
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 38; 2026 > Article
- Case Report Severe bilateral hydrocarbon pneumonitis requiring surgical drainage following accidental aspiration of industrial cleaning solvent in a seafarer: a case report
-
Sang-Heon Cho1,*
 , Jong Gill Jeong2
, Jong Gill Jeong2 -
Annals of Occupational and Environmental Medicine 2026;38:e8.
DOI: https://doi.org/10.35371/aoem.2026.38.e8
Published online: March 11, 2026
1Department of Family Medicine, Yeosu Chonnam Hospital, Yeosu, Korea
2Department of Surgery, Yeosu Chonnam Hospital, Yeosu, Korea
- *Corresponding author: Sang-Heon Cho Department of Family Medicine, Yeosu Chonnam Hospital, 49 Jwasuyeong-ro, Yeosu 59718, Korea E-mail: sheon1023@gmail.com
• Received: December 15, 2025 • Revised: February 22, 2026 • Accepted: March 2, 2026
© 2026 Korean Society of Occupational & Environmental Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,995 Views
- 74 Download
Abstract
-
Background Hydrocarbon pneumonitis is typically self-limiting, and severe complications, such as lung abscesses, are rare. Here, we report the case of a seafarer who developed bilateral lung abscesses after aspirating an industrial cleaning solvent, highlighting the aggravating role of delayed medical care and improper first-aid measures in a maritime setting.
-
Case presentation A 46-year-old seafarer presented with dyspnea, 3 days after accidentally ingesting a hydrocarbon-based solvent that he mistook for water. Although he immediately spat out the fluid, he aspirated a small amount. His condition rapidly deteriorated to necrotizing pneumonia with bilateral lung abscesses, as confirmed by chest computed tomography. Despite empirical antibiotic therapy, the abscess worsened, necessitating a video-assisted thoracic surgery for drainage. The patient recovered after surgery and underwent a prolonged course of antibiotic therapy.
-
Conclusions This case underscores the potential for life-threatening complications from industrial solvent aspiration, exacerbated by delayed medical care and forceful spitting. Strict workplace safety protocols, including the prohibition of storing chemicals in food containers to avoid confusion, and awareness about not inducing vomiting after ingestion, are essential to prevent such severe occupational injuries.
BACKGROUND
Hydrocarbon pneumonitis is an acute lung injury caused by the aspiration of volatile hydrocarbon compounds.1 While often associated with accidental ingestion in children or occupational exposure in fire-eaters and fuel siphoners, it remains a significant hazard in various industrial settings where solvents are frequently used.2,3
The toxicity of hydrocarbons is primarily determined by their physical properties; low viscosity and low surface tension facilitate rapid aspiration and wide dissemination into the distal airways.4 Upon entering the alveoli, these substances disrupt surfactant function, induce intense inflammatory responses, and cause direct tissue necrosis.1,2 Although the clinical course varies, most cases of hydrocarbon pneumonitis are self-limiting and resolve with supportive care. Serious complications such as lung abscesses, pneumatoceles, or bronchopleural fistulas are relatively rare, and cases requiring surgical intervention are infrequently reported.4,5
Most reported cases of occupational hydrocarbon pneumonitis involve fuels, such as diesel, gasoline, and kerosene.3,4 There is a paucity of literature describing severe necrotizing pneumonia caused by specific industrial cleaning solvents. In this report, we describe a rare and severe case of a seafarer who developed bilateral lung abscesses requiring surgical drainage after accidental aspiration of a hydrocarbon-based electric motor cleaner that was misidentified as drinking water because it was stored in a beverage container. This case highlights the potential severity of industrial solvent aspiration and underscores the importance of chemical management in workplace safety.
CASE PRESENTATION
A previously healthy 46-year-old male Filipino seafarer presented to the emergency department with dyspnea. Three days prior to admission, while working on a ship, he accidentally ingested a hydrocarbon-based industrial cleaning solvent, Electrosolv-E (Unitor Chemicals AS, Kjopmannskjaer, Norway), mistaking it for drinking water as the liquid was clear, colorless, and odorless. He immediately spat out the substance due to its unpleasant taste but reported that a small amount entered his nasal cavity and airway during the process. Following the exposure, he developed fever, cough, lower chest pain, and dyspnea. Owing to his distance from the sea to the shore, he visited the emergency department 3 days after the onset of symptoms.
Upon admission, his vital signs were as follows: blood pressure, 100/60 mmHg; pulse rate, 120 beats/min; respiratory rate, 20 breaths/min; and body temperature, 38.2°C. Pulse oximetry revealed that oxygen saturation was 95% on room air. Chest auscultation revealed crackling rales in the lower bibasilar lobes. Initial laboratory investigations showed significant leukocytosis with white blood cell (WBC) count of 28,100 cells/µL and elevated C-reactive protein (CRP) level of 35.39 mg/dL. To evaluate for potential secondary infection, multiple microbiological cultures were performed during the early hospital course. These included blood and sputum cultures on the day of hospital admission (day 1), a follow-up sputum culture on day 2, and sputum and urine cultures on day 3. All cultures yielded no specific growth. Chest radiography revealed bilateral pleural effusions and patchy consolidations in both lower lung fields suggestive of pneumonia (Fig. 1). Contrast-enhanced computed tomography (CT) of the chest revealed ground-glass opacities in the right middle lobe, base of the right lower lobe, and left lower lobe, accompanied by intrinsic air and bronchovascular bundles. Based on these findings, the patient was admitted to the intensive care unit with a diagnosis of encapsulated necrotizing pneumonia.
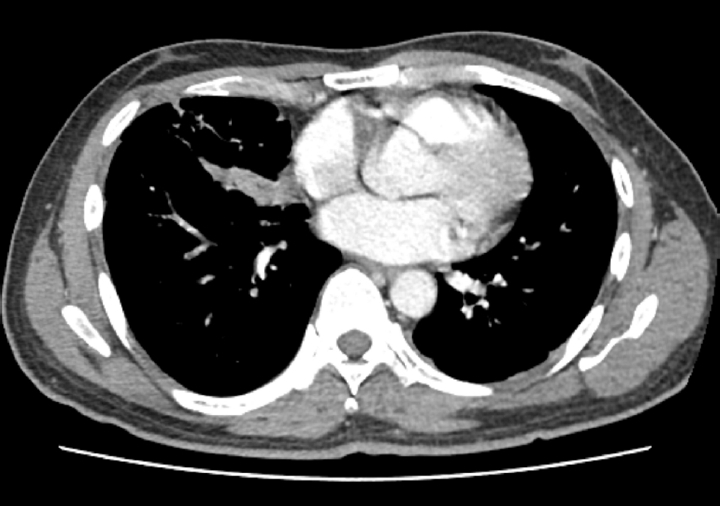
Empirical intravenous antibiotic therapy with piperacillin/tazobactam and levofloxacin was administered. On the second day of admission, the patient developed hemoptysis for which intravenous tranexamic acid was administered for 5 days, followed by oral maintenance. Clinical improvement was not achieved following a 7-day course of intravenous antibiotics, with the clinical course marked by unresolved febrile episodes and persistent leukocytosis. Furthermore, a follow-up chest CT on hospital day 7 revealed aggravation of the internal cavitations and abscess formation within the consolidative lesions of the right middle lobe and both lower lobes (Fig. 2). The failure of conservative management to arrest the necrotizing process, combined with the high risk of secondary sepsis from the poorly drained, inspissated purulent material, prompted the decision to escalate to video-assisted thoracoscopic surgery (VATS) for definitive source control and debridement. Intraoperative examination revealed dense pleural adhesions and extensive necrosis of the lung parenchyma. Thick, yellowish, and inspissated purulent material was drained from the abscess cavities located in the right middle and left lower lobes (Fig. 3). Given the deep and multiloculated nature of the abscesses, wide unroofing was performed via wedge resection using an endoscopic stapler and ultrasonic shear to ensure adequate drainage. Subsequently, thorough decortication and irrigation of the thoracic cavity were performed. A closed thoracostomy was performed with chest tube and Hemovac placement. Histopathological examination of the lung tissue revealed acute fibrinous and organizing pneumonia, consistent with chemical exposure.
After surgery, the antibiotic regimen was modified. Piperacillin/tazobactam was discontinued after 8 days of treatment and the regimen was switched to cefepime, which was maintained for 21 days. Levofloxacin was administered intravenously for 15 days, followed by oral maintenance for 14 days. The patient’s condition improved steadily. He was transferred to the general ward on hospital day 11, and the chest tubes were removed on hospital day 15. By hospital day 28, follow-up chest radiography showed significant resolution of haziness in the right middle and left lower lobes (Fig. 4). Laboratory markers normalized, with WBC count of 8,200 cells/µL and CRP level of 0.37 mg/dL. The temporal changes in these inflammation-related biomarkers throughout the hospital stay are illustrated in Fig. 5. The comprehensive clinical course, encompassing the temporal relationship between symptom onset, diagnostic imaging, and therapeutic interventions, is summarized in Fig. 6. The patient was discharged on day 29 of hospitalization without further respiratory complications.
The study was exempt from Institutional Review Board (IRB) review as it was a single case report. Accordingly, the requirement for informed consent was waived.
DISCUSSION AND CONCLUSION
The present case highlights severe manifestations of hydrocarbon pneumonitis complicated by bilateral lung abscesses following accidental aspiration of an industrial cleaning solvent. While hydrocarbon pneumonitis is well documented in pediatric accidental ingestion or specific occupational groups, such as fire-eaters,3 this case underscores the critical hazard posed by industrial solvents in maritime settings and the potential for life-threatening complications requiring surgical intervention.
The clinical course and prognosis of hydrocarbon pneumonitis are intrinsically linked to the physicochemical properties of the aspirate and extent of the initial injury. Typically, aspiration of low-viscosity hydrocarbons results in acute but self-limiting chemical pneumonitis. Systemic manifestations such as fever and leukocytosis often resolve within days with supportive care, although radiological resolution may lag by weeks or months.1,6 A well-documented sequela in such cases is the formation of pneumatoceles and thin-walled air cysts, which usually resolve spontaneously without intervention.3,6 This presentation is in distinct contrast to exogenous lipoid pneumonia induced by high-viscosity oils, which follows a chronic, indolent course often characterized by fibrosis or mass-like paraffinomas.6,7
However, this case is noteworthy due to its atypically severe progression, deviating significantly from the expected trajectories. Instead of a self-limiting course or simple pneumatocele formation, the patient developed rapid necrotizing pneumonia that progressed to severe multiloculated lung abscesses. While the clinical severity of hydrocarbon pneumonitis is primarily determined by the physicochemical properties of the aspirate—such as low viscosity and low surface tension—the occupational setting acts as a significant modifier of the clinical course. In this case, although the patient reported aspirating only a 'small amount', the inherent toxicity of the hydrocarbon-based solvent with low viscosity caused extensive tissue necrosis. Furthermore, the maritime context served as a critical aggravating factor in the development of life-threatening complications. The 3-day delay in medical access, typical of remote maritime work, provided a unique clinical window for the unchecked progression of the chemical injury. Hydrocarbon aspiration induces an immediate inflammatory response characterized by macrophage activation and the release of inflammatory cytokines, leading to chemical pneumonitis.3,4 Although the use of prophylactic antibiotics and corticosteroids remains controversial and is generally not recommended for uncomplicated cases,4,8 the lack of immediate medical monitoring allows the initial chemical injury to progress unchecked. While secondary bacterial infection was initially suspected as a contributing factor for the progression to necrotizing pneumonia, all microbiological cultures yielded negative results, and clinical deterioration occurred despite empirical antibiotic therapy. Therefore, sterile chemical necrosis may have served as a primary or concurrent pathogenic mechanism for the extensive tissue destruction. In this context, the persistent inflammatory markers and atypical radiological aggravation may reflect intense inflammatory destruction caused by the direct toxicity of the hydrocarbon itself, rather than purely infectious processes. Consequently, while conservative management remains the standard of care for uncomplicated hydrocarbon pneumonitis, this case demonstrates that surgical intervention, such as VATS, is inevitable when the disease course is complicated by extensive necrosis and localized abscesses refractory to antibiotic therapy. Surgical intervention was warranted as the extensive necrosis and inspissated purulent material were refractory to empirical antibiotic therapy. This underscores a vital lesson: while conservative management is the standard for adult hydrocarbon pneumonitis, clinicians must consider early surgical debridement when necrotic complications arise, especially when medical access has been delayed.
In addition to the delayed presentation, the profound severity of the lung injury in this case reflects a class effect of low-viscosity hydrocarbons rather than a unique toxicity specific to Electrosolv-E. According to the safety data sheet, this agent is a hydrotreated heavy naphtha (CAS number 64742-48-9) consisting of C11–C13 hydrocarbons, which share general physicochemical properties—such as low viscosity and low surface tension—common to this class of substances.9 These properties allow for rapid penetration into the distal airways and disruption of the pulmonary surfactant, leading to direct alveolar cytotoxicity.10,11 Crucially, the patient’s immediate reaction to spit out the fluid likely exacerbates the injury. Forceful spitting or vomiting atomizes the liquid, forcing the glottis to open and increasing the risk of aspiration.2 It should be clearly noted that while ingestion of hydrocarbons is not safe and can cause systemic toxicity, the risk of severe, life-threatening lung injury is primarily driven by aspiration during attempts to expel the substance.1,2,9 This highlights a critical safety lesson: workers must be informed that for low-viscosity hydrocarbons, inducing vomiting or forceful spitting significantly increases the risk of severe pulmonary toxicity.
Therefore, the exposure mechanism is critical. From an occupational health perspective, this incident stems from a fundamental failure in hazardous communication, misidentifying a colorless, odorless solvent such as water. Reliance on sensory cues such as smell or color is unreliable and dangerous, and despite the Safety Data Sheet noting a slight hydrocarbon odor,9 it was insufficient to prevent accidental ingestion in this real-world setting. Therefore, administrative controls, including standardized color-coded labeling and mandatory use of dedicated, secured chemical storage lockers, must be rigorously implemented to eliminate the root cause of such accidents. Furthermore, safety training should incorporate realistic emergency scenarios emphasizing that an instinctive reaction to spit or vomit low-viscosity hydrocarbons can be detrimental and that first-aid protocols must explicitly contraindicate induced vomiting and highlight the risk of atomization and subsequent aspiration during forceful spitting.
In conclusion, this case illustrates severe hydrocarbon pneumonitis complicated by bilateral lung abscesses necessitating surgical intervention in a seafarer, and exacerbated by delayed medical access and aspiration risk associated with spitting out the solvent. This underscores the critical need for strict chemical storage protocols and safety education, emphasizing that vomiting or spitting is contraindicated during hydrocarbon ingestion. Early recognition and aggressive management are vital for favorable outcomes in severe occupational cases.
Abbreviations
CRP
C-reactive protein
CT
computed tomography
VATS
video-assisted thoracoscopic surgery
WBC
white blood cell
-
Competing interests
The authors declare that they have no competing interests.
-
Author contributions
Conceptualization: Cho SH, Jeong JG. Data curation: Cho SH. Methodology/formal analysis/validation: Cho SH. Writing - original draft: Cho SH. Writing - review & editing: Cho SH, Jeong JG.
NOTES
Fig. 1.
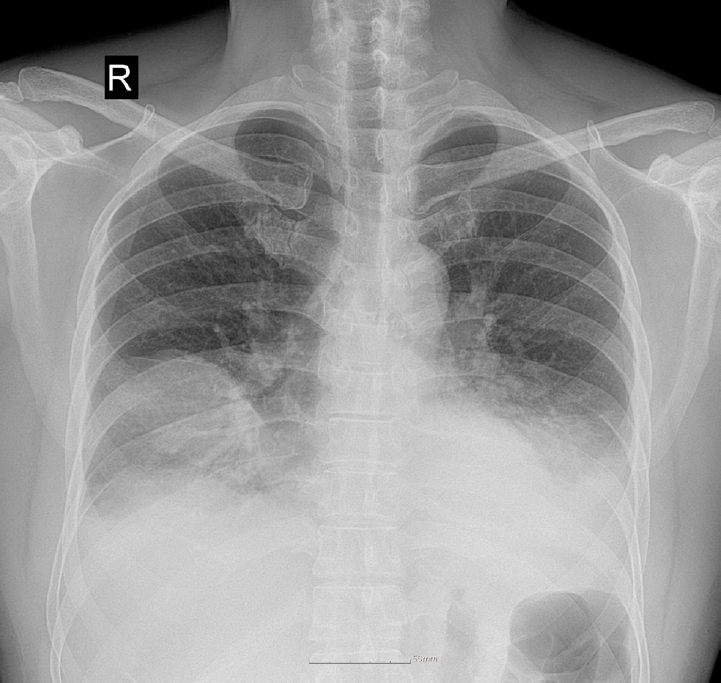
Initial chest radiograph showing bilateral patchy consolidations over lower lung fields with pleural effusion.
Fig. 2.

Chest computed tomography on day 7 revealing multiloculated abscesses involving right middle and left lower lobes.
Fig. 3.
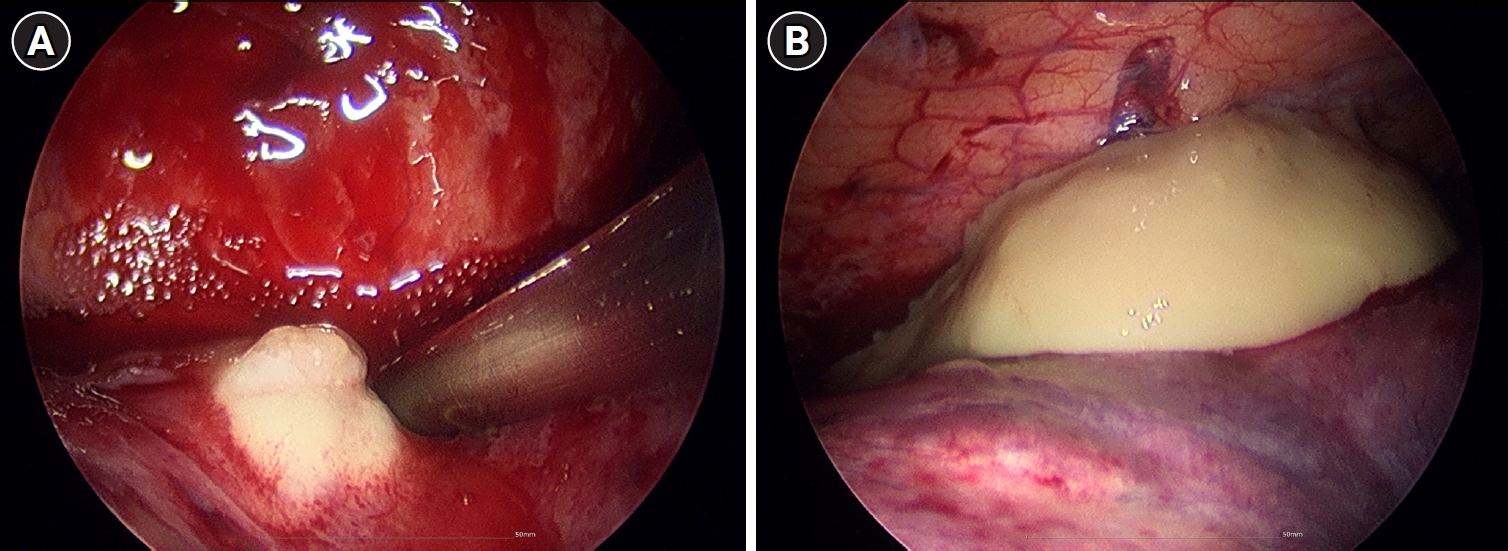
Intraoperative thoracoscopic findings of bilateral lung abscesses secondary to necrotizing pneumonia. (A) Right middle lobe. (B) Left lower lobe.
Fig. 4.
Near-complete resolution of multiloculated abscesses involving right middle and left lower lobes at follow-up computed tomography.
Fig. 5.
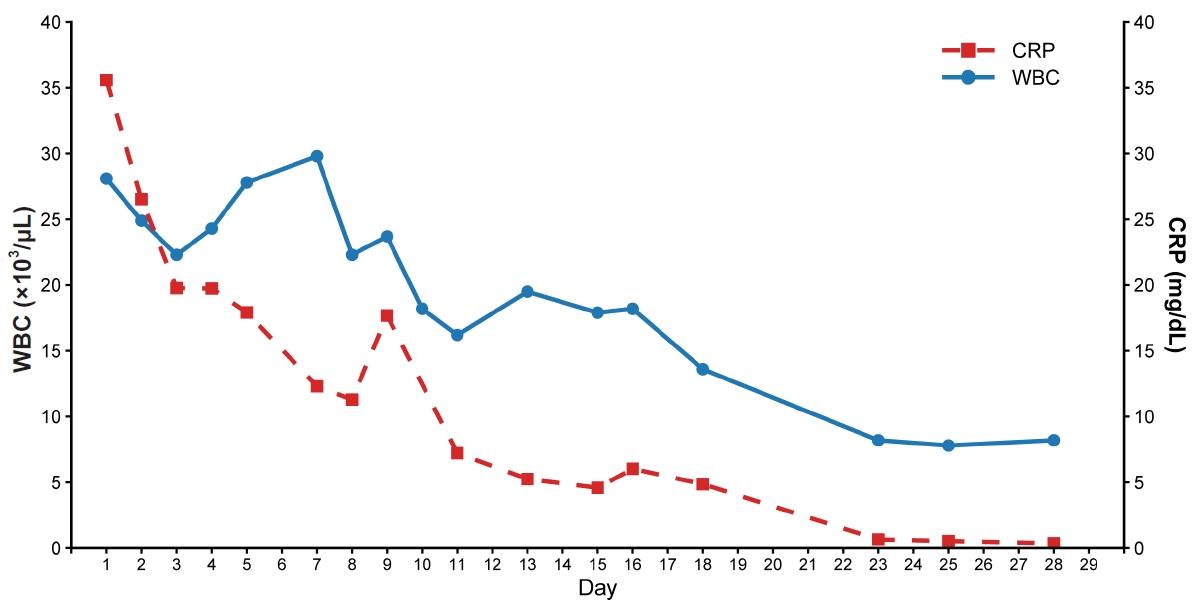
Temporal changes in white blood cell (WBC) count and C-reactive protein (CRP) level during the 29-day hospitalization.
Fig. 6.
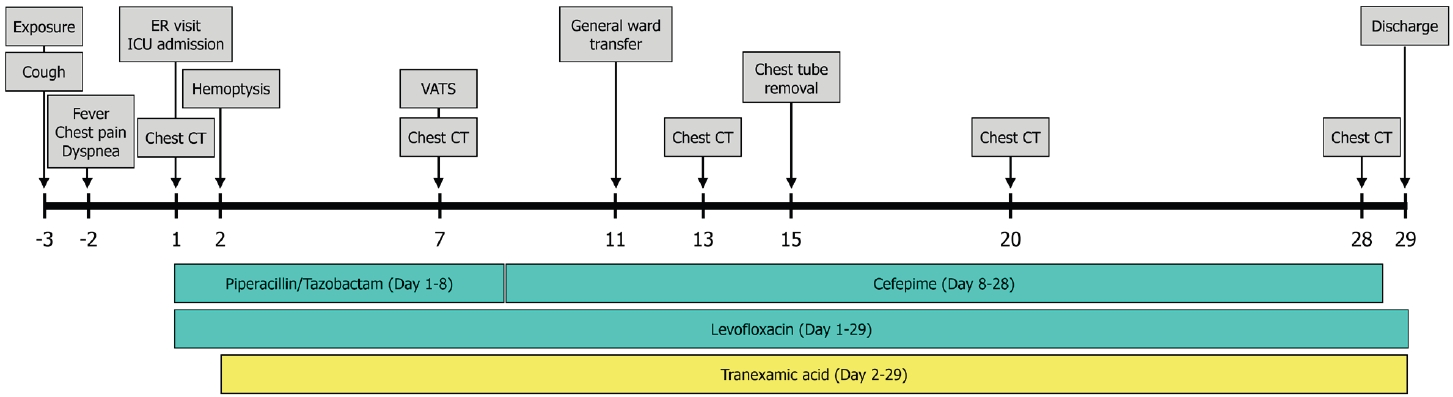
Clinical timeline illustrating the patient’s course from exposure to discharge, including key clinical events, diagnostic imaging, and therapeutic interventions. CT: computed tomography; ER: emergency room; ICU: intensive care unit; VATS: video-assisted thoracoscopic surgery.
- 1. Tormoehlen LM, Tekulve KJ, Nanagas KA. Hydrocarbon toxicity: a review. Clin Toxicol (Phila) 2014;52(5):479–89.ArticlePubMed
- 2. Kim SH, Jegal Y, Choy N, Kim Y. A case of chemical pneumonitis after ingestion of hydrocarbon. Korean J Occup Environ Med 2009;21(4):406–11.ArticlePDF
- 3. Yi MS, Kim KI, Jeong YJ, Park HK, Lee MK. CT findings in hydrocarbon pneumonitis after diesel fuel siphonage. AJR Am J Roentgenol 2009;193(4):1118–21.ArticlePubMed
- 4. Reddy R, Baek J, Perone HR, Chen K, Lichtstein DM. The hurricane lung: a case of hydrocarbon pneumonitis with abscess formation following fuel siphoning. Cureus 2021;13(5):e14807.ArticlePubMedPMC
- 5. Rajpoot A, Sharma P, Kumar A, Rathore SS. Hydrocarbon pneumonitis with abscess formation following diesel siphoning. BMJ Case Rep 2022;15(6):e249147.ArticlePubMedPMC
- 6. Hu X, Lee JS, Pianosi PT, Ryu JH. Aspiration-related pulmonary syndromes. Chest 2015;147(3):815–23.ArticlePubMed
- 7. Marchiori E, Zanetti G, Mano CM, Hochhegger B. Exogenous lipoid pneumonia: clinical and radiological manifestations. Respir Med 2011;105(5):659–66.ArticlePubMed
- 8. Shrivastava MS, Palkar AV, Karnik ND. Hydrocarbon pneumonitis masquerading as acute lung injury. BMJ Case Rep 2011;2011:bcr0320114017.PubMedPMC
- 9. Unitor Chemicals AS. Safety Data Sheet: ELECTROSOLV-E (Version 3.0.0). Kjopmannskjaer, Norway: Unitor Chemicals AS; 2003.
- 10. Pham K, Sverchek J, McPheeters RA. Chemical pneumonitis from hydrocarbon aspiration. West J Emerg Med 2008;9(3):165.PubMedPMC
- 11. Petrescu IO, Cosoveanu CS, Popa A, Stanca L, Petrescu F, Tudorascu RD, et al. Fatal evolution in the pneumonia caused by diesel fuel aspiration: case report. Curr Health Sci J 2016;42(3):293–7.PubMedPMC
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteSevere bilateral hydrocarbon pneumonitis requiring surgical drainage following accidental aspiration of industrial cleaning solvent in a seafarer: a case report
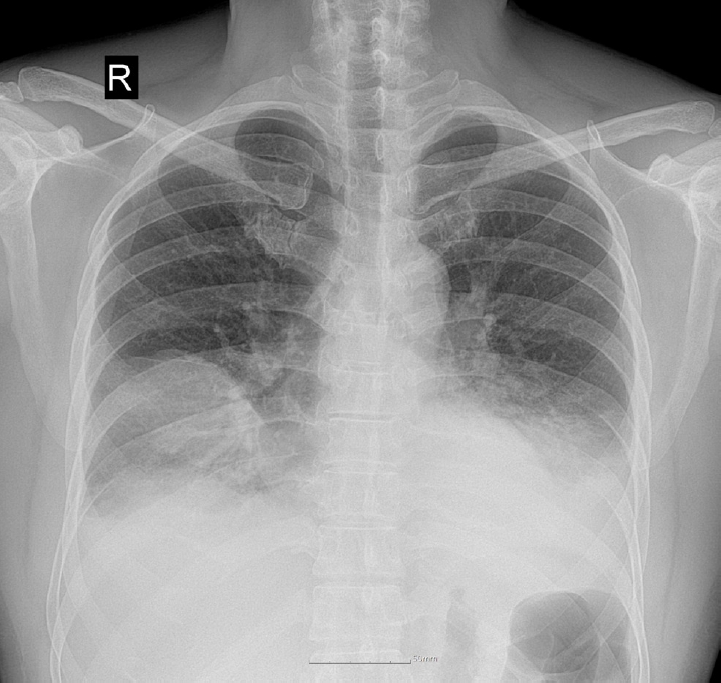

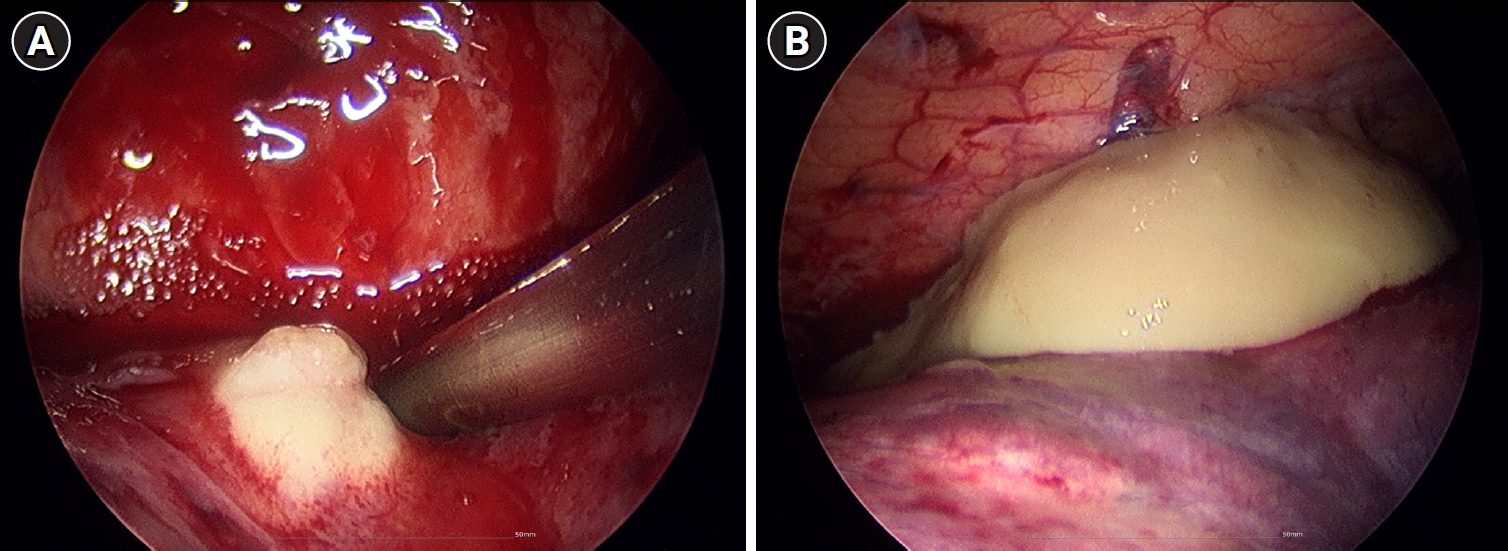
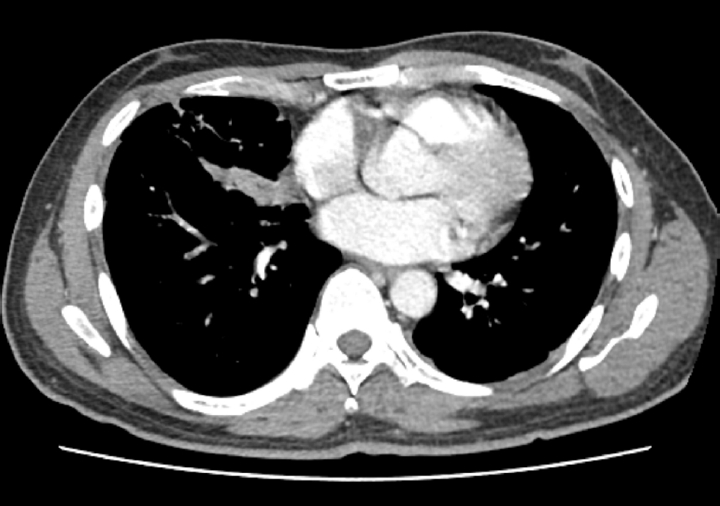
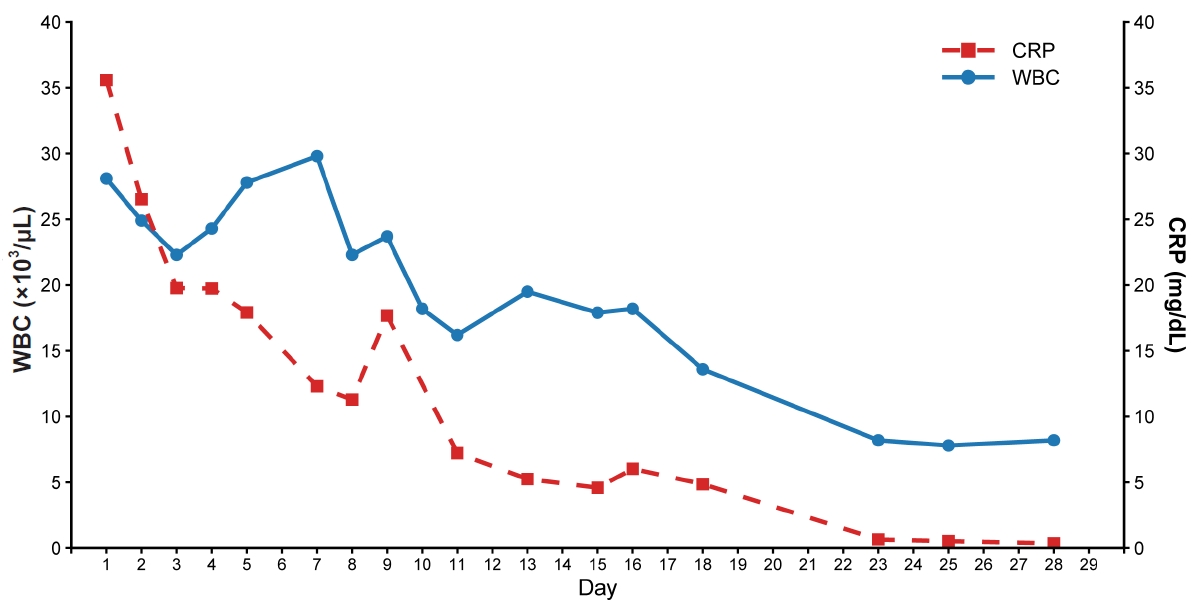
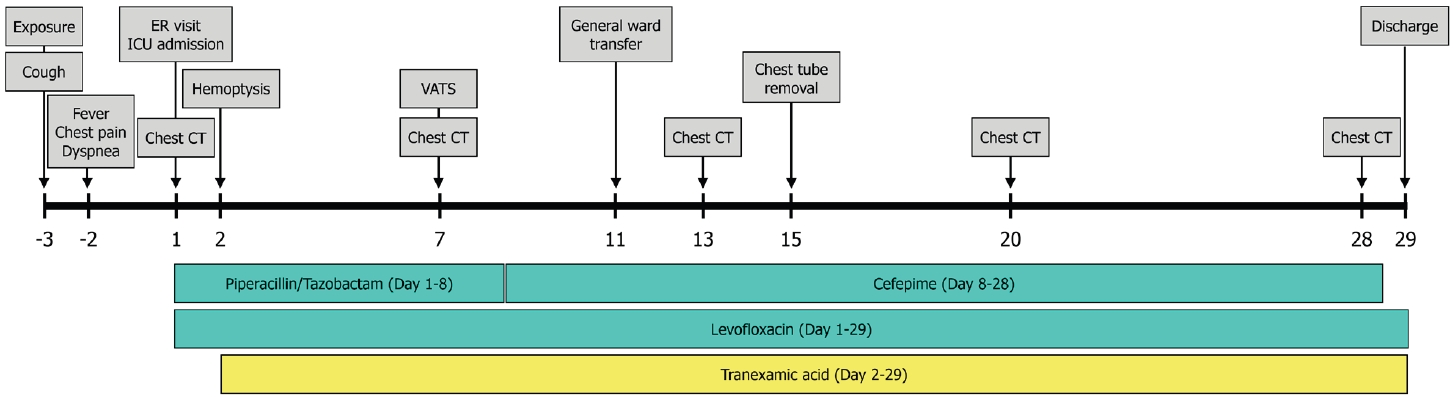
Fig. 1. Initial chest radiograph showing bilateral patchy consolidations over lower lung fields with pleural effusion.
Fig. 2. Chest computed tomography on day 7 revealing multiloculated abscesses involving right middle and left lower lobes.
Fig. 3. Intraoperative thoracoscopic findings of bilateral lung abscesses secondary to necrotizing pneumonia. (A) Right middle lobe. (B) Left lower lobe.
Fig. 4. Near-complete resolution of multiloculated abscesses involving right middle and left lower lobes at follow-up computed tomography.
Fig. 5. Temporal changes in white blood cell (WBC) count and C-reactive protein (CRP) level during the 29-day hospitalization.
Fig. 6. Clinical timeline illustrating the patient’s course from exposure to discharge, including key clinical events, diagnostic imaging, and therapeutic interventions. CT: computed tomography; ER: emergency room; ICU: intensive care unit; VATS: video-assisted thoracoscopic surgery.
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fig. 5.
Fig. 6.
Severe bilateral hydrocarbon pneumonitis requiring surgical drainage following accidental aspiration of industrial cleaning solvent in a seafarer: a case report

