
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 38; 2026 > Article
- Case Report Case series: from ventilation failure to substitution success in occupational lead poisoning at a Korean indoor firing range
-
Chul Gab Lee1,2,*
 , Soo Hyeong Park1,2
, Soo Hyeong Park1,2 -
Annals of Occupational and Environmental Medicine 2026;38:e5.
DOI: https://doi.org/10.35371/aoem.2026.38.e5
Published online: February 9, 2026
1Department of Occupational and Environmental Medicine, Chosun University Hospital, Gwangju, Korea
2Gwangju Branch of Korea Occupational Disease Surveillance Center, Gwangju, Korea
- *Corresponding author: Chul Gab Lee Department of Occupational and Environmental Medicine, Chosun University Hospital, 365 Pilmun-daero, Dong-gu, Gwangju 61453, Korea E-mail: eecg@daum.net, cglee@chosun.ac.kr
• Received: December 8, 2025 • Revised: January 30, 2026 • Accepted: January 30, 2026
© 2026 Korean Society of Occupational & Environmental Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,037 Views
- 84 Download
Abstract
-
Background Indoor firing ranges are globally recognized as high-risk settings for occupational and recreational lead exposure due to the use of lead-based ammunition and frequently inadequate ventilation systems. In Korea, however, public health surveillance and regulatory oversight have remained limited. This case series empirically demonstrates that in high-emission settings like indoor firing ranges, ventilation upgrades are insufficient. Source substitution with lead-free primer ammunition proved to be the only definitive intervention.
-
Case presentation In late 2023, an index case presenting with abdominal pain was found to have a blood lead level (BLL) of 55 µg/dL, prompting a government-mandated investigation. Nine male shooting instructors (tenure: 4–65 months) were subsequently identified with BLLs ranging from 38.2–73.2 µg/dL, while airborne lead concentrations (ALC) reached 0.51 mg/m³—10 times the occupational exposure limit (OEL: 0.05 mg/m³). During a 3-month closure to upgrade ventilation, workers received chelation therapy (CaNa₂EDTA and D-penicillamine), which reduced their BLLs to 3.2–25.7 µg/dL. However, 2 months after reopening, post-intervention ALC remained elevated at 0.0797 mg/m³, still exceeding the OEL, and BLLs rebounded to 16.2–53.3 µg/dL. A substitution strategy was then implemented, replacing lead-based ammunition with copper-clad, lead-free primer rounds. This intervention decreased ALC to <0.003 mg/m³ and lowered BLLs to 4.9–23.1 µg/dL. Despite the reduced airborne concentrations, several workers continued to exhibit BLLs around 20 µg/dL, suggesting subtle ongoing exposure and mobilization of bone-stored lead.
-
Conclusions This cluster demonstrates that in environments where hazardous agents are continuously generated, such as indoor firing ranges, engineering controls alone, such as improved ventilation, may not provide adequate protection. Substitution—the most effective intervention within the hierarchy of controls—was essential for eliminating exposure. Furthermore, the toxicokinetics of bone lead in chronically exposed adults highlight the need for ongoing monitoring and cautious decision-making regarding treatment and return-to-work planning.
BACKGROUND
Lead is a pervasive and potent multisystem toxicant with no known safe level of exposure.1 A substantial body of evidence confirms that adverse health effects occur in both children and adults at blood lead levels (BLLs) below 10 μg/dL and even at levels below 5 μg/dL.2 In adults, chronic low-level exposure is associated with a range of deleterious outcomes, including hypertension, cardiovascular disease, renal dysfunction, cognitive decline, and reproductive harm.3 Both the European Union4 and California in the United States5 have recently strengthened occupational lead exposure standards, reflecting growing epidemiological evidence that chronic low-level lead exposure can cause adverse health effects at blood lead concentrations below traditional occupational thresholds (Table 1).
Although the reinforcement of the Occupational Safety and Health (OSH) Act in Korea has successfully reduced lead poisoning in traditional lead-processing industries—such as smelting and battery manufacturing—recreational indoor firing ranges remain a significant and often inadequately regulated source of high-intensity exposure.6 The discharge of firearms using conventional ammunition releases a complex aerosol of lead-containing particulates. This process involves two primary mechanisms: the detonation of lead styphnate in the primer, and the vaporization and mechanical abrasion of the lead bullet as it traverses the barrel at high temperatures and pressures. These fine and ultrafine particles contaminate the air and surfaces, placing shooters, instructors, and maintenance personnel at high risk of exposure via inhalation and inadvertent ingestion.6-8 Globally, outbreaks of lead poisoning linked to firing ranges are well-documented, affecting millions of individuals, including law enforcement personnel, military staff, and recreational users.
The Korean Special Health Examination (SHE) system,9 established under the OSH Act, mandates periodic medical surveillance for workers exposed to occupational hazards. The system employs a standardized classification scheme based on both clinical severity and causality. Examination results are categorized by stage—‘C’ (observation or preventive management) or ‘D’ (diagnosis requiring active medical management)—and by etiology—‘1’ (occupational) or ‘2’ (non–work-related). Importantly, classifications of C1 and D1 carry legal implications, obligating employers to implement environmental control measures and to make fitness-for-duty adjustments, including work restrictions or job reassignment. In contrast, C2 and D2 classifications indicate non-occupational conditions, for which clinical management is shifted to personal medical care rather than workplace intervention. Despite this well-defined regulatory framework, recreational indoor firing ranges in Korea had remained largely outside formal occupational health oversight until late 2023. This regulatory gap became evident when a shooting coach presented to an emergency department with severe abdominal pain and was found to have a BLL of 55 µg/dL. This value exceeded the D1 threshold (≥40 µg/dL), constituting a legally recognized occupational disease and triggering a nationwide investigation by the Ministry of Employment and Labor (MOEL) and the Korea Occupational Safety and Health Agency (KOSHA). The investigation revealed systemic regulatory failures: 59.1% of the 22 inspected indoor firing ranges exceeded the occupational exposure limit (OEL) for airborne lead concentrations (ALC) (0.05 mg/m³ or 50 µg/m3), and 26.4% of the 87 tested workers were legally classified as D1 cases, necessitating immediate corrective action.
This case series analyzes nine workers from the most severely affected facility to provide insights into workplace interventions and the outcomes of chelation therapy. The objectives are to evaluate the effectiveness of sequential workplace interventions guided by the hierarchy of controls, and to describe the clinical course, outcomes, and challenges inherent in managing severely exposed workers.
CASE PRESENTATION
This descriptive case series examines nine male shooting coaches employed at a single commercial indoor firing range in J City, Korea. These workers were identified with elevated BLLs during a special investigation mandated by MOEL in early 2024. Demographic data, including age and duration of employment, are presented in Table 2. The facility operated eight shooting lanes within a confined area measuring 20 m (L) × 16 m (W) × 2.5 m (H). Various pistol calibers (380 ACP, 9 mm, and 357 Magnum) were used, with a total daily discharge of 2,500 to 4,000 rounds. This study details the sequential interventions implemented to mitigate lead exposure and describes clinical management, including chelation therapy, administered to reduce BLLs in the affected workers.
At the initial screening in March 2024, eight of the nine workers exhibited BLLs exceeding 40 µg/dL, classifying them as ‘D1.’ Consequently, they were referred to the Department of Occupational and Environmental Medicine at the Korea Occupational Disease Surveillance Center (KODSC) for evaluation of chelation therapy eligibility. Clinically, the workers presented with typical symptoms of lead toxicity. Neurological complaints included chronic migraines, fatigue, and finger cramps, while gastrointestinal symptoms included recurrent abdominal pain, dyspepsia, and diarrhea. Cases A (73.2 µg/dL) and C (72.4 µg/dL) exhibited the most severe lead poisoning. Specifically, cases A and F reported chronic headaches and fatigue, whereas cases B and G reported gastrointestinal distress. Notably, cases C, D, and E experienced recurrent intermittent finger stiffness. In case E, electromyography findings were consistent with peripheral neuropathy, suggesting that lead exposure had affected peripheral motor nerves, potentially slowing nerve conduction velocity or causing axonal degeneration.
Chelation therapy was initiated for the eight workers (cases A–H) meeting the D1 criterion (40 µg/dL). Case I (initial BLL 38.2 µg/dL) subsequently received one course of therapy in August 2024. The therapeutic goal was to achieve a stable BLL below 20 µg/dL on at least two consecutive measurements. The inpatient procedure utilized combination therapy comprising intravenous calcium disodium ethylene-diamine-tetra-acetate (CaNa2EDTA) and oral D-penicillamine. CaNa2EDTA was administered at 1 g twice daily (total 2 g/day) for 7 days, alongside oral D-penicillamine at 750 mg/day. To minimize the risk of nephrotoxicity, aggressive hydration was maintained with 2,000 mL of fluids daily. Furosemide (10 mg) was administered to ensure urine output exceeded 2,000–3,000 mL/day. Patients were monitored closely for 24 hours for signs of toxic encephalopathy, and lead concentrations in blood and urine were measured daily for 7 days. No serious adverse events occurred, except for temporary hypertension in case B on day 4 of EDTA administration. Post-discharge, two patients reported pruritus associated with oral penicillamine and were treated with antihistamines.
A chronological series of environmental assessments and interventions was implemented to mitigate lead exposure. The variations in ALC throughout this period are summarized in Table 2 and Fig. 1.
(1) Initial assessment (March 2024): Initial measurements indicated significant occupational overexposure. The area sample collected at the shooting line was 0.51 mg/m3, exceeding the Korean OEL of 0.05 mg/m3 by tenfold. Personal samples for two workers (cases E and I) measured 0.29 mg/m3 and 0.45 mg/m3, respectively, confirming significant occupational overexposure.
(2) Intervention 1 (engineering control, May–August 2024): The facility underwent a 3-month closure to upgrade the ventilation system. The existing system, a simple exhaust-only design with a hood positioned 16 meters from the shooting line, was deemed insufficient for source capture. It was upgraded to increase blower capacity, achieving a supply and exhaust air volume of 650 m3/min. Concurrently, affected workers received inpatient medical treatment during this closure period.
(3) Post-intervention assessment and control limitations: Following the facility’s reopening in September 2024, a follow-up assessment was conducted in October 2024 to verify the efficacy of the engineering controls. Results indicated that ventilation improvements alone failed to achieve regulatory compliance. Personal air samples for cases B, C, and F were 0.0797 mg/m3, 0.0772 mg/m3, and 0.0726 mg/m3, respectively (Table 2), all of which remained above the OEL. Furthermore, workers’ BLLs, which had declined during the closure, increased markedly upon their return. For instance, case B’s BLL rose from 15.9 µg/dL to 53.3 µg/dL. These findings demonstrated that the hazard remained uncontrolled despite improved ventilation, resulting in the re-exposure of workers to hazardous lead levels.
(4) Intervention 2 (source substitution): Consequently, in late October 2024, the workplace escalated measures according to the hierarchy of controls. The facility mandated the exclusive use of encapsulated ammunition (total metal jacket), featuring a lead core fully enclosed by a copper jacket and a lead-free primer. This design prevents hot propellant gases from vaporizing lead at the bullet's base and eliminates lead styphnate smoke.
(5) Final assessments (November and December 2024): Substantial improvements were observed by 1-month post-substitution. In November 2024, the sample from case B was below the limit of detection, and case C measured 0.007 mg/m3. By December 2024, all individual samples were below 0.003 mg/m3, confirming that source substitution successfully reduced exposure to negligible levels.
The longitudinal changes in BLLs for the nine workers are detailed in Table 2 and Fig. 1. Following the initial hospitalization (May–August 2024), BLLs decreased substantially; case D reached a nadir of 3.2 µg/dL. However, a clinically significant rise in BLLs was observed in the six workers (cases A–F) who returned to the facility in September 2024 prior to the ammunition substitution. This resurgence, exemplified by case B (53.3 µg/dL), necessitated additional chelation therapy and was attributed primarily to occupational re-exposure rather than endogenous redistribution alone. In contrast, the three workers (cases G, H, and I) who resigned in September 2024 and avoided re-exposure did not experience this sharp increase. Their BLLs demonstrated a steady decline or stability. By May 2025, following the full implementation of encapsulated ammunition, BLLs for all workers stabilized at lower levels. However, the continuing workers (e.g., cases B and C) maintained slightly higher BLLs compared to those who resigned, likely reflecting the mobilization of cumulative bone lead burden.
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki. The present study protocol was reviewed and approved by the Institutional Review Board of CHOSUN IRB (approval No. 2025-08-002). Informed consent was submitted by all subjects when they were enrolled.
DISCUSSION AND CONCLUSION
These unexpected cases of lead poisoning at an indoor firing range in Korea offer critical insights into regulatory gaps and occupational health management. First, the incident highlights a significant regulatory blind spot regarding the emerging recreational firing industry. Historically, Korea has achieved substantial success in reducing occupational lead exposure. Nationwide work environment monitoring data indicate that the geometric mean of ALC in lead-handling workplaces decreased from 3.14 µg/m3 in 1994 to 1.11 µg/m3 in 2021.10 Furthermore, an analysis of 365,331 SHE cases (2003–2011) revealed that the geometric mean of BLLs declined from 5.89 µg/dL to 3.53 µg/dL. Notably, the prevalence of workers exceeding 30 µg/dL (C1 criterion) dropped from 4.3% to 0.8%, and those exceeding 40 µg/dL (D1 criterion) fell from 1.32% to 0.16%.11 In tandem with these declining trends, Korean regulators strengthened the OEL for ALC from 150 µg/m3 (in 1990) to 50 µg/m3, and tightened the biological exposure indices (BEI) within the SHE system in 2009 lowering the C1 threshold from 40 to 30 µg/dL and D1 from 60 to 40 µg/dL.10 However, indoor firing ranges were largely excluded from this surveillance framework, as they were categorized as part of the expanding leisure service sector rather than traditional manufacturing. Consequently, the severe exposure identified in March 2024—where ALC levels reached 290-450 µg/m3 (0.29–0.45 mg/m3)—was an unanticipated regulatory failure that has since sparked significant public health debate.
Second, the assumption that enhanced ventilation alone could prevent lead poisoning proved insufficient. Despite engineering interventions, hazardous exposure persisted. This case underscores that the only definitive safety measure is source elimination: specifically, the replacement of conventional lead-based ammunition with encapsulated or lead-free alternatives. This aligns with the hierarchy of controls, where substitution is far more effective than engineering controls in this specific environment.
Third, the clinical management of severe cases remains a challenge. The incident raises important questions regarding the therapeutic benefit of chelation therapy for symptomatic workers with BLLs exceeding the D1 threshold (≥40 µg/dL). Further discussion is needed to establish clear clinical endpoints, specifically determining the target BLL to which patients should be reduced to ensure long-term safety.
Mechanics of contamination and exposure pathways
This case provides a compelling illustration of the occupational hygiene principle known as the 'hierarchy of controls.' The contamination process initiates the moment a firearm is discharged. The primer, typically containing lead styphnate, detonates, and the lead bullet travels through the barrel, generating extreme heat and pressure. This process vaporizes, melts, and mechanically abrades the lead from both the primer and the bullet, releasing a complex aerosol of lead-containing dust, smoke, and gas.6,8 This aerosol, composed of fine and ultrafine particles, acts as the primary vector of exposure, contaminating the air, surfaces, and ventilation systems. Specifically, the combustion of gunpowder and the friction of the bullet generate lead fumes that oxidize upon contact with atmospheric oxygen at temperatures exceeding 1,000°C. Consequently, instructors standing in proximity to the shooter inhale high concentrations of lead dust and smoke. Furthermore, secondary exposure occurs through dermal contact or ingestion while handling spent cartridges or cleaning the facility. Prior to MOEL’s investigation, these workers lacked specific training on lead hazards and did not distinguish between work and casual clothing, exacerbating the risk. This highlights that without addressing the source, ancillary measures are insufficient.
Limitations of engineering controls (ventilation)
Despite the implementation of a “push-pull” ventilation system—an engineering control designed to provide a substantial airflow of 650 m3/min—the ALC remained above the OEL (0.05 mg/m3 or 50 µg/m3). This failure can be attributed to the aerodynamic characteristics of the contaminant and the insufficient capture velocity relative to the emission speed.12 Lead fumes generated during discharge expand explosively at high velocities and temperatures. According to American Conference of Governmental Industrial Hygienists guidelines, capturing such high-velocity fugitive emissions requires exceptionally high control velocities. However, the "push" air supply behind the shooter can induce a “backflow effect,” creating turbulence and eddy currents around the shooter’s body that trap contaminants in the breathing zone.13 This issue is aggravated when multiple shooters fire simultaneously in a confined space (20 m × 16 m × 2.5 m), severely compromising ventilation efficiency. Moreover, general dilution ventilation is inherently unsuitable for highly toxic substances like lead. While local exhaust ventilation is theoretically ideal, installing hoods close to the emission source presents structural challenges, as it obstructs the shooter's field of vision and mobility.14,15 Thus, relying solely on ventilation proved to be an inadequate control strategy.
Efficacy of source substitution
A significant reduction in ALC was ultimately achieved only by ascending the hierarchy of controls to substitution. The facility replaced conventional lead-primer ammunition with encapsulated, "environmentally friendly" alternatives (total metal jacket with lead-free primers). Subsequently, ALC levels plummeted to well below the OEL. This outcome empirically demonstrates that eliminating the hazard or substituting it with a less hazardous alternative is a far more effective and reliable intervention than relying on lower-level measures such as engineering controls (ventilation) or personal protective equipment.6,16-18
In this instance, the failure of engineering controls (ventilation) to lower ALC posed a critical legal risk to the employer. Recognizing that partial mitigation measures could not guarantee compliance or immunity from prosecution under the Serious Accident Punishment Act—enacted in 2022 amidst intense social controversy in Korea—the employer was compelled to invest in fundamental source substitution, despite its higher operational costs, rather than relying solely on engineering retrofits. This case illustrates that stringent legal frameworks can effectively alter the cost-benefit analysis of safety management, driving employers to prioritize intrinsic safety measures to prevent severe health outcomes. Furthermore, this regulatory imperative to prevent critical occupational illnesses necessitates a re-evaluation of the clinical distinction between ‘lead exposure’ and ‘lead poisoning,’ as the definitions of these terms fundamentally dictate both the medical response and the ethical obligations of the practitioner.
While institutional guidelines for chelation therapy in lead poisoning vary slightly, there is universal consensus that eliminating the source of exposure is the fundamental principle of prevention and treatment. Furthermore, it is well-established that no safe BLL exists for children. A critical question, therefore, arises: why is chelation therapy typically considered only when BLLs exceed 50 μg/dL, despite accumulating evidence that BLLs as low as 10 μg/dL can cause long-term adverse effects on multiple organ systems, including cardiovascular disease?3
Several factors contribute to this clinical uncertainty. First, while BLL is the most convenient and widely used biomarker, it has limitations. Since lead has a relatively short half-life in blood of approximately 30 days, BLL primarily reflects recent exposure. Consequently, a single BLL measurement is insufficient to reliably quantify cumulative dose or total body burden, nor can it definitively confirm or exclude chronic lead-related health effects. In adults, over 90% of the body burden of lead is sequestered in bone and teeth, where it has a biological half-life of 20–30 years.19-21 This skeletal reservoir poses a risk of endogenous remobilization into the bloodstream during periods of increased bone turnover—such as pregnancy, lactation, menopause, or specific metabolic states—thereby complicating clinical management. For these reasons, uniformly recommending chelation therapy for patients with elevated BLLs, particularly those who are asymptomatic, may be inappropriate. In the present case, however, chelation was deemed necessary because the workers presented with BLLs ranging from 38.2 to 72.2 μg/dL and exhibited various symptoms, even though these symptoms were not severe enough to completely incapacitate their daily lives.
Second, and crucially, clinical decisions often rely on extrapolation from pediatric studies due to a lack of data in adults. A comprehensive analysis of the Treatment of Lead-Exposed Children (TLC) trial demonstrated that while children treated with the drug succimer showed significantly lower mean BLLs compared to the placebo group during the first 6 months, these reductions were transient.22 Importantly, succimer treatment did not translate into measurable cognitive, neuropsychological, behavioral, or neuromotor benefits at long-term follow-up assessments conducted at 36 months and 7 years of age.23,24 The consistent conclusion from the TLC trial is that chelation therapy is ineffective in reversing neurodevelopmental deficits in children with BLLs below 45 µg/dL. Although these findings are specific to children, they reinforce the hesitation to recommend chelation in adults where long-term benefits are similarly unclear. While it is known that BLLs as low as 10 µg/dL increase the risk of hypertension and renal dysfunction, there is a lack of systematic evidence supporting the efficacy of chelation in preventing these outcomes in asymptomatic adults. Consequently, potential adverse effects of therapy often weigh heavily against its uncertain benefits in clinical decision-making.
Third, from a toxicokinetic perspective, the redistribution of lead presents a significant challenge. As noted, over 95% of total body lead in adults is stored in the skeleton.25 Even if lead is successfully cleared from the blood and soft tissues through chelation, a “rebound” phenomenon often occurs as lead re-equilibrates from these large bone stores back into the bloodstream, potentially raising BLLs again. In the context of the Korean workforce, occupational lead exposure has drastically declined; the geometric mean BLL of lead-exposed workers dropped from 5.89 μg/dL in 2003 to 3.53 μg/dL in 2011,11 with only 0.16% of 50,000 monitored workers exceeding 40 μg/dL. Furthermore, the average BLL of the general adult population in Korea (2023) is 1.75 μg/dL (geometric mean 1.44), with a 95th percentile of 3.62 μg/dL.26 Given these trends, current BLLs in workers are likely even lower than in 2011. Against this backdrop of successful national control, the extremely high ALCs and BLLs detected at the indoor shooting range represent a stark anomaly. This incident brought to light a significant blind spot in workplace safety regulations regarding recreational facilities.
Since then, a debate has emerged among occupational physicians regarding the appropriate management of lead exposure in indoor firing ranges and the clinical protocols for workers with elevated BLLs. Many practitioners classify the elevated BLLs observed in these workers as ‘lead exposure’ rather than ‘lead poisoning,’ arguing that chelation therapy is therefore not indicated. However, in occupational toxicology, ‘exposure’ typically denotes a hazard-based concept, whereas ‘poisoning’ signifies a risk-based clinical pathology. While decisions regarding chelation therapy require a careful medical evaluation of the risk-benefit balance, physicians bear a paramount ethical obligation to intervene—not merely to treat, but to mitigate hazardous working conditions that pose ongoing threats to workers’ health. Consequently, the distinction between framing health effects as ‘lead exposure’ versus ‘lead poisoning’ is not merely semantic but reflects a broader philosophical difference regarding intervention strategies within occupational medicine.
Ultimately, in this case series, occupational lead exposure was successfully mitigated, and the body burden of lead was reduced through chelation therapy.27 While the long-term health implications for these workers remain to be fully elucidated, no significant adverse events were observed during treatment. It is anticipated that the therapeutic benefits will outweigh potential risks in the long term. However, the findings of this report should be interpreted with caution due to limitations inherent in a descriptive case series, including a small sample size, the restriction to a single workplace, and the absence of a control group.
Although this descriptive case series focuses on a single workplace event, it highlights a critical public health blind spot that demands immediate attention in Korea.28 This incident identified that approximately 22 indoor firing ranges are currently operating in Korea. At the facility where the case occurred, daily attendance ranged from 200 to 400 individuals, suggesting that an estimated 100,000 civilians are potentially exposed to lead annually. Despite these figures, the absence of systematic occupational health management has resulted in a lack of reliable data regarding the total number of range employees and the general population engaged in recreational shooting nationwide. Furthermore, there is limited transparency concerning environmental remediation measures taken by other facilities following the MOEL investigation. Due to this lack of data, longitudinal studies are essential to evaluate BLLs and associated health outcomes. Such research should specifically facilitate a comparative analysis between workers at facilities that have transitioned to lead-free ammunition and those that continue to use conventional lead-based ammunition.
Historically, occupational safety frameworks have often functioned reactively, addressing hazards only after health damages are confirmed, rather than proactively anticipating risks.29 However, this incident should serve as a wake-up call to public health authorities worldwide.30 Crucially, this case aligns with a rapidly evolving global consensus toward stricter lead regulation. Notably, in the 2024–2025 period, major international regulatory bodies, including the European Union and California Division of Occupational Safety and Health,4,5 have moved to significantly lower the OELs for airborne lead and the BEIs for BLLs (Table 1). These legislative shifts reflect a growing scientific recognition that previously accepted thresholds are insufficient to protect workers from chronic toxicity. Korea’s regulations urgently need updating to meet stricter global standards. It is imperative to move beyond broad oversight and adopt more granular management strategies that can detect and mitigate risks in non-traditional sectors, such as the emerging leisure industry.
Therefore, for indoor shooting ranges in Korea and elsewhere, this report advocates for a dual-pronged approach: a systematic transition to intrinsic safety measures—specifically, the mandatory use of lead-free primers and encapsulated ammunition—and the implementation of enhanced, proactive health surveillance programs that harmonize with the heightened global standards for lead control.
Abbreviations
ACOEM
American College of Occupational and Environmental Medicine
ACGIH
American Conference of Governmental Industrial Hygienists
ALC
airborne lead concentration
BEI
biological exposure index
BLL
blood lead level
BLV
biological limit value
Cal/OSHA
California Division of Occupational Safety and Health
CFR
Code of Federal Regulations
EU
European Union
JSOH
Japan Society for Occupational Health
KODSC
Korea Occupational Disease Surveillance Center
KOSHA
Korea Occupational Safety and Health Agency
MOEL
Ministry of Employment and Labor
ND
non-detect
NIOSH
National Institute for Occupational Safety and Health
OEL
occupational exposure limit
OSH
Occupational Safety and Health
OSHA
Occupational Safety and Health Administration
PEL
permissible exposure limit
REL
recommended exposure limit
SHE
Korean Special Health Examination
TLC
Treatment of Lead-Exposed Children
TLV-TWA
threshold limit value–time-weighted average
TWA
time-weighted average
-
Competing interests
The authors declare that they have no competing interests.
-
Author contributions
Conceptualization: Lee CG. Data curation: Park SH. Methodology/formal analysis/validation: Lee CG. Project administration: Lee CG. Writing - original draft: Lee CG. Writing - review & editing: Lee CG.
-
Acknowledgments
We express our sincere gratitude to the officials of the Ministry of Employment and Labor (MOEL) for their trust and active cooperation in the treatment and prevention efforts. We also thank Dr. Hyeongyeong Choi of the Jeju KMI Center for identifying and referring these lead poisoning cases for chelation therapy. Furthermore, we appreciate the dedicated assistance of Ji Won Kang, Si Woo Hwang, Hyeo Na Kim, and Hyeon Kyeong Ko from the Gwangju branch of the Korea Occupational Disease Surveillance Center (KODSC) throughout the clinical management process.
NOTES
Fig. 1.
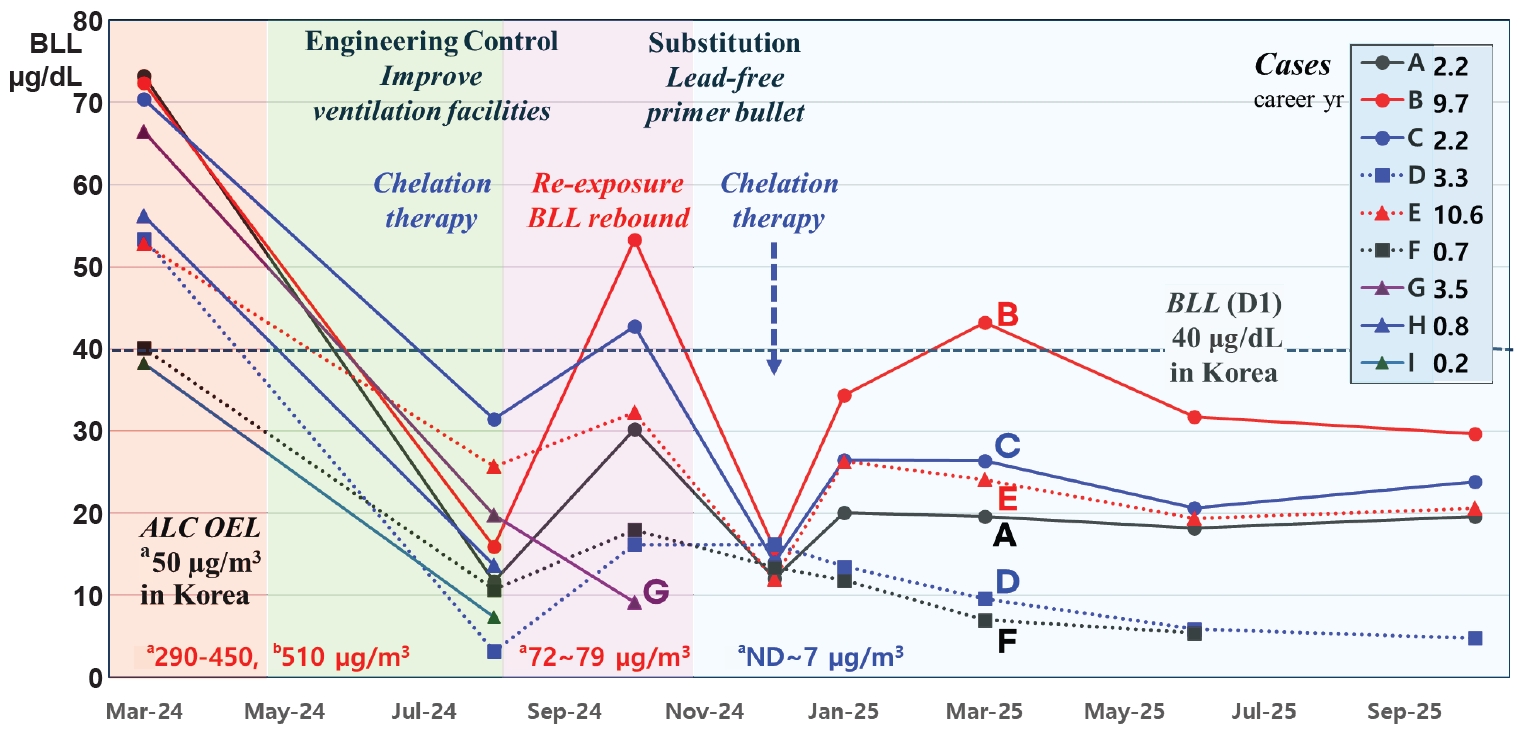
Implementation of the hierarchy of controls and longitudinal trends in lead metrics. This figure illustrates the efficacy of the hierarchy of controls. Engineering controls (improved ventilation) failed to sufficiently lower ALC, whereas substitution with encapsulated ammunition (copper-jacketed, lead-free primer) successfully eliminated the hazard. Corresponding BLLs show distinct patterns: Case B (long tenure) exhibits a “rebound” despite chelation, suggesting mobilization of bone-stored lead, contrasting with case E (managerial role). High initial BLLs in short-tenure cases F, H, and I confirm that BLL reflects intense recent exposure. ALC: airborne lead concentration; BLL: blood lead level; OEL: occupational exposure limit; ND: not detected; D1: diagnosis requiring active medical management under the Korean Special Health Examination system. aPersonal sampling; bArea sampling.
Table 1.
Occupational exposure limits for ALC and biological exposure indices for BLLs in selected countries
In Korea, C1 (occupational): concerns about the progression to an occupational disease. requires follow-up, D1 (occupational): confirmed findings of an occupational disease. requires treatment and work adjustment.
ALC: airborne lead concentration; BLL: blood lead level; TWA: time-weighted average; EU: European Union; BLV: biological limit value; OSHA: Occupational Safety and Health Administration; CFR: Code of Federal Regulations; Cal/OSHA: California Division of Occupational Safety and Health; PEL: permissible exposure limit; NIOSH: National Institute for Occupational Safety and Health; REL: recommended exposure limit; ACGIH: American Conference of Governmental Industrial Hygienists; TLV-TWA: threshold limit value–time-weighted average; BEI: biological exposure index; ACOEM: American College of Occupational and Environmental Medicine; JSOH: Japan Society for Occupational Health.
Table 2.
Demographic characteristics and longitudinal changes in airborne and BLLs
| Cases | Age (years) | Working period (years) | ALC (mg/m3)a | BLL (µg/dL) | Initial symptoms | Chelation frequency total (pre/posta) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mar 2024b | Oct 2024c | Nov 2024 | Dec 2024d | Jan 2025e | Mar 2024b | Aug 2024f | Oct 2024c | Jan 2025e | Jun 2025e | Oct 2025e | |||||
| A | 37 | 2.2 | 0.003 | 73.2 | 11.7 | 30.2 | 18.4 | 18.2 | 16.9 | Chronic headache fatigue | 6 (5/1) | ||||
| B | 39 | 9.7 | 0.079 | ND | 72.4 | 15.9 | 53.3 | 13.5 | 31.7 | 29.7 | Recurrent abdominal pain, diarrhea, headache, intermittent finger twitching | 9 (4/5) | |||
| C | 29 | 2.2 | 0.072 | 0.007 | 0.003 | 0.007 | 70.4 | 31.5 | 42.8 | 23.1 | 20.6 | 23.8 | Chronic headache, Indigestion | 6 (4/2) | |
| D | 42 | 3.3 | 53.4 | 3.2 | 16.2 | 7.3 | 5.9 | 4.8 | Intermittent finger twitching | 6 (6/0) | |||||
| E | 53 | 10.6 | 0.29 | 52.8 | 25.7 | 32.3 | 19.7 | 19.4 | 20.6 | Intermittent finger twitching | 4 (1/3) | ||||
| F | 30 | 0.7 | 0.073 | 0.002 | 0.001 | 40.1 | 10.7 | 18.0 | 4.9 | 5.3 | 3.4 | Chronic headache | 3 (3/0) | ||
| G | 34 | 3.5 | 66.5 | 19.8 | g | Abdominal pain, chronic fatigue | 6 (6/0) | ||||||||
| H | 27 | 0.8 | 56.2 | 13.7 | g | 9.2 | Nonspecific | 2 (2/0) | |||||||
| I | 20 | 0.2 | 0.45 | 38.2 | 7.4 | g | Nonspecific | 1 (1/0) | |||||||
Ventilation intervention in August 2024, the area sample value of ALC in March 2024 is 0.51 mg/m3.
ALC: airborne lead concentration; BLL: blood lead level; ND: non-detect.
aKorea occupational exposure limit (OEL) by personal sampling is 0.05 mg/m3 (50 µg/m3);
bAt the time of the first inspection;
cAfter improving the ventilation system and re-exposure to lead fume;
dAfter replacing with lead-free ammunition (so-called eco-friendly ammunition);
eFollow-up results show the effects of lead stored in bones, especially in cases B and E;
fJust before returning to work after chelation therapy;
gResignation in September 2024.
- 1. Olufemi AC, Mji A, Mukhola MS. Potential health risks of lead exposure from early life through later life: implications for public health education. Int J Environ Res Public Health 2022;19(23):16006.ArticlePubMedPMC
- 2. National Toxicology Program. NTP monograph on health effects of low-level lead. https://ntp.niehs.nih.gov/research/assessments/noncancer/completed/lead. Updated 2011. Accessed December 20, 2025.
- 3. Collin MS, Venkatraman SK, Vijayakumar N, Kanimozhi V, Arbaaz SM, Stacey RG, et al. Bioaccumulation of lead (Pb) and its effects on human: a review. J Hazard Mater Adv 2022;7:100094.Article
- 4. European Parliament, Council of the European Union. Proposal for a Directive amending Council Directive 98/24/EC and Directive 2004/37/EC as regards the limit values for lead and its inorganic compounds and diisocyanates. https://eur-lex.europa.eu/eli/dir/2024/869/oj. Updated 2024. Accessed December 20, 2025.
- 5. Cal/OSHA. Title 8, Section 1532.1 (Lead in Construction) and Section 5198 (Lead in General Industry). https://www.dir.ca.gov/title8/1532_1.html. Updated 2014. Accessed December 20, 2025.
- 6. Laidlaw MA, Filippelli G, Mielke H, Gulson B, Ball AS. Lead exposure at firing ranges: a review. Environ Health 2017;16(1):34.ArticlePubMedPMCPDF
- 7. Alcock R, Wajrak M, Oosthuizen J. Assessment of the effectiveness of ventilation controls in managing airborne and surface lead levels at a newly commissioned indoor shooting range. Int J Environ Res Public Health 2022;19(18):11711.ArticlePubMedPMC
- 8. Vandebroek E, Haufroid V, Smolders E, Hons L, Nemery B. Occupational exposure to metals in shooting ranges: a biomonitoring study. Saf Health Work 2019;10(1):87–94.ArticlePubMedPMC
- 9. Ministry of Government Legislation. Occupational Safety and Health Act, Article 130 (Special health examinations). https://www.law.go.kr/LSW/eng/engMain.do. Updated 2025. Accessed December 20, 2025.
- 10. Koh DH, Choi S, Park JH, Lee SG, Kim HC, Kim I, et al. Evaluation of temporal trends of lead exposure in Korean workers using workplace monitoring data. J Korean Med Sci 2023;38(34):e271.ArticlePubMedPMCPDF
- 11. Kim JH, Kim EA, Koh DH, Byun K, Ryu HW, Lee SG. Blood lead levels of Korean lead workers in 2003-2011. Ann Occup Environ Med 2014;26:30.ArticlePubMedPMCPDF
- 12. Goodfellow HD, Kosonen R. Industrial Ventilation Design Guidebook. Vol. 1. Fundamentals. Boston, MA: Academic Press; 2020.
- 13. Melendez J, Reilly D, Duran C. Numerical investigation of ventilation efficiency in a Combat Arms training facility using computational fluid dynamics modelling. Build Environ 2021;188:107404.Article
- 14. Barsan ME, Boeniger MF, Crouch KG, Esswein EJ, Kardous CA, Khan A, et al. Preventing Occupational Exposures to Lead and Noise at Indoor Firing Ranges. Atlanta, GA: Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health; 2009.
- 15. Grabinski CM, Methner MM, Jackson JM, Moore AL, Flory LE, Tilly T, et al. Characterization of exposure to byproducts from firing lead-free frangible ammunition in an enclosed, ventilated firing range. J Occup Environ Hyg 2017;14(6):461–72.ArticlePubMed
- 16. Weber AK, Bannon DI, Abraham JH, Seymour RB, Passman PH, Lilley PH, et al. Reduction in lead exposures with lead-free ammunition in an advanced urban assault course. J Occup Environ Hyg 2020;17(11-12):598–610.ArticlePubMed
- 17. Morris GA, Cannady R. Proper use of the hierarchy of controls. Prof Saf 2019;64(08):37–40.
- 18. Ajslev JZ, Moller JL, Andersen MF, Pirzadeh P, Lingard H. The hierarchy of controls as an approach to visualize the impact of occupational safety and health coordination. Int J Environ Res Public Health 2022;19(5):2731.ArticlePubMedPMC
- 19. Rabinowitz MB. Toxicokinetics of bone lead. Environ Health Perspect 1991;91:33–7.ArticlePubMedPMC
- 20. Barbosa F, Tanus-Santos JE, Gerlach RF, Parsons PJ. A critical review of biomarkers used for monitoring human exposure to lead: advantages, limitations, and future needs. Environ Health Perspect 2005;113(12):1669–74.ArticlePubMedPMC
- 21. Wedeen R, Goldman R, Headapohl D, Hipkins K, Hu H, Kosnett M, et al. Medical Management Guidelines for Lead-Exposed Adults. CSTE Medical Management Guidelines Added October 2013. Washington, DC: Association of Occupational and Environmental Clinics; 2007.PDF
- 22. Rogan WJ, Dietrich KN, Ware JH, Dockery DW, Salganik M, Radcliffe J, et al. The effect of chelation therapy with succimer on neuropsychological development in children exposed to lead. N Engl J Med 2001;344(19):1421–6.ArticlePubMed
- 23. Dietrich KN, Ware JH, Salganik M, Radcliffe J, Rogan WJ, Rhoads GG, et al. Effect of chelation therapy on the neuropsychological and behavioral development of lead-exposed children after school entry. Pediatrics 2004;114(1):19–26.ArticlePubMedPDF
- 24. McKay CA Jr. Role of chelation in the treatment of lead poisoning: discussion of the Treatment of Lead-Exposed Children Trial (TLC). J Med Toxicol 2013;9(4):339–43.ArticlePubMedPMCPDF
- 25. Sears ME. Chelation: harnessing and enhancing heavy metal detoxification--a review. ScientificWorldJournal 2013;2013:219840.ArticlePubMedPMCPDF
- 26. KOSIS. Results of the Korean National Environmental Health Survey (KoNEHS). https://kosis.kr/eng/. Updated 2025. Accessed December 20, 2025.
- 27. Specht AJ, Lin Y, Xu J, Dickerson AS, Yan C, Hu H, et al. The effect of chelation on bone Pb stores in Pb poisoned children. J Expo Sci Environ Epidemiol 2025;35(5):709–14.ArticlePubMedPMCPDF
- 28. Lee BK. Occupational health management in the lead industry: the Korean experience. Saf Health Work 2011;2(2):87–96.ArticlePubMedPMC
- 29. Park WJ, Lee SH, Lee SH, Yoon HS, Moon JD. Occupational lead exposure from indoor firing ranges in Korea. J Korean Med Sci 2016;31(4):497–501.ArticlePubMedPMCPDF
- 30. Tong S, von Schirnding YE, Prapamontol T. Environmental lead exposure: a public health problem of global dimensions. Bull World Health Organ 2000;78(9):1068–77.PubMedPMC
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteCase series: from ventilation failure to substitution success in occupational lead poisoning at a Korean indoor firing range
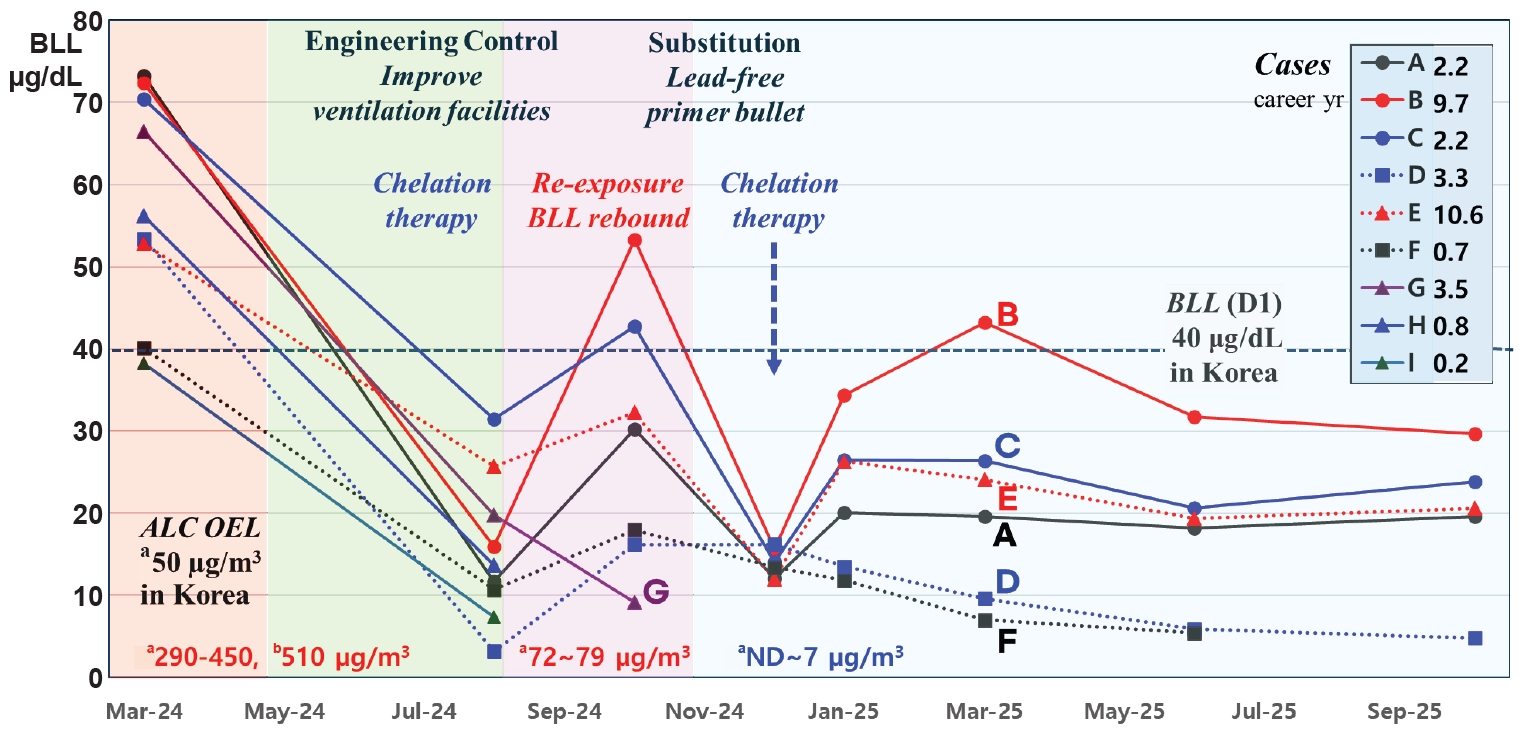
Fig. 1. Implementation of the hierarchy of controls and longitudinal trends in lead metrics. This figure illustrates the efficacy of the hierarchy of controls. Engineering controls (improved ventilation) failed to sufficiently lower ALC, whereas substitution with encapsulated ammunition (copper-jacketed, lead-free primer) successfully eliminated the hazard. Corresponding BLLs show distinct patterns: Case B (long tenure) exhibits a “rebound” despite chelation, suggesting mobilization of bone-stored lead, contrasting with case E (managerial role). High initial BLLs in short-tenure cases F, H, and I confirm that BLL reflects intense recent exposure. ALC: airborne lead concentration; BLL: blood lead level; OEL: occupational exposure limit; ND: not detected; D1: diagnosis requiring active medical management under the Korean Special Health Examination system. aPersonal sampling; bArea sampling.
Fig. 1.
Case series: from ventilation failure to substitution success in occupational lead poisoning at a Korean indoor firing range
| Country/authority | ALC mg/m3 (8-hour TWA) | BLL (µg/dL) | Regulatory status | Actions upon exceedance and remarks |
|---|---|---|---|---|
| Korea | 0.05 | Special health exam guideline 30 (C1)/40 (D1) | Legally binding (Occupational Safety and Health Act) | Diagnosis and follow-up: If BLL ≥30, health exam interval shortened (6→3 months) |
| Job transfer or work restriction required if diagnosed as an occupational disease sufferer (D1) | ||||
| EU | 0.03 | 15 (from 2029), 30 (transitional until the end of 2028) | Legally binding (Directive 2024/869) | Medical surveillance mandatory if air >0.015 mg/m3 or BLL >9 µg/dL |
| Transitional BLV 30 µg/dL until December 31, 2028 | ||||
| USA | ||||
| OSHA | 0.05 | ≥60 (general), ≥50 (construction) | Legally binding (29 CFR 1910.1025) | Medical removal mandatory if BLL ≥60 (or average ≥50) |
| Return permitted when BLL<40, Action Level 0.03 mg/m3 | ||||
| Cal/OSHA | 0.01 | 30 (single), 20 (chronic) | Legally binding (Title 8 §1532.1) | Effective Jan 1, 2025: PEL tightened to 0.01 mg/m3 |
| Medical removal if single BLL ≥30 or last two ≥20 | ||||
| Return when BLL <15 | ||||
| NIOSH | 0.05 REL | <5 recommended goal | Advisory | Goal: recommends maintaining adult BLL <5 µg/dL; emphasizes minimization despite REL of 0.05 |
| ACGIH | 0.05 TLV-TWA | 20 (BEI) | Advisory | Note: carcinogenicity A3 (confirmed animal carcinogen) |
| BEI set at 20 µg/dL to prevent neurobehavioral effects | ||||
| ACOEM | Not specified health-based guidance | <20 action level <10 preferred target | Advisory (professional guideline) | Clinical and preventive guidance: removal from further exposure recommended when BLL ≥20 µg/dL; enhanced surveillance and exposure reduction advised at lower levels. emphasizes that no safe BLL has been identified and advocates primary prevention and minimization of exposure |
| Japan Government | 0.05 Control Level | 40 control class 3 | Legally binding (lead poisoning prevention rule) | Work environment management; if control level exceeded (class 3), facility improvements and respiratory protection mandatory |
| JSOH | 0.03 | 15 reference value | Advisory | Technical recommendation: stricter than government standards based on evidence preventing reproductive toxicity |
| China | 0.05 (dust), 0.03 (fume) | 40 diagnostic criteria | Legally binding (GBZ 2.1/GBZ 37) | Diagnosis: Per GBZ 37-2015, BLL ≥400 µg/L (40 µg/dL) triggers observation or diagnosis requiring action |
| Cases | Age (years) | Working period (years) | ALC (mg/m3) |
BLL (µg/dL) | Initial symptoms | Chelation frequency total (pre/post |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mar 2024 |
Oct 2024 |
Nov 2024 | Dec 2024 |
Jan 2025 |
Mar 2024 |
Aug 2024 |
Oct 2024 |
Jan 2025 |
Jun 2025 |
Oct 2025 |
|||||
| A | 37 | 2.2 | 0.003 | 73.2 | 11.7 | 30.2 | 18.4 | 18.2 | 16.9 | Chronic headache fatigue | 6 (5/1) | ||||
| B | 39 | 9.7 | 0.079 | ND | 72.4 | 15.9 | 53.3 | 13.5 | 31.7 | 29.7 | Recurrent abdominal pain, diarrhea, headache, intermittent finger twitching | 9 (4/5) | |||
| C | 29 | 2.2 | 0.072 | 0.007 | 0.003 | 0.007 | 70.4 | 31.5 | 42.8 | 23.1 | 20.6 | 23.8 | Chronic headache, Indigestion | 6 (4/2) | |
| D | 42 | 3.3 | 53.4 | 3.2 | 16.2 | 7.3 | 5.9 | 4.8 | Intermittent finger twitching | 6 (6/0) | |||||
| E | 53 | 10.6 | 0.29 | 52.8 | 25.7 | 32.3 | 19.7 | 19.4 | 20.6 | Intermittent finger twitching | 4 (1/3) | ||||
| F | 30 | 0.7 | 0.073 | 0.002 | 0.001 | 40.1 | 10.7 | 18.0 | 4.9 | 5.3 | 3.4 | Chronic headache | 3 (3/0) | ||
| G | 34 | 3.5 | 66.5 | 19.8 | Abdominal pain, chronic fatigue | 6 (6/0) | |||||||||
| H | 27 | 0.8 | 56.2 | 13.7 | 9.2 | Nonspecific | 2 (2/0) | ||||||||
| I | 20 | 0.2 | 0.45 | 38.2 | 7.4 | Nonspecific | 1 (1/0) | ||||||||
Table 1. Occupational exposure limits for ALC and biological exposure indices for BLLs in selected countries
In Korea, C1 (occupational): concerns about the progression to an occupational disease. requires follow-up, D1 (occupational): confirmed findings of an occupational disease. requires treatment and work adjustment. ALC: airborne lead concentration; BLL: blood lead level; TWA: time-weighted average; EU: European Union; BLV: biological limit value; OSHA: Occupational Safety and Health Administration; CFR: Code of Federal Regulations; Cal/OSHA: California Division of Occupational Safety and Health; PEL: permissible exposure limit; NIOSH: National Institute for Occupational Safety and Health; REL: recommended exposure limit; ACGIH: American Conference of Governmental Industrial Hygienists; TLV-TWA: threshold limit value–time-weighted average; BEI: biological exposure index; ACOEM: American College of Occupational and Environmental Medicine; JSOH: Japan Society for Occupational Health.
Table 2. Demographic characteristics and longitudinal changes in airborne and BLLs
Ventilation intervention in August 2024, the area sample value of ALC in March 2024 is 0.51 mg/m3. ALC: airborne lead concentration; BLL: blood lead level; ND: non-detect. Korea occupational exposure limit (OEL) by personal sampling is 0.05 mg/m3 (50 µg/m3); At the time of the first inspection; After improving the ventilation system and re-exposure to lead fume; After replacing with lead-free ammunition (so-called eco-friendly ammunition); Follow-up results show the effects of lead stored in bones, especially in cases B and E; Just before returning to work after chelation therapy; Resignation in September 2024.

