.2024; 103(12): e37485. CrossRef - Associations Between Genetically Predicted Iron Status and Cardiovascular Disease Risk: A Mendelian Randomization Study
Alexa Barad, Andrew G. Clark, Eva K. Pressman, Kimberly O. O'Brien
Journal of the American Heart Association.2024;[Epub] CrossRef - Is iron status associated with markers of non-communicable disease in adolescent Indian children?
S. Ghosh, T. Thomas, A. Kurpad, H. S. Sachdev
European Journal of Clinical Nutrition.2023; 77(2): 173. CrossRef - A proposed method for defining the required fortification level of micronutrients in foods: An example using iron
Santu Ghosh, Tinku Thomas, Raghu Pullakhandam, Krishnapillai Madhavan Nair, Harshpal S. Sachdev, Anura V. Kurpad
European Journal of Clinical Nutrition.2023; 77(4): 436. CrossRef - The associations between hematological parameters and the incidence of prehypertension and hypertension in children and adolescents: a prospective cohort study
Lan Huang, Cui Song, Qin Liu, Xiaoyue Liang, Yanling Ren, Daochao Huang, Xianmin Guan, Xizhou An, Xiaohua Liang
Hypertension Research.2023; 46(9): 2085. CrossRef - Dietary intakes of total, nonheme, and heme iron and hypertension risk: a longitudinal study from the China Health and Nutrition Survey
Shangling Wu, Peiyan Chen, Jingjing He, Zhaoyan Liu, Yi Sui, Keji Li, Aiping Fang
European Journal of Nutrition.2023; 62(8): 3251. CrossRef - Association between soluble transferrin receptor and systolic hypertension in adults: National Health and Nutrition Examination Survey (2007–2010 and 2015–2018)
Haoran Wang, Qianjin Qi, Shuaihua Song, Di Zhang, Li Feng
Frontiers in Cardiovascular Medicine.2022;[Epub] CrossRef - The association between serum ferritin and blood pressure in adult women: a large cross-sectional study
Andong He, Xiaofeng Yang, Yuzhen Ding, Lu Sun, Meiting Shi, Ruiman Li
Clinical and Experimental Hypertension.2022; 44(6): 523. CrossRef - Influence of serum ferritin combined with blood cadmium concentrations on blood pressure and hypertension: From the Korean National Health and Nutrition Examination Survey
Jeoung A. Kwon, Eunjung Park, Seyoung Kim, Byungmi Kim
Chemosphere.2022; 288: 132469. CrossRef - Role of Iron‐Related Oxidative Stress and Mitochondrial Dysfunction in Cardiovascular Diseases
Fang Yan, Kaifeng Li, Wenjuan Xing, Mingqing Dong, Mingliang Yi, Haifeng Zhang, Tao Li
Oxidative Medicine and Cellular Longevity.2022;[Epub] CrossRef - Appraising the Causal Association between Systemic Iron Status and Heart Failure Risk: A Mendelian Randomisation Study
Xingchen Wang, Xizhi Wang, Yingchao Gong, Xiaoou Chen, Danfeng Zhong, Jun Zhu, Lenan Zhuang, Jing Gao, Guosheng Fu, Xue Lu, Dongwu Lai
Nutrients.2022; 14(16): 3258. CrossRef - Maternal Iron Status in Early Pregnancy and Blood Pressure Throughout Pregnancy, Placental Hemodynamics, and the Risk of Gestational Hypertensive Disorders
Minerva J Taeubert, Clarissa J Wiertsema, Marijn J Vermeulen, Hugo G Quezada-Pinedo, Irwin K Reiss, Martina U Muckenthaler, Romy Gaillard
The Journal of Nutrition.2022; 152(2): 525. CrossRef - Correlation of Serum Ferritin and Adenosine Deaminase with Body Mass Index in Children: A cross-sectional study
Suchanda Sahu, Medha Menon, Joseph John
Indian Journal of Physiology and Pharmacology.2021; 65: 109. CrossRef - Telomere Length and Oxidative Stress and Its Relation with Metabolic Syndrome Components in the Aging
Graciela Gavia-García, Juana Rosado-Pérez, Taide Laurita Arista-Ugalde, Itzen Aguiñiga-Sánchez, Edelmiro Santiago-Osorio, Víctor Manuel Mendoza-Núñez
Biology.2021; 10(4): 253. CrossRef - Osmotic fragility in essential hypertension revisited: A correlation with Iron status and lipid profile
Z H Alhillawi, S R M Al-Ani, H K Al-Hakeim
Journal of Physics: Conference Series.2021; 1853(1): 012032. CrossRef - Iron in Cardiovascular Disease: Challenges and Potentials
Shizhen Li, Xiangyu Zhang
Frontiers in Cardiovascular Medicine.2021;[Epub] CrossRef - Evaluation of serum ferritin levels in patients of hypertension
Divmehar Kaur, Harvinder Singh, Maninder Kaur, G K Bedi, R P S Sibia
International Journal of Clinical Biochemistry and Research.2020; 7(3): 317. CrossRef - WITHDRAWN: Can Traditional Chinese Medicine provide insights into controlling the COVID-19 pandemic: Serpentinization-induced lithospheric long-wavelength magnetic anomalies in Proterozoic bedrocks in a weakened geomagnetic field mediate the aberrant tran
Moses Turkle Bility, Yash Agarwal, Sara Ho, Isabella Castronova, Cole Beatty, Shivkumar Biradar, Vanshika Narala, Nivitha Periyapatna, Yue Chen, Jean Nachega
Science of The Total Environment.2020; : 142830. CrossRef - Measuring plasma ferritin levels with two different methods: A comparison of roche cobas E601 versus roche cobas C501 (integrated modular system roche cobas 6000)
Durmuş Ayan, Sibel Soylemez
Journal of Medical Biochemistry.2019;[Epub] CrossRef - Markers of iron status, blood pressure and incident hypertension among Chinese adults
Yongjian Zhu, Gaiyun Chen, Yacong Bo, Yanhua Liu
Nutrition, Metabolism and Cardiovascular Diseases.2019; 29(8): 830. CrossRef - The Moderating Effect of Shift Work on Lipid Pathway: An Application of Multi-Group Path Analysis Model
Shokofeh Maleki, Mohammad Gholami Fesharaki, Mohsen Rowzati
Iranian Red Crescent Medical Journal.2018;[Epub] CrossRef
 Cite
Cite- Figure
-
- Related articles
-
- Association between workplace cooperation and depressive symptoms differs according to employment type: the seventh Korean Working Conditions Survey
- Association between heavy metal exposure and high-sensitivity C-reactive protein in the elderly: Korea National Health and Nutrition Examination Survey (KNHANES) 2016–2017
- Relationship between long-term PM2.5 exposure and myopia prevalence in adults: analysis of the Korea National Health and Nutrition Examination Survey–Air Pollution Linked Data, 2020
- Association between single-person household wage workers in South Korea and insomnia symptoms: the 6th Korean Working Conditions Survey (KWCS)
Association between serum ferritin and hypertension according to the working type in Korean men: the fifth Korean National Health and nutrition examination survey 2010–2012
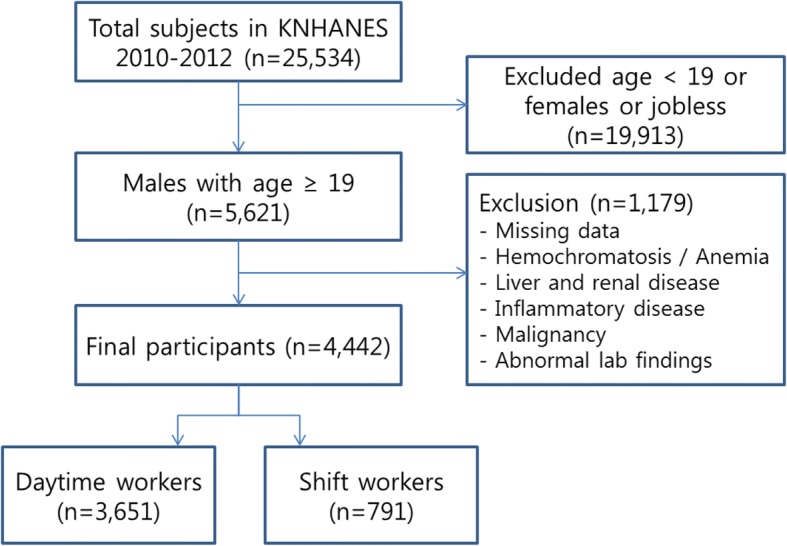
Fig. 1 A flow of the study design
Fig. 1
Association between serum ferritin and hypertension according to the working type in Korean men: the fifth Korean National Health and nutrition examination survey 2010–2012
| Variables | Quartiles of serum ferritin (ng/mL) | ||||
| Quartile 1 (≤ 66.82) | Quartile 2 (66.83–100.78) | Quartile 3 (100.79–149.13) | Quartile 4 (> 149.13) | P for trend | |
| N | 1111 | 1110 | 1111 | 1110 | |
| Age (year) | 43.87 (0.512) | 42.10 (0.486) | 42.34 (0.459) | 42.31 (0.443) | 0.025 |
| SBP (mm Hg) | 119.58 (0.503) | 119.15 (0.553) | 119.26 (0.545) | 120.95 (0.522) | 0.083 |
| DBP (mm Hg) | 78.96 (0.411) | 79.41 (0.422) | 79.65 (0.392) | 81.58 (0.400) | < 0.001 |
| WC (cm) | 82.29 (0.311) | 83.97 (0.376) | 84.11 (0.338) | 86.05 (0.377) | < 0.001 |
| BMI (kg/m2) | 23.56 (0.106) | 24.14 (0.132) | 24.20 (0.116) | 24.82 (0.141) | < 0.001 |
| FBS (mg/dL) | 95.48 (0.613) | 96.63 (0.673) | 98.33 (0.893) | 101.28 (0.878) | < 0.001 |
| TC (mg/dL) | 184.81 (1.204) | 188.77 (1.180) | 191.67 (1.301) | 193.25 (1.396) | < 0.001 |
| Triglyceride (mg/dL) | 130.68 (3.151) | 143.87 (3.559) | 155.31 (4.443) | 182.03 (6.145) | < 0.001 |
| AST (IU/L) | 21.08 (0.245) | 21.89 (0.228) | 23.00 (0.292) | 24.38 (0.305) | < 0.001 |
| ALT (IU/L) | 20.72 (0.371) | 23.47 (0.433) | 24.78 (0.441) | 28.70 (0.548) | < 0.001 |
| Hb (g/dL) | 15.23 (0.039) | 15.45 (0.036) | 15.49 (0.033) | 15.60 (0.041) | < 0.001 |
| TIBC (μg/dL) | 320.41 (1.401) | 309.24 (1.316) | 306.42 (1.266) | 302.56 (1.539) | < 0.001 |
| Cr (mg/dL) | 0.95 (0.004) | 0.96 (0.005) | 0.96 (0.004) | 0.96 (0.004) | 0.011 |
| WBC (103/uL) | 6.20 (0.050) | 6.29 (0.054) | 6.31 (0.050) | 6.43 (0.051) | 0.001 |
| VitD (ng/mL) | 18.36 (0.249) | 18.35 (0.243) | 18.45 (0.243) | 18.13 (0.234) | 0.540 |
| Variables | Quartiles of serum ferritin (ng/mL) | ||||
| Quartile 1 (≤ 66.82) | Quartile 2 (66.83–100.78) | Quartile 3 (100.79–149.13) | Quartile 4 (> 149.13) | p-value | |
| Smoking status (%) | |||||
| Quit smoker or non-smoker | 681 (58.7) | 635 (52.5) | 586 (46.9) | 605 (50.7) | < 0.001 |
| Current smoker | 430 (41.3) | 473 (47.5) | 524 (53.1) | 504 (49.3) | |
| Alcohol intake (%) | |||||
| Less than once a month | 445 (37.1) | 339 (29.5) | 307 (28.3) | 258 (20.6) | < 0.001 |
| More than twice a month | 664 (62.9) | 764 (70.5) | 797 (71.7) | 845 (79.4) | |
| Hypertension (%) | |||||
| Hypertension (−) | 770 (74.8) | 760 (73.7) | 779 (73.0) | 723 (68.5) | 0.029 |
| Hypertension (+) | 341 (25.2) | 350 (26.3) | 332 (27.0) | 387 (31.5) | |
| Variables | Odds ratio (95% confidence intervals)a | |
|---|---|---|
| Quartile 1 (≤ 66.82) | Quartile 4 (> 149.13) | |
| Daytime workers | 1.000 (ref.) | 1.426 (1.066–1.906) |
| Shift workers | 1.035 (0.680–1.576) | 1.696 (1.083–2.658) |
| Odds ratio (95% confidence intervals) | ||||
|---|---|---|---|---|
| Variables | Daytime workers | Shift workers | ||
| Unadjusted | Adjusteda | Unadjusted | Adjusteda | |
| Quartiles of ferritin (ng/mL) | ||||
| Quartile 1 (≤ 66.82) | Ref. | Ref. | Ref. | Ref. |
| Quartile 2 (66.83–100.78) | 1.037 (0.811–1.327) | 1.125 (0.853–1.484) | 1.168 (0.690–1.976) | 1.364 (0.738–2.518) |
| Quartile 3 (100.79–149.13) | 1.127 (0.865–1.469) | 1.274 (0.959–1.691) | 0.958 (0.571–1.608) | 1.088 (0.582–2.031) |
| Quartile 4 (> 149.13) | 1.297 (1.015–1.657) | 1.372 (1.027–1.833) | 1.726 (1.015–2.935) | 2.009 (1.042–3.873) |
Table 1 General and clinical characteristics according to the quartiles of serum ferritin
Data are presented as the mean (standard deviation), or numbers (percentages)
Table 2 Odds ratios (95% CI) for the prevalence of hypertension according to the interaction of serum ferritin and working type
aLogistic regression analysis after adjusting for age, FBS, TC, TIBC, BMI, alcohol intake and smoking status
Table 3 Odds ratios (95% CI) for the prevalence of hypertension according to the quartile groups of serum ferritin levels in each daytime workers and shift workers
aAdjusted for age, FBS, TC, TIBC, BMI, alcohol intake and smoking status

