
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 38; 2026 > Article
- Original Article Acute health effects of accidental exposure to lithium hydroxide at a battery material production plant
-
Chul Gab Lee1,2,*
 , Soo Hyeong Park1, Ji Won Kang2, Si Woo Hwang2, Hyeo Na Kim2, Hyeon Kyeong Ko2
, Soo Hyeong Park1, Ji Won Kang2, Si Woo Hwang2, Hyeo Na Kim2, Hyeon Kyeong Ko2 -
Annals of Occupational and Environmental Medicine 2026;38:e6.
DOI: https://doi.org/10.35371/aoem.2026.38.e6
Published online: February 9, 2026
1Department of Occupational and Environmental Medicine, Chosun University Hospital, Gwangju, Korea
2Gwangju Branch of Korea Occupational Disease Surveillance Center, Gwangju, Korea
- *Corresponding author: Chul Gab Lee Department of Occupational and Environmental Medicine, Chosun University Hospital, 365 Pilmun-daero, Dong-gu, Gwangju 61453, Korea E-mail: cglee@chosun.ac.kr, eecg@daum.net
• Received: August 13, 2025 • Revised: January 27, 2026 • Accepted: January 30, 2026
© 2026 Korean Society of Occupational & Environmental Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,857 Views
- 116 Download
- 1 Crossref
Abstract
-
Background Lithium hydroxide (LiOH) is increasingly used in electric vehicle battery production; however, its health effects in the work environment remain underreported. This study characterizes the acute health effects on workers following accidental occupational exposure to LiOH at a Korean lithium plant in March 2024.
-
Methods We analyzed health effects from two LiOH exposure accidents on March 6 and 9, 2024, involving 50–100 kg powder spills. Two datasets were examined: acute symptoms from 115 workers who visited hospitals immediately after exposure, and a symptom severity survey from 474 workers conducted 2 weeks post-exposure. Workers were stratified by distance from the leak source (<10 m, 10–20 m, >20 m) and respirator use. Univariate general linear modeling was applied to analyze the relationship between symptom occurrence and both the distance from the exposure source and respirator use.
-
Results Among workers visiting hospitals immediately, local irritation symptoms predominated: sore throat (58.3%), cough (28.7%), and skin dermatoses (17.4%). Systemic symptoms included headache (45.2%), nausea (18.3%), chest tightness (12.2%), and dizziness (9.6%). Two-week follow-up revealed overall symptom improvement; severe cough decreased from 22.2% to 10.1%. However, despite general improvement, a significant portion of workers reported persistent respiratory issues, including cough (28.7%) and sputum production (31.0%). Symptom severity showed a significant dose-response relationship with proximity to the source (p < 0.001). While respirator use offered initial protection (p = 0.021), this effect was not statistically significant after 2 weeks.
-
Conclusions Occupational LiOH exposure caused acute irritation and systemic symptoms, demonstrating immediate tissue damage consistent with its alkalinity and systemic toxicity upon absorption. As lithium battery production expands globally, these results emphasize the necessity for developing specific occupational exposure limits and medical surveillance guidelines for lithium compounds.
BACKGROUND
Lithium, a key raw material for secondary batteries, is in increasingly high demand. Its necessity has been emphasized in recent years due to the rising market for electric vehicles (EVs) and the proliferation of smart devices. The global transition toward cleaner energy and transportation has led to a significant surge in the need for high-performance rechargeable batteries,1 making lithium compounds more critical than ever. One of the key materials is lithium hydroxide (LiOH). It is essential for producing high-nickel cathode materials used in EV batteries, enabling longer life, enhanced safety, and higher power output. Compared to lithium carbonate (Li2CO3), another standard material, LiOH exhibits superior performance in the synthesis of these high-performance batteries, driving its demand as the EV market grows.2,3
Lithium has long been used in psychiatry as a treatment for bipolar disorder in the form of lithium carbonate, so its toxicity profile is well established.4 If occupationally exposed to lithium hydroxide, hydroxide ions (OH–) can cause immediate corrosive damage through liquefactive necrosis,5 and lithium ions (Li+) have the potential to cause systemic effects upon absorption. However, the specific mechanism of action in occupational settings is not yet fully elucidated.6-8 This is largely due to the paucity of literature on lithium toxicity within occupational and environmental medicine, despite the significant expansion of lithium use in various industries, including the secondary battery sector.9-13
In Korea, the construction of a lithium hydroxide plant was promoted to enhance the competitiveness of the domestic battery industry and establish a stable supply chain, thereby reducing dependence on imports. Unfortunately, a LiOH leak occurred in March 2024 during an accelerated commissioning phase at a plant with an annual production capacity of 43,000 tons. This accident provided an unprecedented opportunity to characterize the acute health effects in a large cohort of workers exposed to LiOH.
METHODS
This report documents the acute health effects of occupational exposure to LiOH resulting from two accidental releases during the commissioning of a new production facility.
The first accident occurred at approximately 8:00 a.m. on March 6, 2024, during the final commissioning stage of the primary LiOH production plant. Mechanical vibrations caused a rupture in a silicone connector within the powder supply lines, releasing approximately 50–100 kg of LiOH powder. The leak originated from a height of roughly 5 to 6 m and was dispersed by prevailing winds. The plume directly impacted workers conducting a morning Tool Box Meeting immediately beneath the construction site of the second lithium plant. Workers receiving a pre-work briefing were suddenly enveloped in LiOH dust; this exposure necessitated an immediate work stoppage as workers presented with acute mucosal irritation.
Exposure intensity varied by location; some workers experienced direct, high-intensity contact with the powder, while others reported only mild irritation. Symptoms included stinging sensations in the eyes, nose, and oropharynx—clinically resembling exposure to lacrimatory agents—accompanied by coughing and epiphora. Direct dermal contact resulted in erythematous rashes. Due to the unprecedented nature of the accident and the lack of established response protocols, union officials and supervisors directed all affected workers to a nearby emergency department. Physicians, confronted with several hundred workers presenting simultaneously with similar irritant symptoms and lacking immediate toxicological data on LiOH, provided supportive care. Patients were discharged following the resolution of their acute symptoms.
A second exposure event occurred three days later. During site preparation for a safety inspection, the use of compressed air to dislodge residual LiOH powder from structural crevices resulted in the re-aerosolization of the chemical. This secondary dust cloud affected workers who were changing into work uniforms in a temporary break room. Although the March 6 accident had concluded without severe sequelae, workers exhibiting symptoms from this second exposure were advised to undergo further medical evaluation.
Following these two accidents, approximately 700 workers sought medical attention at local facilities. However, due to the absence of a centralized epidemiological investigation and privacy restrictions, comprehensive aggregate data were unavailable. This study analyzes two distinct datasets: (1) physician-reported clinical records from 115 workers treated at a single hospital, and (2) a self-reported symptom survey completed by 474 workers 2 weeks post-accident. While a population overlap between these datasets is likely, the anonymized nature of the data precludes direct linkage. Future reports will address long-term health outcomes in the subset of patients who presented to an occupational and environmental medicine clinic with persistent symptoms.
The two datasets document clinical signs and symptoms resulting from a single lithium hydroxide exposure event. The first dataset is derived from physician assessments conducted immediately post-exposure, while the second is based on a self-reported questionnaire administered 2 weeks later.
The first dataset categorizes symptoms from 115 individuals presenting at the hospital into local irritant and systemic symptoms, calculating the incidence of each. While a subset of workers underwent imaging (e.g., chest radiography or low-dose computed tomography), diagnoses were primarily based on physician interviews and physical examinations.
The second dataset comprises follow-up survey data from 474 workers, collected 2 weeks post-accident. This survey evaluated the severity of symptoms both at the time of exposure and at the two-week follow-up. Participants rated the severity of respiratory (cough, sputum, dyspnea on exertion/rest, chest pain, nasopharyngeal irritation), dermatological (facial pruritus), ocular (pruritus, injection), and gastrointestinal (heartburn, abdominal pain) symptoms on a scale from 0 (‘not at all’) to 10 (‘very bothersome’). Additionally, distance from the leakage source was stratified into three categories (<10 m, 10–20 m, and ≥20 m), and the use of respiratory protection was recorded.
Symptom frequencies from the hospital visit data were summarized using counts and percentages for the 115 cases. For the second dataset, we calculated the proportion of participants reporting a change in symptom severity (measured on a scale of 0–10) between the initial exposure and the 2-week follow-up. Additionally, the severity ratings of the 10 symptoms were summed to derive composite symptom scores for both the time of exposure and 2 weeks post-accident. These symptom scores served as dependent variables. Distance from the exposure source and respirator usage were included as fixed factors. A univariate General Linear Model was employed to examine the associations between these factors and symptom severity. All statistical analyses were performed using SPSS version 29.0 (IBM Corp., Armonk, NY, USA).
This study was conducted by the ethical principles of the Declaration of Helsinki. The present study protocol was reviewed and approved by the Institutional Review Board of CHOSUN IRB (approval No. 2025-08-004). Informed consent was submitted by all subjects when they were enrolled.
RESULTS
The clinical manifestations observed in workers seeking medical attention following lithium hydroxide exposure were categorized into two distinct profiles: immediate corrosive local irritation and systemic toxicity (Table 1). Among the symptoms indicative of local irritation, sore throat was the most predominant, affecting 58.3% (n = 67) of the patients, indicating significant upper airway mucosal injury. This was followed by cough (28.7%, n = 33) and dermatological complications (17.4%, n = 20). Regarding ocular and nasal irritation, reports of bilateral ocular tingling or pain (11.3%, n = 13) and nasal congestion or rhinorrhea (11.3%, n = 13) were documented. Sputum production was noted in 9.6% (n = 11) of cases, a relatively low acute prevalence that contrasts with later findings.
Systemic symptomatology was led by headache, which was reported by 45.2% (n = 52) of the workers, likely reflecting a combination of chemical toxicity and acute physiological stress. Other systemic effects included nausea (18.3%, n = 21), chest tightness (12.2%, n = 14), dizziness (9.6%, n = 11), generalized fatigue (8.7%, n = 10), diarrhea (5.2%, n = 6), and sleep disturbances (2.6%, n = 3).
Data from the symptom survey conducted 2 weeks post-accident on 474 workers (Table 2) indicated a general attenuation in overall symptom severity; however, the prevalence of respiratory symptoms, specifically cough and sputum production, remained notably elevated. The severity profile for cough demonstrated a significant shift: the proportion of workers reporting severe symptoms (7–10 points) declined from an initial 22.2% to 10.1% by the second week, while reports of mild symptoms (1–3 points) increased markedly from 18.8% to 31.0%. The prevalence of moderate symptoms remained relatively stable (21.3% initially vs. 23.8% at follow-up).
While the severity of respiratory symptoms such as cough, sputum production, and sore throat generally trended toward improvement (Table 2, Fig. 1), the absolute prevalence of complaints regarding local irritation—specifically affecting the eyes, nose, and skin—was markedly higher in the retrospective survey (Table 2) compared to the initial hospital intake data (Table 1). Specifically, initial ocular pain was reported by 54.9% in the survey versus 11.3% in hospital records. This discrepancy suggests that a significant portion of workers experienced local irritation immediately following exposure but did not seek medical evaluation, likely perceiving these ocular, nasal, or cutaneous symptoms as insufficiently severe to warrant emergency care.
Systemic symptom severity also exhibited an overall decline over the 2-week period. The prevalence of severe dyspnea on exertion decreased from an initial 12.4% to 5.9% at follow-up, and severe dyspnea at rest declined from 8.9% to 3.6% (Table 2). Despite the general trend toward recovery, distinct subsets of the cohort reported a worsening of symptoms, including sputum production (31.0%), cough (28.7%), and sore throat (25.9%) (Fig. 1), indicating a persistence or evolution of respiratory inflammation in these individuals.
Fig. 2 illustrates the correlation between symptom severity, distance from the leak source, and respirator usage. A statistically significant inverse relationship was observed between the total symptom score at the time of the accident and the distance from the source; scores were highest in the group closest to the leak (<10 m) and decreased as distance increased (p < 0.001). Furthermore, symptom scores were significantly elevated in workers who did not wear respirators (p = 0.021), with a significant interaction between distance and respirator use (p = 0.012). At the 2-week follow-up, the distance-dependent gradient in symptom scores persisted (p < 0.001), with a marked reduction in scores for those exposed at distances of 10 m or greater. However, the protective effect associated with respirator use was no longer significant at the 2-week mark (p = 0.071), suggesting that while respirators mitigated the acute symptom burden, their impact on the persistence of subacute symptoms was less pronounced or confounded by other exposure variables.
DISCUSSION
Literature offering direct comparisons to occupational LiOH exposure is sparse.14 To our knowledge, this is the first case report documenting acute occupational lithium hydroxide exposure in humans resulting from an accidental release. While a 1981 National Institute for Occupational Safety and Health (NIOSH) health hazard assessment at a lithium processing facility noted that workers frequently experienced upper respiratory irritation and skin rashes upon exposure to lithium compounds, that study lacked detailed exposure data.9 Animal studies have demonstrated that inhalation of lithium dust or fumes can induce pulmonary tissue damage, potentially leading to pneumonia in rats.10 Lithium hydroxide is a highly alkaline substance with a distinct dual toxicological profile, as it completely dissociates into two ions: the hydroxide anion (OH–) and the lithium cation (Li+). As observed in this incident, the affected workers presented with a unique injury profile combining immediate corrosive damage with systemic toxicity.
Primarily, nearly all exposed workers exhibited acute irritation of the respiratory tract, eyes, or skin, consistent with the strong alkaline properties of LiOH. The hydroxide ion (OH–) induces an immediate, localized corrosive effect. As a strong base, LiOH causes severe tissue injury through liquefactive necrosis. Unlike acid-induced coagulative necrosis, which forms a protective eschar, liquefactive necrosis involves the saponification of fats and the denaturation of proteins, transforming tissue into a gelatinous mass. Consequently, alkaline substances penetrate deeper than acids, causing persistent tissue destruction until the alkali is fully neutralized or removed; this extends the injury zone well beyond the initial contact period.15 This mechanism accounts for the severe burning sensation, coughing, and irritation reported by workers immediately post-exposure. Upon contact with the moist mucous membranes of the eyes and respiratory tract, LiOH dust dissolves and dissociates, damaging the epithelial lining. Inhaled fine particles deposit along the respiratory tract—from the nasopharynx to the bronchioles—resulting in chemical bronchitis and tracheitis. The persistence of cough and sputum in many workers 2 weeks post-accident underscores the lingering nature of this damage. Furthermore, the correlation between increased symptom severity and proximity to the leak source suggests a clear dose-response relationship.
Secondary to local effects, lithium cations (Li+) exert systemic toxicity upon absorption. While the toxicity of therapeutic lithium for bipolar disorder is well-documented in psychiatry, its mechanism of action in occupational settings remains under-researched, representing a significant gap in the medical literature. Lithium cations released from LiOH may enter the bloodstream via compromised mucous membranes or the lungs. As a small ion, lithium is widely distributed throughout the body and is not metabolized.16 In cases of acute absorption among lithium-naïve individuals, systemic effects may manifest even if serum concentrations remain below the high levels typically associated with overdose. Many workers reported systemic symptoms—including headache, dizziness, fatigue, abdominal pain, and nausea—that could not be attributed to local irritation alone. These clinical findings align with the known adverse effect profile of lithium, which encompasses neurological (e.g., tremors, cognitive impairment) and gastrointestinal disturbances.17
Several critical lessons emerge from this incident. We emphasize that lithium hydroxide, similar to other strong alkalis like sodium hydroxide, must be managed as a hazardous substance in the workplace. Facilities handling significant quantities of LiOH require strict engineering controls to prevent leakage. The failure of the flexible pipe coupling in this case highlights a potential design or maintenance deficiency. Consequently, enhanced sealing mechanisms or redundant safety features—such as automatic shut-off valves, sealed systems, and scrubbers—are imperative.
Secondly, regarding respiratory protection, symptoms were severe among workers within 10 meters of the exposure source, regardless of the type of respirator utilized. This suggests that standard particulate respirators (dust masks), designed primarily for filtration, were ineffective against the fine, aerosolized particles of highly irritating LiOH. Consequently, handling LiOH powder mandates the use of appropriate chemical-grade respiratory protection alongside chemical splash goggles. Furthermore, as the clinical evaluations of patients referred for persistent respiratory symptoms revealed concurrent cutaneous lesions—such as macules and papules localized to the face and neck—the use of proper protective clothing, including long-sleeved, chemical-resistant suits, is essential to prevent such cutaneous exposure. This incident confirms that relying solely on dust masks and standard workwear is inadequate for protection against LiOH.
Thirdly, the persistence of symptoms underscores the necessity for medical surveillance following such exposures. Workers subject to significant exposure require post-incident health monitoring, including comprehensive respiratory assessments. Pulmonary function tests (PFTs) may be indicated for select individuals to evaluate potential functional impairment, such as acute chemical bronchitis or reactive airways dysfunction syndrome.18 Ocular follow-up is similarly critical, as alkaline injuries can precipitate delayed complications. However, as lithium hydroxide is a relatively novel hazard in this context and is not currently designated as a controlled substance under the Korean Occupational Safety and Health Act, regulatory agencies—including the Ministry of Employment and Labor—have regrettably discontinued long-term follow-up.
Ultimately, these findings highlight the critical importance of emergency preparedness and specialized training in facilities handling corrosive chemicals. The occurrence of a secondary release during the initial cleanup phase indicates significant procedural deficiencies. Effective decontamination protocols—specifically, the use of industrial vacuums with HEPA filters rather than dry sweeping or compressed air blowing—were either absent or improperly executed. Employers must establish a robust incident response plan that includes immediate evacuation, isolation of the hazard area, execution of proper decontamination procedures, and provision of emergency resources (e.g., eyewash stations and emergency showers). It is imperative that employees are thoroughly trained in rapid response protocols to minimize exposure risks.
This study has several limitations. As an observational study conducted in an emergency context, precise quantitative data, such as atmospheric concentration levels or individual dosimeter readings, were unavailable. Reliance on worker recollection for estimating proximity and symptom severity 2 weeks post-incident may have introduced recall bias. Furthermore, the survey did not capture specific psychological sequelae, such as stress or anxiety, which are relevant given the nature of the accident. The absence of objective clinical data, specifically PFTs and serum lithium concentrations, further limits the assessment. Although short-term loss to follow-up was minimal due to a high response rate, long-term surveillance is required to fully elucidate potential chronic health effects.
Notwithstanding these limitations, the overall correlation between physician-recorded clinical symptoms and post-exposure questionnaire responses validates a consistent pattern of local irritation and systemic acute health effects associated with LiOH exposure. Historically, the toxicity of occupational LiOH exposure has been poorly characterized, as standard automated packaging processes typically limit exposure to negligible trace amounts. However, this incident—characterized by a large patient cohort and a homogeneous exposure setting (single site, single substance)—provides a unique and robust dataset for elucidating the acute toxicological profile of LiOH.
CONCLUSIONS
The lithium hydroxide (LiOH) leak incident in Korea in March 2024 not only precipitated severe acute health sequelae among workers but also exposed critical deficiencies in existing preventive protocols. Dozens of workers exhibited chemical irritation of the respiratory tract, eyes, and skin, alongside systemic symptoms indicative of lithium absorption. While the majority of acute symptoms resolved within weeks, the persistence of respiratory pathology in a subset of workers underscores the necessity for longitudinal medical surveillance beyond immediate post-incident intervention. These findings emphasize the substantial occupational hazard posed by LiOH; a single release event has the potential to affect hundreds of individuals and lead to long-term health consequences.
From a practical perspective, this study mandates the urgent implementation of more rigorous safety management protocols for handling LiOH and analogous corrosive agents. A multifaceted approach encompassing engineering controls (e.g., improved isolation and ventilation), administrative measures (e.g., emergency preparedness training and standard operating procedures), and enhanced personal protective equipment is essential to prevent recurrence and safeguard worker health. Notably, effective remediation of the initial spill could have significantly mitigated the secondary exposure event. Furthermore, given the paucity of specific guidelines regarding occupational lithium exposure limits and medical surveillance protocols in current literature and regulations, health authorities and industry leaders are urged to establish comprehensive standards.
Ultimately, this case serves as a critical paradigm of the evolving risks within modern industrial frameworks. As global lithium battery production expands, the potential for occupational exposure to lithium compounds concomitantly rises. It is our hope that the lessons derived from this Korean incident will drive the enhancement of global safety standards and emergency response capabilities to ensure a safer working environment.
Abbreviations
EV
electric vehicle
NIOSH
National Institute for Occupational Safety and Health
PFT
pulmonary function test
-
Competing interests
The authors declare that they have no competing interests.
-
Author contributions
Conceptualization: Lee CG. Data curation: Park SH, Kang JW, Hwang SW, Kim HN, Ko HK. Methodology/formal analysis/validation: Lee CG. Project administration: Lee CG. Writing - original draft: Lee CG. Writing - review & editing: Lee CG, Park SH, Kang JW, Hwang SW, Kim HN, Ko HK.
-
Acknowledgments
We would like to thank Dr. Tae-Woo Kim of K-COMWEL SunCheon Hospital and Dr. Jin-Young Kim, an occupational nurse at the Jeonnam Eastern Workers' Health Center, for reporting the case to the Occupational Disease Surveillance Center. Some of the contents of this paper were presented at the 2024 Summer Conference of Korean Industrial Hygiene Association.
NOTES
Fig. 1.
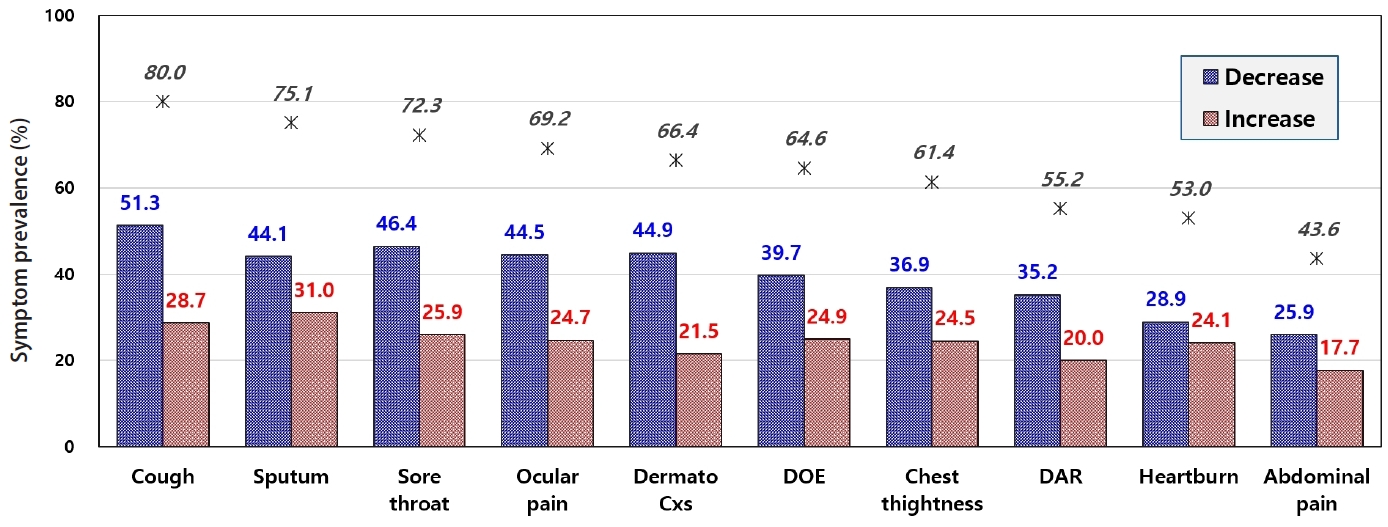
Longitudinal trajectory of symptom severity 2 weeks post-exposure to lithium hydroxide, comparing the severity to the baseline. The denominator symptoms includes all workers who reported a severity score ≥1 at either time point (initial or 2-week follow-up); workers scoring 0 at both time points were excluded. For instance, 80.0% of 474 workers (n = 379) reported cough at either or both time points; among these, 51.3% reported symptom alleviation (decrease in severity score) and 28.7% reported exacerbation (increase in severity score) at the 2-week follow-up relative to initial exposure. DOE: dyspnea on exertion; DAR: dyspnea at rest.
Fig. 2.
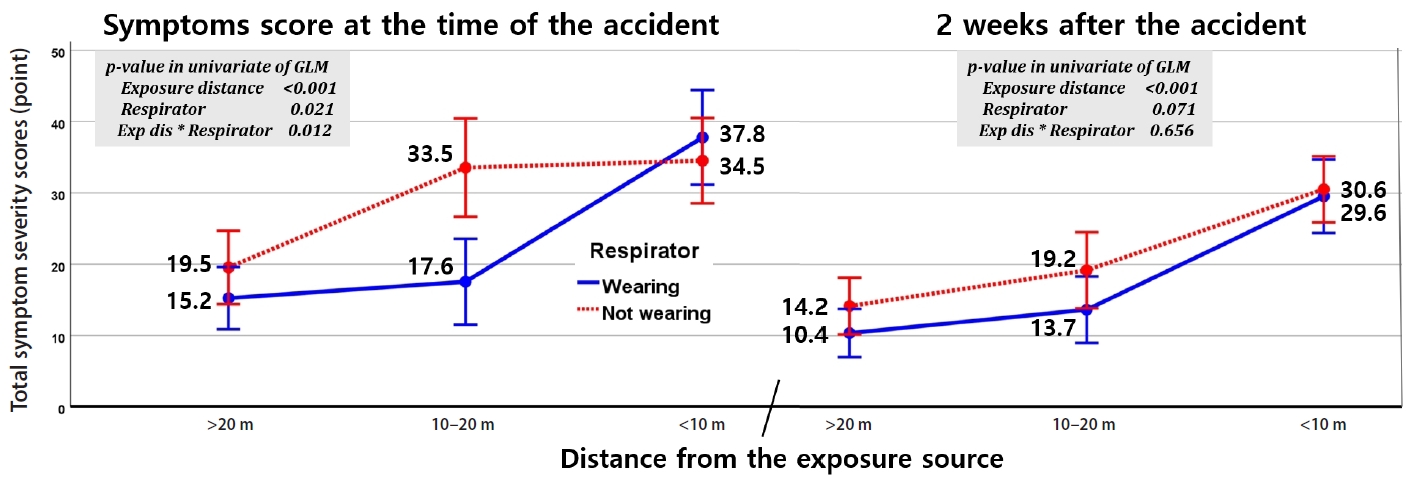
Impact of proximity to the leak source and respirator usage on total symptom severity scores. At the time of the accident (baseline) and 2 weeks post-accident. In the 10–20 m zone, baseline symptom scores were significantly lower for respirator users (17.6) compared to non-users (33.5). While distance and respirator use significantly influenced acute symptom severity (p < 0.001), this statistical significance dissipated at the two-week follow-up (p = 0.071). p-values were calculated using a univariate General Linear Model (GLM).
Table 1.
Acute symptoms in medically evaluated workers
Table 2.
Symptom prevalence and severity at exposure vs. 2 weeks later
- 1. Calisaya-Azpilcueta D, Herrera-Leon S, Lucay FA, Cisternas LA. Assessment of the supply chain under uncertainty: the case of lithium. Minerals 2020;10(7):604.Article
- 2. Fitch B, Yakovleva M, Meiere S. Lithium hydroxide based performance improvements for nickel rich NCM layered cathode material. Electrochemical Society Meeting Abstracts, Vol. MA2016-02. Pennington, NJ: The Electrochemical Society, Inc.; 2016, 469.ArticlePDF
- 3. Saaid FI, Kasim MF, Winie T, Elong KA, Azahidi A, Basri ND, et al. Ni-rich lithium nickel manganese cobalt oxide cathode materials: a review on the synthesis methods and their electrochemical performances. Heliyon 2024;10(1):e23968.ArticlePubMedPMC
- 4. Kamal ZM, Dutta S, Rahman S, Etando A, Hasan E, Nahar SN, et al. Therapeutic application of lithium in bipolar disorders: a brief review. Cureus 2022;14(9):e29332.ArticlePubMedPMC
- 5. Judkins DG, Chen RJ, McTeer AV. Alkali toxicity. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2023.
- 6. Wen J, Sawmiller D, Wheeldon B, Tan J. A review for lithium: pharmacokinetics, drug design, and toxicity. CNS Neurol Disord Drug Targets 2019;18(10):769–78.ArticlePubMed
- 7. Bortolozzi A, Fico G, Berk M, Solmi M, Fornaro M, Quevedo J, et al. New advances in the pharmacology and toxicology of lithium: a neurobiologically oriented overview. Pharmacol Rev 2024;76(3):323–57.ArticlePubMedPMC
- 8. Sakrajda K, Rybakowski JK. The mechanisms of lithium action: the old and new findings. Pharmaceuticals (Basel) 2025;18(4):467.ArticlePubMedPMC
- 9. Salisbury S, Keenlyside R. Health Hazard Evaluation Report: HHE-80-036-922. Bessemer City, NC: Lithium Corporation of America; 1981.
- 10. Greenspan BJ, Allen MD, Rebar AH. Inhalation toxicity of lithium combustion aerosols in rats. J Toxicol Environ Health 1986;18(4):627–37.ArticlePubMed
- 11. Frolova AD, Chekunova MP, Vasil'kovskii VG, Kuz'minskaia GN, Teterkina OA. Toxicology and hygienic regulation of lithium and its salts in the air of work areas. Med Tr Prom Ekol 1993;(3-4):37–8.
- 12. Aral H, Vecchio-Sadus A. Toxicity of lithium to humans and the environment: a literature review. Ecotoxicol Environ Saf 2008;70(3):349–56.ArticlePubMed
- 13. Lagerkvist BJ, Lindell B. The Nordic Expert Group for Criteria Documentation of Health Risks from Chemicals: 131. Lithium and Lithium Compounds. Stockholm, Sweden: National Institute for Working Life; 2002.
- 14. Kim JC, Kang SY, Chung BY, Park CW, Kim HO. Case report: erythema multiforme induced by lithium contact. Ann Dermatol 2023;35(Suppl 2):S225–8.ArticlePubMedPMCPDF
- 15. Lam W, Neupane R, Marks JM. Acidic and basic injuries. In: Docimo S Jr, Pauli EM, editors. Clinical Algorithms in General Surgery: A Practical Guide. Cham, Switzerland: Springer; 2019, 143–5.
- 16. Bauer M, Grof P, Muller-Oerlinghausen B. Lithium in Neuropsychiatry: The Comprehensive Guide. Boca Raton, FL: CRC Press; 2013.
- 17. Kansagra AJ, Yang E, Nambiar S, Patel PS, Karetzky MS. A rare case of acute respiratory distress syndrome secondary to acute lithium intoxication. Am J Ther 2014;21(2):e31–4.ArticlePubMed
- 18. Brooks SM. Then and now reactive airways dysfunction syndrome. J Occup Environ Med 2016;58(6):636–7.ArticlePubMed
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Sustainable Working Life Within the Production and Recycling of Lithium-Ion Batteries for Electric Vehicles (GreenWorkLiB)
Klara Midander, Anneli Julander, Erik Rosengren, Sandra Johannesson, Florencia Harari
Batteries.2026; 12(6): 203. CrossRef
 Cite
CiteAcute health effects of accidental exposure to lithium hydroxide at a battery material production plant
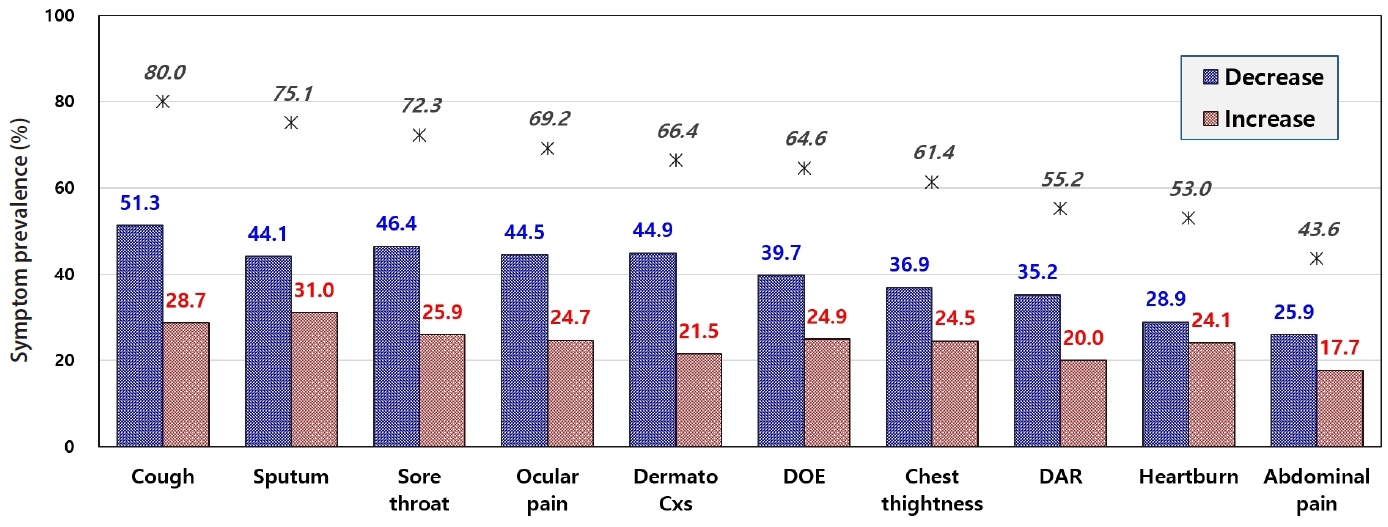
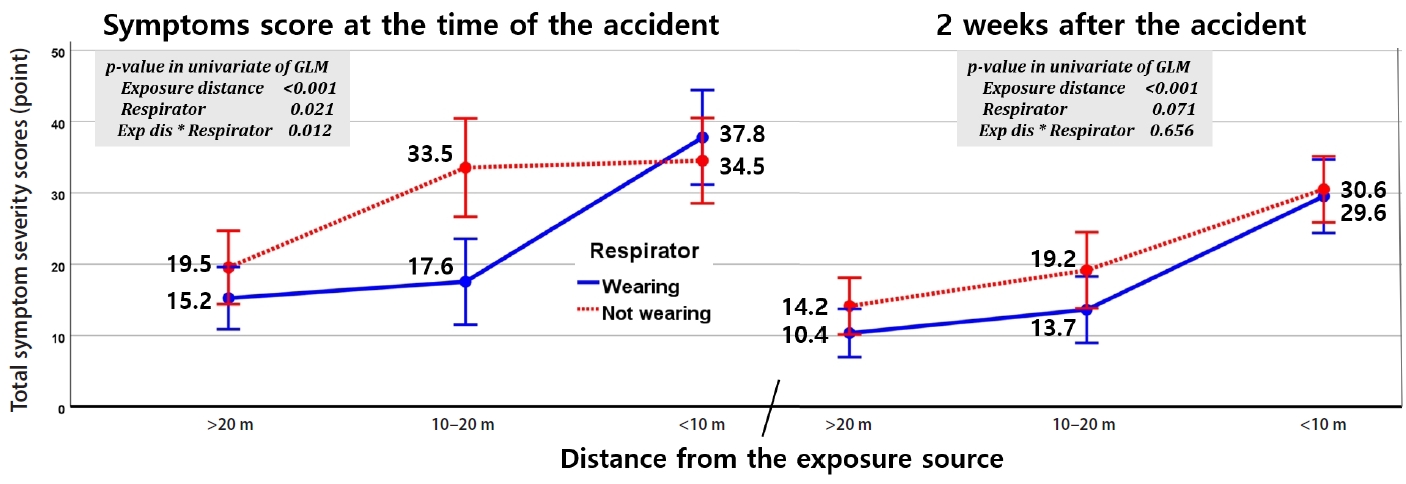
Fig. 1. Longitudinal trajectory of symptom severity 2 weeks post-exposure to lithium hydroxide, comparing the severity to the baseline. The denominator symptoms includes all workers who reported a severity score ≥1 at either time point (initial or 2-week follow-up); workers scoring 0 at both time points were excluded. For instance, 80.0% of 474 workers (n = 379) reported cough at either or both time points; among these, 51.3% reported symptom alleviation (decrease in severity score) and 28.7% reported exacerbation (increase in severity score) at the 2-week follow-up relative to initial exposure. DOE: dyspnea on exertion; DAR: dyspnea at rest.
Fig. 2. Impact of proximity to the leak source and respirator usage on total symptom severity scores. At the time of the accident (baseline) and 2 weeks post-accident. In the 10–20 m zone, baseline symptom scores were significantly lower for respirator users (17.6) compared to non-users (33.5). While distance and respirator use significantly influenced acute symptom severity (p < 0.001), this statistical significance dissipated at the two-week follow-up (p = 0.071). p-values were calculated using a univariate General Linear Model (GLM).
Fig. 1.
Fig. 2.
Acute health effects of accidental exposure to lithium hydroxide at a battery material production plant
| No. (%) (n = 115) | |
|---|---|
| Local irritation symptoms | |
| Sore throat | 67 (58.3) |
| Cough | 33 (28.7) |
| Dermatological complications | 20 (17.4) |
| Nasal congestion or rhinorrhea | 13 (11.3) |
| Ocular pain | 13 (11.3) |
| Sputum | 11 (9.6) |
| Dry mouth and sore | 6 (5.2) |
| Systemic symptoms | |
| Headache | 52 (45.2) |
| Nausea | 21 (18.3) |
| Chest tightness | 14 (12.2) |
| Dizziness | 11 (9.6) |
| Generalized fatigue | 10 (8.7) |
| Diarrhea | 6 (5.2) |
| Sleep disturbances | 3 (2.6) |
| Slight (1–3) | Moderate (4–6) | Severe (7–10) | Total | |||||
|---|---|---|---|---|---|---|---|---|
| Initial | After 2 weeks | Initial | After 2 weeks | Initial | After 2 weeks | Initial | After 2 weeks | |
| Cough | 18.8 | 31.0 | 21.3 | 23.8 | 22.2 | 10.1 | 62.2 | 65.0 |
| Sputum | 23.0 | 34.6 | 17.5 | 19.6 | 17.5 | 8.9 | 58.0 | 63.1 |
| Sore throat | 17.1 | 30.0 | 18.1 | 17.7 | 20.0 | 7.8 | 55.3 | 55.5 |
| Eyes sting | 20.0 | 29.7 | 18.6 | 15.6 | 16.2 | 7.6 | 54.9 | 53.0 |
| Skin trouble | 18.1 | 28.1 | 18.4 | 13.5 | 15.2 | 6.1 | 51.7 | 47.7 |
| DOE | 19.4 | 29.3 | 17.5 | 13.5 | 12.4 | 5.9 | 49.3 | 48.7 |
| DAR | 17.7 | 23.2 | 15.4 | 12.7 | 8.9 | 3.6 | 42.0 | 39.5 |
| Chest tightness | 18.1 | 27.2 | 16.0 | 10.5 | 11.2 | 7.4 | 45.4 | 45.1 |
| Heartburn | 17.1 | 24.7 | 13.5 | 10.8 | 8.2 | 6.1 | 38.8 | 41.6 |
| Abdominal pain | 14.3 | 21.5 | 10.8 | 9.1 | 7.4 | 3.2 | 32.5 | 33.8 |
Table 1. Acute symptoms in medically evaluated workers
Table 2. Symptom prevalence and severity at exposure vs. 2 weeks later
Values are presented as percentage. DOE: dyspnea on exertion; DAR: dyspnea at rest.

