
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 36; 2024 > Article
- Original Article The risk of insomnia by work schedule instability in Korean firefighters
-
Saebomi Jeong1
 , Jeonghun Kim1, Sung-Soo Oh1, Hee-Tae Kang1, Yeon-Soon Ahn2,*, Kyoung Sook Jeong1,*
, Jeonghun Kim1, Sung-Soo Oh1, Hee-Tae Kang1, Yeon-Soon Ahn2,*, Kyoung Sook Jeong1,* -
Annals of Occupational and Environmental Medicine 2024;36:e24.
DOI: https://doi.org/10.35371/aoem.2024.36.e24
Published online: September 10, 2024
1Department of Occupational and Environmental Medicine, Wonju Severance Christian Hospital, Wonju College of Medicine, Yonsei University, Wonju, Korea
2Department of Preventive Medicine, Wonju College of Medicine, Yonsei University, Wonju, Korea
- *Correspondence: Kyoung Sook Jeong Department of Occupational and Environmental Medicine, Wonju Severance Christian Hospital, Wonju College of Medicine, Yonsei University, 20 Ilsan-ro, Wonju 26426, Korea E-mail: jeongks@yonsei.ac.kr
- *Yeon-Soon Ahn Department of Preventive Medicine, Wonju College of Medicine, Yonsei University, 20 Ilsan-ro, Wonju 26426, Korea E-mail: ysahn1203@gmail.com
• Received: May 16, 2024 • Revised: August 5, 2024 • Accepted: August 7, 2024
© 2024 Korean Society of Occupational & Environmental Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background Firefighters are exposed to shift work, as well as unpredictable emergency calls and traumatic events, which can lead to sleep problems. This study aimed to investigate the risk of insomnia by work schedule instability in Korean firefighters.
-
Methods This study used the Insomnia Severity Index to assess the insomnia in firefighters. The work schedule stability was classified with the frequency of the substitute work and the timing of notification for work schedule changes. Logistic regression analysis was used to assess the adjusted odds ratio of insomnia by work schedule stability with covariates including sex, age, education, smoking, alcohol, caffeine intake, shift type, job, and underlying conditions.
-
Results Of the 8,587 individuals, 751 (8.75%) had moderate to severe insomnia (Insomnia Severity Index ≥ 15). The prevalence of insomnia was statistically significantly higher as the frequency of substitute work increased: <1 time per month (6.8%), 1–2 times (9.5%), 3–5 times (13.4%), and more than 5 times (15.7%) (p < 0.001). Additionally, the prevalence of insomnia was statistically significantly higher when the timing of the schedule change notification was urgent or irregular: no change or several weeks before (5.4%), several days before (7.9%), one day before or on the day (11.2%), irregularly notification (11.6%) (p < 0.001). In comparison to the group with good frequency of the substitute work/good timing of schedule change notification group, the adjusted odds ratios of insomnia were 1.480 (95% confidence interval [CI]: 1.237–1.771) for Good/Bad group, 1.862 (95% CI: 1.340–2.588) for Bad/Good group, and 1.885 (95% CI: 1.366–2.602) for Bad/Bad group.
-
Conclusions Work schedule instability was important risk factor of insomnia in firefighters. It suggests that improving the stability of work schedules could be a key strategy for reducing sleep problems in this occupational group.
BACKGROUND
Sleep is critical for both mental and physical health. Insomnia, which has been linked to mental disorders and cognitive impairments, predisposes people to various physical health problems all of which are associated with premature mortality.1-3 Sleep disorders caused by shift work increase the risk of cancers, including breast, prostate, and colon cancer.4,5 Additionally, sleep problems also reduce work productivity and are linked to injuries and deaths from vehicle and workplace accidents.6,7
Risk factors for insomnia include female sex, old age, obesity, and physical inactivity, and studies have shown that it is influenced by caffeine intake, smoking, and drinking8-12 In addition, previous studies have shown that insomnia is associated with not only physical diseases such as hypertension, dyslipidemia, heart disease, and skin disease, but also mental diseases such as depression, anxiety, and post-traumatic stress disorder (PTSD).13-17
According to a report from the Korea National Fire Agency, large-scale fires have recently increased, and the number of emergency rescue requests is also increasing.18 Firefighters are faced to the difficult occupational environments, which includes exposure to shift work, psychosocial stressors, and traumatic events that can lead to PTSD.19 The unpredictable emergencies contributes significantly to the risk of sleep disorders among firefighters, as they must remain alert and respond at any time, often disrupting their sleep patterns.20
Unavoidable emergency calls and limited job autonomy with shift work in professions like firefighting have been consistently linked to poor sleep quality, a concern also observed in police officers, military personnel, and medical personnel.21-23 A systematic review and meta-analysis found a 30.49% prevalence of sleep disorders among firefighters, with 51.43% reporting poor sleep quality.24 Factors such as rotating shift patterns, types of job, effort-reward imbalance, traumatic incident exposure, and frequent nighttime emergency calls have association with sleep disorders among firefighters.20,25,26
Despite these findings, research into how the instability of firefighters’ work schedule affects their insomnia is limited. The objective of this study is to investigate the association between work schedule instability and insomnia among Korean firefighters. Especially, Korean firefighters have been exposed with frequent changes of work schedules. By identifying work schedule instability that is detrimental to sleep disorders, this study aims to inform the factors that may contribute to these negative health outcomes and ultimately improve health and well-being in firefighter organizations.
METHODS
The survey was conducted to investigate the firefighting activity system in Korean firefighters and to improve it through changes in the firefighting environment. From November 2017 to August 2018, data were collected from firefighters across Korea through an online survey conducted.20 Of the 48,042 Korean firefighters, 9,810 responded to the survey, resulting in a response rate of approximately 20.42%. Out of the initial 9,810 participants, 8,587 individuals were finally included, after excluding 157 participants due to missing data, 87 who were currently taking sleeping pills, and 979 who only worked daytime (Fig. 1).
For sleep assessment, the Korean version of the Insomnia Severity Index (ISI) was used. 27 The ISI is a short subjective questionnaire with seven items that assess the severity of difficulty initiating sleep, the severity of difficulty maintaining sleep, the severity of difficulty waking up, sleep satisfaction, interference with daytime functioning, the noticeability of sleep problems to others, and the level of worry caused by insomnia. In this study, no insomnia or a mild level of insomnia (ISI score <15) was classified as not having insomnia, while moderate to severe insomnia (ISI score ≥15) was classified as having insomnia.27
To investigate the work schedule instability in firefighters who work shifts, questionnaires were distributed that asked monthly days of substitute work and timing of notification for work schedule changes. The survey asked, “How often do you have to do substitute work due to manpower vacuum?” Participants chose one of <1, 1–2, 3–5, or >5 (numbers/month). And the survey asked, “If the established work schedule has to be changed at the request of the fire department, when will you be notified of the change in work schedule?”. Participants selected one of the following answers: no change in schedule change, several weeks before, several days before, one day before, on the day, or irregularly notification, and then participants divided into four groups as no change in schedule or several weeks before, several days before, one day before or on the day, and irregularly notification.28
Furthermore, participants were divided into four groups based on their monthly number of substitute work and the timing of schedule change notifications. Working less than 3 days of substitute work per month was classified as Good while working 3 days or more of substitute work per month was classified as Bad. If there were no changes to the work schedule or if notification was given several weeks or days in advance, the timing of schedule change notification was classified as Good. If a change in working hours was announced one day in advance, on the same day, or irregularly, the timing of schedule change notification was classified as Bad. Finally, the work schedule stability was divided into four groups, Good/Good, Good/Bad, Bad/Good, and Bad/Bad (Fig. 1).
The variables investigated in the study included a wide range of demographic, physical, psychosocial, and work-related factors, each carefully selected to shed light on the multifaceted nature of the participants’ lives and the association with health outcomes, particularly insomnia.
The demographic data were collected including age, sex, body mass index (BMI), education, marital status, monthly income, smoking status, alcohol consumption, caffeine intake, and exercise. The obesity was classified with BMI by two groups: <25 (normal) or ≥25 kg/m2 (obese). Alcohol consumption, caffeine intake, and exercise variables were divided into two groups: yes or no.
The physical health question asked whether they had been diagnosed with the disease by a doctor. Mental health conditions including depression, anxiety, and PTSD were assessed with the Patient Health Questionnaire-9 (PHQ-9), Generalized Anxiety Disorder-7 (GAD-7), and the Primary Care-PTSD screen (PC-PTSD), respectively.29-31 In the analysis, a total score of less than 5 was classified as no depressive or anxiety symptoms, and a total score of 5 or more was classified as the presence of symptoms.29,30
Work-related characteristics were also thoroughly examined to identify the occupational hazards and challenges that firefighters face. The classification of job types reflected the various roles in the firefighting profession, each with its own set of demands and stressors. The shift work patterns in Korean firefighters, who were the subjects of the study, were typically 3, 6, 9, and 21 cycles.32
The chi-square test or t-test was used to compare the prevalence of insomnia by demographic or socioeconomic characteristics or psychosocial symptoms.
Logistic regression analysis was used to investigate the risk of insomnia by work schedule instability. Confounding variables included general variables as well as physical factors, psychosocial factors and work-related variables. To show the odds ratio (OR) of insomnia for work schedule instability after excluding effects of confounding variables, we analyzed the ORs adjusted for confounding variables step by step. We calculated overall crude and adjusted ORs including Model 1, which adjusted for sex and age group; Model 2, which further adjusted for education level, smoking status, alcohol consumption, caffeine intake, exercise, hypertension, dyslipidemia, cardiac disease, skin disease, and depressive symptoms; and Model 3, which further adjusted for shift type and job. Marital status and monthly income, which have a high correlation with age, and anxiety symptoms and PTSD symptoms, which have a high correlation with depressive symptoms, were excluded as confounding variables due to the multicollinearity.
The statistical procedures were executed using the IBM SPSS Statics version 26.0 (IBM Corp., Armonk, NY, USA), with a p-value of less than 0.05 indicating statistical significance.
This study was granted ethical approval from the Institutional Review Board of Yonsei University Wonju Severance Christian Hospital (approval number: CR318031).
RESULTS
The general characteristics of the study population are summarized in Table 1. The prevalence of insomnia in all participants was 8.75%. The composition of the study participants was predominantly male, accounting for 93.8%. The most represented age group was individuals in their 30s, comprising 41.6% of the participants. The mean age of the subjects was 39.1 years with a standard deviation of 8.50. The prevalence of insomnia was significantly higher in female (11.5%) and married group (9.4%) than male (8.6%) and single group (7.3%). The prevalence of insomnia significantly increased with age and monthly income. In the group with current smoking, alcohol drinking, caffeine intake and exercise, the prevalence of insomnia was significantly lower than in the group without them. There was no significant difference in the prevalence of insomnia by BMI and education level.
Participants with underlying diseases and psychological symptoms including hypertension, dyslipidemia, cardiac disease, skin disease, depressive symptoms, anxiety symptoms, and PTSD symptoms had a higher prevalence of insomnia compared to those without these conditions (p < 0.001) (Table 2).
Work-related variables including job type, monthly number of substitute work, and timing of schedule change notifications, were significantly associated with insomnia. There is no significant difference in the prevalence of insomnia by type of shift. By job, the prevalence of insomnia was notably higher among those in fire investigation, fire suppression and emergency medical services compared to administration, rescue, and other roles (p = 0.014).
The prevalence of insomnia was statistically significantly higher as the frequency of substitute work increased: <1 time per month (6.8%), 1–2 times (9.5%), 3–5 times (13.4%), and more than 5 times (15.7%) (p < 0.001). Additionally, the prevalence of insomnia was statistically significantly higher when the timing of the schedule change notification was urgent or irregular: no change or several weeks before (5.4%), several days before (7.9%), one day before or on the day (11.2%), irregularly notification (11.6%) (p < 0.001).
By work schedule stability, the Good/Good group had the lowest prevalence of insomnia (6.3%), while Good/Bad group (10.6%), Bad/Good group (13.0%), and the Bad/Bad group (14.7%) had the higher prevalence (p < 0.001) (Table 3).
Table 4 shows the ORs for insomnia by work schedule instability based on work-related factors, including a comparison to the frequency of monthly substitute work and timing of notification for schedule change. When compared to the group with less than one substitute work per month, the adjusted odds ratios for groups with 1–2, 3–5, and more than 5 substitute work were 1.327 (95% confidence interval [CI]: 1.103–1.597), 1.794 (95% CI: 1.355–2.375), and 1.823 (95% CI: 1.142–2.910) respectively. By the timing of notification for schedule change compared to the group with no changes or notifications several weeks in advance, the adjusted odds ratios for experiencing insomnia were 1.448 (95% CI: 1.130–1.855) for those notified several days before, 1.719 (95% CI: 1.320–2.238) for those notified a day before or on the day, and 1.816 (95% CI: 1.410–2.338) for those with irregular notifications.
By work schedule stability, the adjusted odds ratios for insomnia compared to the Good/Good reference group were 1.480 (95% CI: 1.237–1.771) for Good/Bad, 1.862 (95% CI: 1.340–2.588) for Bad/Good, and 1.885 (95% CI: 1.366–2.602) for Bad/Bad, indicating a significant increase in the risk for insomnia based on these work-related dynamics.
DISCUSSION
This study focused on the association between insomnia and work schedule instability based on frequency of monthly substitute work and the timing of the work schedule change notification in the shift-working firefighter. The odds ratio of insomnia was higher when the number of monthly overtime hours was greater and work schedule changes were notified late or irregularly. This association persisted for work schedule instability.
In this study, 751 (8.75%) reported moderate to severe insomnia among the participants. This prevalence was higher compared to a previous study on Korean pre-employed firefighters, where insomnia rates were 3.2% for those in their 20s and 4.5% for those in their 30s.33 Previous studies had shown that insomnia prevalence among firefighters can vary significantly, ranging from 4% to 61%, depending on factors such as sex, age, nationality, and the method of assessing insomnia.24
In our study, as in previous studies, the prevalence of insomnia was found to be high in female, older age groups, no exercising group, and who with underlying physical and mental diseases.8,9,12-14,16,17 Unlike previous studies, the prevalence of insomnia was high in married, high-income, current smoker, alcohol drinker, caffeine consumer.11,12 This was because the nature of the factor differed depending on the age groups of the subjects in our study.
In our study, we additionally stratified by age group and examined the association between work schedule instability and insomnia (Supplementary Table 1). The results of this association analysis were consistent across all age groups. In particular, when work schedule stability was bad in group in their 30s, which accounts for the largest proportion of our study subjects, the odd ratio was larger and the risk of insomnia was found to increase further. This suggests that work schedule instability may have a greater impact on insomnia in people in their 30s, and may also be related to work-family balance, so further study is needed.34 In those in their 20s, the timing of work schedule change notification was an important factor. In those in their 50s, the number of substitute work was an important factor in insomnia which suggests that older group may be more affected by frequency due to their decline in physical strength.35 In our subgroup analysis by sex, the association between work schedule instability and insomnia was observed to be consistent with the overall findings, with broader confidence intervals observed in the female group compared to the male group (Supplementary Table 2).
Prior studies in occupational health have primarily focused on the association with work schedules and sleep quality, emphasizing the negative effects of irregular work schedules on overall sleep health. Previous research has highlighted the negative effects changing in working schedule has on health outcomes.36 Geiger-Brown et al.37 reported that work schedule instability of nurse group was mainly investigated the frequency of overtime hours or early return to work. This study significantly improves our understanding of the complex relationship between work schedule instability and insomnia in firefighters, providing critical insights into the field of occupational health.38 Although it is challenging to eliminate the shift work environment for firefighters, managing sleep among firefighters might be feasible by controlling and enhancing the stability of their work schedules.
There are several previous studies that have addressed the physiological mechanisms related to sleep in shift workers. Circadian rhythms are important in regulating human physiology and behavior, but shift work can disrupt the circadian oscillation of sleep and wakefulness.39 Chronic sleep deprivation can affect the sympathetic nervous system and cause increased activity in the hypothalamic-pituitary-adrenal axis.40 The relationship between the activation of these stress systems and sleep deprivation is bidirectional, with sleep loss affecting sensitivity to stress stimuli.40,41 The shift work environment of firefighters makes them more vulnerable to insomnia, and additionally, if they have to alternative substitute work due to manpower vacancies, it can further adversely affect their sleep. In this regard, further study on physiological responses to work instability will be needed.
And also, our analysis indicates a potential interaction between the components of work schedule instability—monthly number of substitute work and timing of schedule change notifications. This interaction suggests that the combined effect of these variables on insomnia may be greater than the sum of their individual effects. One plausible mechanism is that frequent schedule changes, coupled with short notice periods, may exacerbate the disruption of circadian rhythms, leading to more severe sleep disturbances. Future studies should include explicit interaction terms in the model to better understand these dynamics and validate our findings.
This study has several limitations that should be addressed. First, the cross-sectional design limits our ability to determine causality between insomnia and work schedule instability. Second, relying on survey data increases the possibility of recall bias. Third, the assessment of work schedule instability was based on subjective evaluations, which may not accurately reflect the objective nature of work schedules. Fourth, the study subjects were not randomly selected but participated voluntarily. Voluntary participation could lead to selection bias, as those who chose to participate might have different characteristics, such as being more health-conscious or having more pronounced sleep issues, compared to those who did not participate. This limitation should be taken into account when interpreting the results and generalizing the findings to the broader population of firefighters. Fifth, setting the cutoff for PHQ-9 and GAD-7 at 5 points may not effectively capture mild symptoms of depression and anxiety in this generally healthy firefighter population, potentially resulting in a skewed distribution of scores.
Despite these limitations, this study’s main strength is its focused examination of the association work schedule instability with sleep health among firefighters. The clear demonstration of the negative impact of low stability on sleep emphasizes the critical need for interventions tailored to this issue. Strategies such as creating more consistent work schedules and improving communication about schedule changes, as suggested by the recommendations of Billings and Focht,42 could be beneficial. Furthermore, the findings of this study have broader implications, emphasizing the importance of sleep considerations in the occupational health policies of various industries, including medical personnel, soldiers, and police officers. This emphasizes the universal importance of work schedule instability in ensuring the well-being of workers in various fields.
CONCLUSIONS
This study explores the risk of insomnia by work schedule instability in firefighters. By synthesizing these findings with existing literature, we gain a comprehensive understanding of the study’s unique insights. These findings not only inform immediate interventions aimed at improving firefighter well-being but also pave the way for broader discussions about sleep health within the context of occupational health policy-making.
Abbreviations
BMI
body mass index
CI
confidence interval
EMS
emergency medical services
GAD-7
Generalized Anxiety Disorder-7
HPA
hypothalamic-pituitary-adrenal
ISI
Insomnia Severity Index
OR
odds ratio
PC-PTSD
Primary Care-PTSD screen
PHQ-9
Patient Health Questionnaire-9
PTSD
post-traumatic stress disorder
-
Competing interests
Sung-Soo Oh, Yeon-Soon Ahn, and Kyoung Sook Jeong contributing editors of the Annals of Occupational and Environmental Medicine, were not involved in the editorial evaluation or decision to publish this article. All remaining authors have declared no conflicts of interest.
-
Author contributions
Conceptualization: Ahn YS, Jeong KS. Data curation: Jeong S, Kim J. Formal analysis: Ahn YS, Jeong S. Investigation: Ahn YS, Jeong KS. Methodology: Jeong S, Oh SS. Software: Jeong KS. Supervision: Kang HT, Oh SS. Validation: Jeong KS, Ahn YS. Visualization: Jeong S. Writing - original draft: Jeong S. Writing - review & editing: Jeong KS, Ahn YS.
-
Acknowledgments
This research was supported by the Emergency Response to Disaster sites Research and Development Program funded by Korean National Fire Agency (20013968, Korea Evaluation Institute of Industrial Technology, KEIT).
NOTES
SUPPLEMENTARY MATERIAL
Supplementary Table 1.
Odds ratios (95% confidence intervals) of insomnia according to work-related variables in age subgroup analysis
Supplementary Table 2.
Odds ratio (95% confidence intervals) of insomnia according to work-related variables in sex subgroup analysis
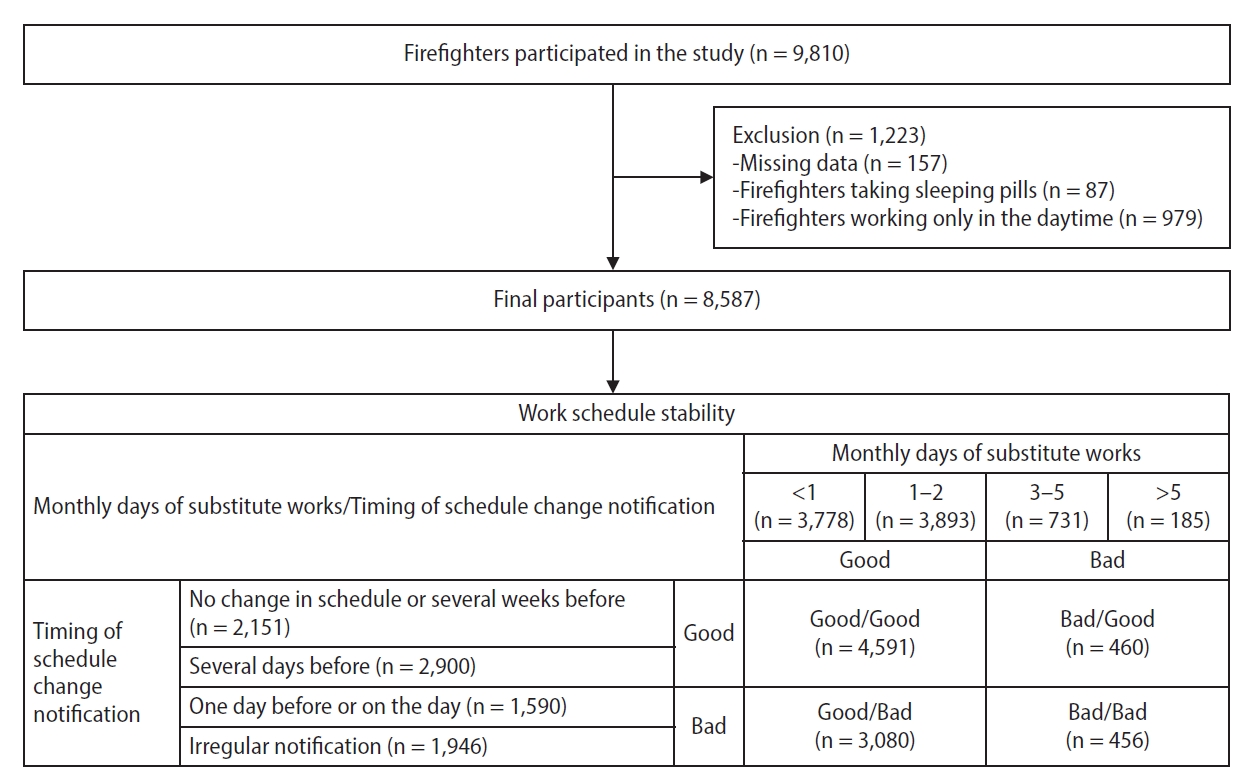
Table 1.
The distribution of participants and prevalence of insomnia by general characteristics
| Variable | Total (n = 8,587) |
Insomniaa |
p-value | |
|---|---|---|---|---|
| No (n = 7,836, 91.25%) | Yes (n = 751, 8.75%) | |||
| Sex | ||||
| Male | 8,056 (93.8) | 7,366 (91.4) | 690 (8.6) | 0.021 |
| Female | 531 (6.2) | 470 (88.5) | 61 (11.5) | |
| Age (years) | ||||
| 20–29 | 1,241 (14.5) | 1,160 (93.5) | 81 (6.5) | 0.003 |
| 30–39 | 3,571 (41.6) | 3,265 (91.4) | 306 (8.6) | |
| 40–49 | 2,497 (29.1) | 2,269 (90.9) | 228 (9.1) | |
| ≥50 | 1,278 (14.9) | 1,142 (89.4) | 136 (10.6) | |
| Mean ± SD | 39.13 ± 8.50 | 39.03 ± 8.50 | 40.25 ± 8.40 | <0.001 |
| BMI (kg/m2) | ||||
| <25 | 5,482 (63.8) | 4,995 (91.1) | 487 (8.9) | 0.548 |
| ≥25 | 3,105 (36.2) | 2,841 (91.5) | 264 (8.5) | |
| Mean ± SD | 24.27 ± 2.51 | 24.27 ± 2.50 | 24.23 ± 2.67 | 0.631 |
| Education | ||||
| High school | 1,873 (21.8) | 1,716 (91.6) | 157 (8.4) | 0.184 |
| College | 2,720 (31.7) | 2,499 (91.9) | 221 (8.1) | |
| ≥University | 3,994 (46.5) | 3,621 (90.7) | 373 (9.3) | |
| Marital status | ||||
| Single | 2,691 (31.3) | 2,494 (92.7) | 197 (7.3) | 0.002 |
| Married | 5,896 (68.7) | 5,342 (90.6) | 554 (9.4) | |
| Monthly income (×1,000 KRW) | ||||
| 2,000–2,999 | 3,127 (36.4) | 2,895 (92.6) | 232 (7.4) | 0.003 |
| 3,000–4,999 | 4,195 (48.9) | 3,805 (90.7) | 390 (9.3) | |
| ≥5,000 | 1,265 (14.7) | 1,136 (89.8) | 129 (10.2) | |
| Smoking status | ||||
| Never smoker | 3,218 (37.5) | 2,918 (90.7) | 300 (9.3) | 0.047 |
| Ex-smoker | 2,934 (34.2) | 2,667 (90.9) | 267 (9.1) | |
| Current smoker | 2,435 (28.4) | 2,251 (92.4) | 184 (7.6) | |
| Alcohol consumption | ||||
| No | 2,356 (27.4) | 2,127 (90.3) | 229 (9.7) | 0.049 |
| Yes | 6,231 (72.6) | 5,709 (91.6) | 522 (8.4) | |
| Caffeine intake | ||||
| No | 1,374 (16.0) | 1,227 (89.3) | 147 (10.7) | 0.005 |
| Yes | 7,213 (84.0) | 6,609 (91.6) | 604 (8.4) | |
| Exercise | ||||
| No | 2,741 (31.9) | 2,468 (90.0) | 273 (10.0) | 0.006 |
| Yes | 5,846 (68.1) | 5,368 (91.8) | 478 (8.2) | |
Values are presented as number (%) or mean ± standard error.
SD: standard deviation; BMI: body mass index; KRW: Korean Won; ISI: Insomnia Severity Index.
aInsomnia was classified with No or Yes by ISI score (No: <15; Yes: ≥15);
bCalculated by chi-square test for binomial variables and t-test for numeric variables.
Table 2.
The distribution of participants and prevalence of insomnia by underlying diseases and psychological symptoms
| Variable | Total (n = 8,587) |
Insomniaa |
p-valueb | |
|---|---|---|---|---|
| No (n = 7,836, 91.25%) | Yes (n = 751, 8.75%) | |||
| Hypertension | ||||
| Yes | 779 (9.1) | 661 (84.9) | 118 (15.1) | <0.001 |
| No | 7,808 (90.9) | 7,175 (91.9) | 633 (8.1) | |
| Dyslipidemia | ||||
| Yes | 751 (8.7) | 987 (86.7) | 151 (13.3) | <0.001 |
| No | 7,836 (91.3) | 6,849 (91.9) | 600 (8.1) | |
| Cardiac disease | ||||
| Yes | 177 (2.1) | 138 (78.0) | 39 (22.0) | <0.001 |
| No | 8,410 (97.9) | 7,398 (91.5) | 712 (8.5) | |
| Skin disease | ||||
| Yes | 949 (11.1) | 787 (82.9) | 162 (17.1) | <0.001 |
| No | 7,638 (88.9) | 7,049 (92.3) | 589 (7.7) | |
| Depressive symptomc | ||||
| Yes | 1,454 (16.9) | 982 (67.5) | 472 (32.5) | <0.001 |
| No | 7,133 (83.1) | 6,854 (96.1) | 279 (3.1) | |
| Anxiety symptomd | ||||
| Yes | 981 (11.4) | 614 (62.6) | 367 (37.4) | <0.001 |
| No | 7,606 (88.6) | 7,222 (95.0) | 384 (5.0) | |
| PTSD symptome | ||||
| Yes | 826 (9.6) | 558 (67.6) | 268 (32.4) | <0.001 |
| No | 7,761 (90.4) | 7,278 (93.8) | 483 (6.2) | |
Values are presented as number (%).
PTSD: post-traumatic stress disorder; ISI: Insomnia Severity Index; PHQ-9: Patient Health Questionnaire-9; GAD-7: Generalized Anxiety Disorder-7; PC-PTSD: Primary Care-PTSD screen.
aInsomnia was classified with No or Yes by ISI score (No: <15, Yes: ≥15);
bCalculated by chi-square test;
cDepressive symptom was classified with No or Yes by PHQ-9 score (No: <5, Yes: ≥5);
dAnxiety symptom was classified with No or Yes by GAD-7 score (No: <5, Yes: ≥5);
ePTSD symptom was classified with No or Yes by PC-PTSD (No: <3, Yes: ≥3 items).
Table 3.
The distribution of participants and prevalence of insomnia by work-related variables
| Variable | Total (n = 8,587) |
Insomniaa |
p-valueb | |
|---|---|---|---|---|
| No (n = 7,836, 91.25%) | Yes (n = 751, 8.75%) | |||
| Type of shift | ||||
| 3-Day cycle | 667 (7.8) | 618 (92.7) | 49 (7.3) | 0.552 |
| 6-Day cycle | 156 (1.8) | 140 (89.7) | 16 (10.3) | |
| 9-Day cycle | 1,169 (13.6) | 1,058 (90.5) | 111 (9.5) | |
| 21-Day cycle | 6,215 (72.4) | 5,675 (91.3) | 540 (8.7) | |
| Others | 380 (4.4) | 345 (90.8) | 35 (9.2) | |
| Job | ||||
| Administration | 96 (1.1) | 89 (92.7) | 7 (7.3) | 0.014 |
| Fire suppression | 2,956 (34.4) | 2,684 (90.8) | 272 (9.2) | |
| EMS | 2,496 (29.1) | 2,258 (90.5) | 238 (9.5) | |
| Rescue | 952 (11.1) | 897 (94.2) | 55 (5.8) | |
| Fire investigation | 220 (2.6) | 198 (90.0) | 22 (10.0) | |
| Others | 1,867 (21.7) | 1,710 (91.6) | 157 (8.4) | |
| Monthly number of substitute workc | ||||
| <1 | 3,778 (44.0) | 3,522 (93.2) | 256 (6.8) | <0.001 |
| 1–2 | 3,893 (45.3) | 3,525 (90.2) | 368 (9.5) | |
| 3–5 | 731 (8.5) | 633 (86.6) | 98 (13.4) | |
| >5 | 185 (2.2) | 156 (84.3) | 29 (15.7) | |
| Timing of schedule change notificationd | ||||
| No change or several weeks before | 2,151 (25.0) | 2,034 (94.6) | 117 (5.4) | <0.001 |
| Several days before | 2,900 (33.8) | 2,670 (92.1) | 230 (7.9) | |
| One day before or on the day | 1,590 (18.5) | 1,412 (88.8) | 178 (11.2) | |
| Irregularly notification | 1,946 (22.7) | 1,720 (88.4) | 226 (11.6) | |
| Work schedule stabilitye | ||||
| Good/Good | 4,591 (53.5) | 4,304 (93.7) | 287 (6.3) | <0.001 |
| Good/Bad | 3,080 (35.9) | 2,743 (89.1) | 337 (10.9) | |
| Bad/Good | 460 (5.4) | 400 (87.0) | 60 (13.0) | |
| Bad/Bad | 456 (5.3) | 389 (85.3) | 67 (14.7) |
Values are presented as number (%).
EMS: emergency medical services; ISI: Insomnia Severity Index.
aInsomnia was classified with No or Yes by ISI score (No: <15, Yes: ≥15);
bCalculated by chi-square test;
cMonthly number of substitute works was classified with Good or Bad (Good: monthly number <3; Bad: monthly number ≥3);
dTiming of schedule change notification was classified with Good or Bad (Good: no change or notification several weeks before or several days before; Bad: notification one day before or on the day or irregular notification);
eWork schedule stability was classified by monthly number of substitute work and timing of schedule change notification.
Table 4.
The odds ratios of insomnia by work schedule change
| Crude | Model 1a | Model 2b | Model 3c | |
|---|---|---|---|---|
| Monthly number of substitute workd | ||||
| <1 | 1 (ref.) | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| 1–2 | 1.436 (1.216–1.696) | 1.375 (1.064–1.778) | 1.298 (1.083–1.556) | 1.327 (1.103–1.597) |
| 3–5 | 2.130 (1.663–2.729) | 2.234 (1.741–2.867) | 1.738 (1.320–2.289) | 1.794 (1.355–2.375) |
| >5 | 2.558 (1.687–3.878) | 2.694 (1.773–4.092) | 1.783 (1.121–2.835) | 1.823 (1.142–2.910) |
| Timing of schedule change notificatione | ||||
| No change or several weeks before | 1 (ref.) | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| Several days before | 1.498 (1.190–1.885) | 1.517 (1.205–1.910) | 1.449 (1.132–1.854) | 1.448 (1.130–1.855) |
| One day before or on the day | 2.192 (1.719–2.794) | 2.130 (1.669–2.717) | 1.729 (1.329–2.249) | 1.719 (1.320–2.238) |
| Irregular notification | 2.284 (1.811–2.882) | 2.285 (1.810–2.885) | 1.810 (1.407–2.327) | 1.816 (1.410–2.338) |
| Work schedule stabilityf | ||||
| Good/Good | 1 (ref.) | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| Good/Bad | 1.842 (1.563–2.172) | 1.801 (1.527–2.125) | 1.475 (1.233–1.763) | 1.480 (1.237–1.771) |
| Bad/Good | 2.249 (1.672–3.026) | 2.314 (1.719–3.115) | 1.789 (1.290–2.481) | 1.862 (1.340–2.588) |
| Bad/Bad | 2.583 (1.942–3.436) | 2.609 (1.959–3.473) | 1.851 (1.347–2.544) | 1.885 (1.366–2.602) |
The adjusted odds ratio (95% confidence interval) was calculated via binomial logistic regression analyses.
aModel 1: adjusted for sex and age;
bModel 2: adjusted for all variables in Model 1, body mass index, education, smoking status, alcohol consumption, caffeine intake, exercise, hypertension, dyslipidemia, cardiac disease, skin disease, and depressive symptom;
cModel 3: adjusted for all variables in model 2, shift type, and job;
dMonthly number of substitute work was classified with Good or Bad (Good: monthly number <3; Bad: monthly number ≥3);
eTiming of schedule change notification was classified with Good or Bad (Good: no change or notification several weeks before or several days before; Bad: notification one day before or on the day or irregular notification);
fWork schedule stability was classified by monthly number of substitute work and timing of schedule change notification.
- 1. Killgore WD. Effects of sleep deprivation on cognition. Prog Brain Res 2010;185:105–29.ArticlePubMed
- 2. Buxton OM, Marcelli E. Short and long sleep are positively associated with obesity, diabetes, hypertension, and cardiovascular disease among adults in the United States. Soc Sci Med 2010;71(5):1027–36.ArticlePubMed
- 3. Kahn-Greene ET, Killgore DB, Kamimori GH, Balkin TJ, Killgore WD. The effects of sleep deprivation on symptoms of psychopathology in healthy adults. Sleep Med 2007;8(3):215–21.ArticlePubMed
- 4. Demers PA, DeMarini DM, Fent KW, Glass DC, Hansen J, Adetona O, et al. Carcinogenicity of occupational exposure as a firefighter. Lancet Oncol 2022;23(8):985–6.ArticlePubMed
- 5. IARC Monographs Vol 124 Group. Carcinogenicity of night shift work. Lancet Oncol 2019;20(8):1058–9.PubMed
- 6. Barger LK, Rajaratnam SM, Wang W, O'Brien CS, Sullivan JP, Qadri S, et al. Common sleep disorders increase risk of motor vehicle crashes and adverse health outcomes in firefighters. J Clin Sleep Med 2015;11(3):233–40.ArticlePubMedPMCPDF
- 7. Uehli K, Mehta AJ, Miedinger D, Hug K, Schindler C, Holsboer-Trachsler E, et al. Sleep problems and work injuries: a systematic review and meta-analysis. Sleep Med Rev 2014;18(1):61–73.ArticlePubMed
- 8. Suh S, Cho N, Zhang J. Sex differences in insomnia: from epidemiology and etiology to intervention. Curr Psychiatry Rep 2018;20(9):69.ArticlePubMedPDF
- 9. Ancoli-Israel S, Cooke JR. Prevalence and comorbidity of insomnia and effect on functioning in elderly populations. J Am Geriatr Soc 2005;53(7 Suppl):S264–71.PubMed
- 10. Cai GH, Theorell-Haglow J, Janson C, Svartengren M, Elmstahl S, Lind L, et al. Insomnia symptoms and sleep duration and their combined effects in relation to associations with obesity and central obesity. Sleep Med 2018;46:81–7.ArticlePubMed
- 11. Gellis LA, Lichstein KL, Scarinci IC, Durrence HH, Taylor DJ, Bush AJ, et al. Socioeconomic status and insomnia. J Abnorm Psychol 2005;114(1):111–8.ArticlePubMed
- 12. Shochat T. Impact of lifestyle and technology developments on sleep. Nat Sci Sleep 2012;4:19–31.ArticlePubMedPMC
- 13. Phillips B, Mannino DM. Do insomnia complaints cause hypertension or cardiovascular disease? J Clin Sleep Med 2007;3(5):489–94.ArticlePubMedPMCPDF
- 14. Joo JH, Lee DW, Choi DW, Park EC. Association between night work and dyslipidemia in South Korean men and women: a cross-sectional study. Lipids Health Dis 2019;18(1):75.ArticlePubMedPMCPDF
- 15. Kaaz K, Szepietowski JC, Matusiak L. Influence of itch and pain on sleep quality in atopic dermatitis and psoriasis. Acta Derm Venereol 2019;99(2):175–80.ArticlePubMed
- 16. Alvaro PK, Roberts RM, Harris JK. A systematic review assessing bidirectionality between sleep disturbances, anxiety, and depression. Sleep 2013;36(7):1059–68.ArticlePubMedPMC
- 17. Lamarche LJ, De Koninck J. Sleep disturbance in adults with posttraumatic stress disorder: a review. J Clin Psychiatry 2007;68(8):1257–70.ArticlePubMed
- 18. 2023 National Fire Agency Statistical Yearbook of Republic of Korea. https://www.nfa.go.kr/nfa/. Updated 2023. Accessed July 31, 2023.
- 19. Harvey SB, Milligan-Saville JS, Paterson HM, Harkness EL, Marsh AM, Dobson M, et al. The mental health of fire-fighters: An examination of the impact of repeated trauma exposure. Aust N Z J Psychiatry 2016;50(7):649–58.ArticlePubMedPDF
- 20. Jang TW, Jeong KS, Ahn YS, Choi KS. The relationship between the pattern of shift work and sleep disturbances in Korean firefighters. Int Arch Occup Environ Health 2020;93(3):391–8.ArticlePubMedPMCPDF
- 21. Garbarino S, Guglielmi O, Puntoni M, Bragazzi NL, Magnavita N. Sleep quality among police officers: implications and insights from a systematic review and meta-analysis of the literature. Int J Environ Res Public Health 2019;16(5):885.ArticlePubMedPMC
- 22. Good CH, Brager AJ, Capaldi VF, Mysliwiec V. Sleep in the United States military. Neuropsychopharmacology 2020;45(1):176–91.ArticlePubMedPMCPDF
- 23. McDowall K, Murphy E, Anderson K. The impact of shift work on sleep quality among nurses. Occup Med (Lond) 2017;67(8):621–5.ArticlePubMed
- 24. Khoshakhlagh AH, Al Sulaie S, Yazdanirad S, Orr RM, Dehdarirad H, Milajerdi A. Global prevalence and associated factors of sleep disorders and poor sleep quality among firefighters: a systematic review and meta-analysis. Heliyon 2023;9(2):e13250.ArticlePubMedPMC
- 25. Chin DL, Odes R, Hong O. Job stress and sleep disturbances among career firefighters in northern California. J Occup Environ Med 2023;65(8):706–10.ArticlePubMed
- 26. Lim DK, Baek KO, Chung IS, Lee MY. Factors related to sleep disorders among male firefighters. Ann Occup Environ Med 2014;26:11.ArticlePubMedPMCPDF
- 27. Thorndike FP, Ritterband LM, Saylor DK, Magee JC, Gonder-Frederick LA, Morin CM. Validation of the insomnia severity index as a web-based measure. Behav Sleep Med 2011;9(4):216–23.ArticlePubMed
- 28. Schneider D, Harknett K. Consequences of routine work-schedule instability for worker health and well-being. Am Sociol Rev 2019;84(1):82–114.ArticlePubMedPMCPDF
- 29. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 2001;16(9):606–13.ArticlePubMedPMC
- 30. Williams N. The GAD-7 questionnaire. Occup Med 2014;64(3):224.Article
- 31. Prins A, Ouimette P, Kimerling R, Cameron RP, Hugelshofer DS, Shaw-Hegwer J, et al. The primary care PTSD screen (PC-PTSD): development and operating characteristics. Prim Care Psychiatry 2003;9(1):9–14.Article
- 32. Oh HJ, Sim CS, Jang TW, Ahn YS, Jeong KS. Association between sleep quality and type of shift work in Korean firefighters. Ann Occup Environ Med 2022;34:e27.ArticlePubMedPMCPDF
- 33. Lim M, Lee S, Seo K, Oh HJ, Shin JS, Kim SK, et al. Psychosocial factors affecting sleep quality of pre-employed firefighters: a cross-sectional study. Ann Occup Environ Med 2020;32:e12.ArticlePubMedPMCPDF
- 34. Choi SM, Kim CW, Park HO, Park YT. Association between unpredictable work schedule and work-family conflict in Korea. Ann Occup Environ Med 2023;35:e46.ArticlePubMedPMCPDF
- 35. Hurley BF. Age, gender, and muscular strength. J Gerontol A Biol Sci Med Sci 1995;50 Spec No:41–4.PubMed
- 36. Costa G, Sartori S, Akerstedt T. Influence of flexibility and variability of working hours on health and well-being. Chronobiol Int 2006;23(6):1125–37.ArticlePubMed
- 37. Geiger-Brown J, Trinkoff A, Rogers VE. The impact of work schedules, home, and work demands on self-reported sleep in registered nurses. J Occup Environ Med 2011;53(3):303–7.ArticlePubMed
- 38. Akerstedt T, Kecklund G. What work schedule characteristics constitute a problem to the individual? A representative study of Swedish shift workers. Appl Ergon 2017;59(Pt A):320–5.ArticlePubMed
- 39. Boivin DB, Boudreau P. Impacts of shift work on sleep and circadian rhythms. Pathol Biol (Paris) 2014;62(5):292–301.ArticlePubMed
- 40. Meerlo P, Sgoifo A, Suchecki D. Restricted and disrupted sleep: effects on autonomic function, neuroendocrine stress systems and stress responsivity. Sleep Med Rev 2008;12(3):197–210.ArticlePubMed
- 41. Minkel J, Moreta M, Muto J, Htaik O, Jones C, Basner M, et al. Sleep deprivation potentiates HPA axis stress reactivity in healthy adults. Health Psychol 2014;33(11):1430–4.ArticlePubMed
- 42. Billings J, Focht W. Firefighter shift schedules affect sleep quality. J Occup Environ Med 2016;58(3):294–8.ArticlePubMed
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Environmental noise exposure and a new biomarker of Alzheimer's disease: A pilot study
Jonghun Lee, Cheol-Woon Kim, Youjin Kim, Seunghyun Lee, Joon Yul Choi, Wanhyung Lee
Journal of Alzheimer’s Disease.2026;[Epub] CrossRef - Mapping Connection and Direction Among Symptoms of Sleep Disturbance and Perceived Stress in Firefighters: Embracing the Network Analysis Perspective
Bin Liu, Mingxuan Zou, Lin Liu, Zhongying Wu, Yinchuan Jin, Yuting Feng, Qiannan Jia, Mengze Li, Lei Ren, Qun Yang
Nature and Science of Sleep.2025; Volume 17: 1143. CrossRef - Associations of long working hours with the use of combustible cigarettes, electronic cigarettes, and heated tobacco products among young adults: a population-based study of South Korea
Seong-Uk Baek, Jin-Ha Yoon
Postgraduate Medical Journal.2025;[Epub] CrossRef - Altered cortical myelination based on gray-to-white matter signal intensity contrast in shift workers
Jonghun Lee, Youjin Kim, Junbeom Lee, Joon Yul Choi, Wanhyung Lee
Brain Structure and Function.2025;[Epub] CrossRef - Association Between Obstructive Sleep Apnea and Atopic Dermatitis in the Korean Adult Population: Results From the 2019–2022 Korea National Health and Nutrition Examination Survey
Jung Min Lee, Wanhyung Lee
Allergy, Asthma & Immunology Research.2025; 17(6): 765. CrossRef - Impact of circadian rhythms on business efficiency and economic growth
Petra Prošková
Nierówności Społeczne a Wzrost Gospodarczy.2025; (83): 38. CrossRef
 Cite
CiteThe risk of insomnia by work schedule instability in Korean firefighters
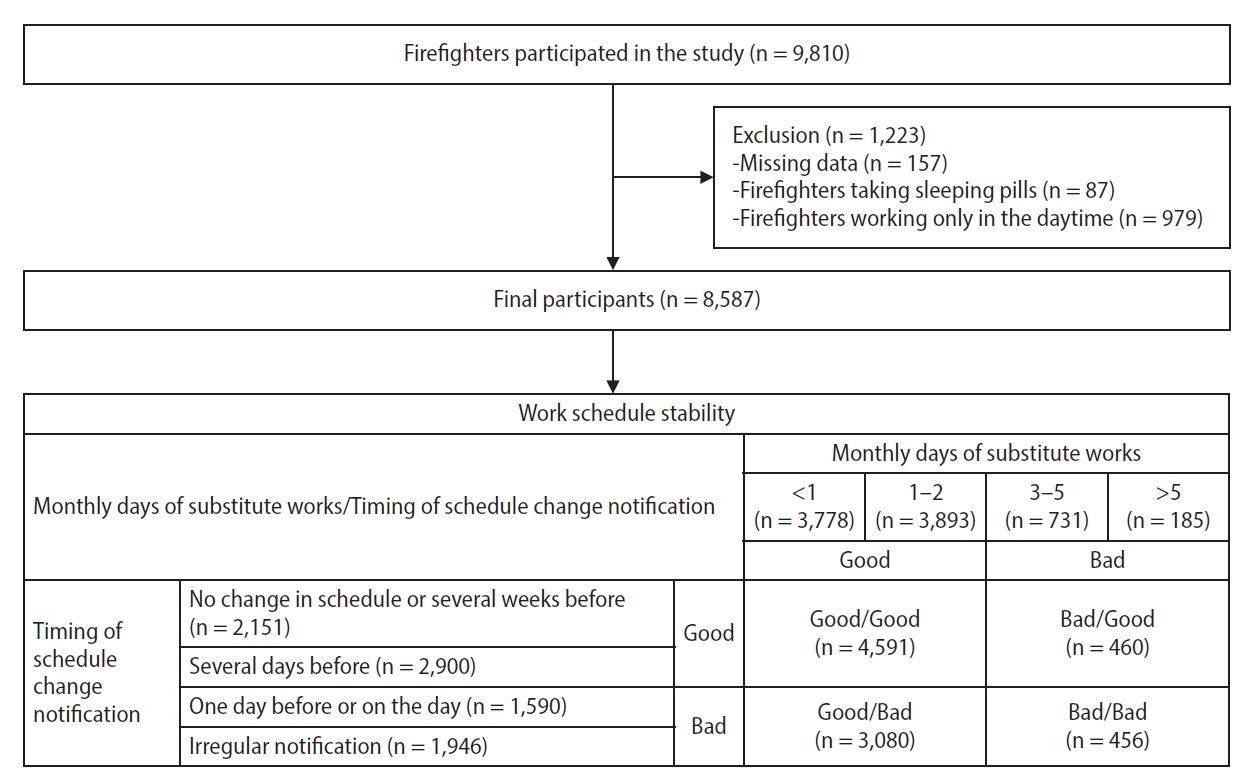
Fig. 1. Classification of participants according to work schedule stability.
Fig. 1.
The risk of insomnia by work schedule instability in Korean firefighters
| Variable | Total (n = 8,587) | Insomnia |
p-value | |
|---|---|---|---|---|
| No (n = 7,836, 91.25%) | Yes (n = 751, 8.75%) | |||
| Sex | ||||
| Male | 8,056 (93.8) | 7,366 (91.4) | 690 (8.6) | 0.021 |
| Female | 531 (6.2) | 470 (88.5) | 61 (11.5) | |
| Age (years) | ||||
| 20–29 | 1,241 (14.5) | 1,160 (93.5) | 81 (6.5) | 0.003 |
| 30–39 | 3,571 (41.6) | 3,265 (91.4) | 306 (8.6) | |
| 40–49 | 2,497 (29.1) | 2,269 (90.9) | 228 (9.1) | |
| ≥50 | 1,278 (14.9) | 1,142 (89.4) | 136 (10.6) | |
| Mean ± SD | 39.13 ± 8.50 | 39.03 ± 8.50 | 40.25 ± 8.40 | <0.001 |
| BMI (kg/m2) | ||||
| <25 | 5,482 (63.8) | 4,995 (91.1) | 487 (8.9) | 0.548 |
| ≥25 | 3,105 (36.2) | 2,841 (91.5) | 264 (8.5) | |
| Mean ± SD | 24.27 ± 2.51 | 24.27 ± 2.50 | 24.23 ± 2.67 | 0.631 |
| Education | ||||
| High school | 1,873 (21.8) | 1,716 (91.6) | 157 (8.4) | 0.184 |
| College | 2,720 (31.7) | 2,499 (91.9) | 221 (8.1) | |
| ≥University | 3,994 (46.5) | 3,621 (90.7) | 373 (9.3) | |
| Marital status | ||||
| Single | 2,691 (31.3) | 2,494 (92.7) | 197 (7.3) | 0.002 |
| Married | 5,896 (68.7) | 5,342 (90.6) | 554 (9.4) | |
| Monthly income (×1,000 KRW) | ||||
| 2,000–2,999 | 3,127 (36.4) | 2,895 (92.6) | 232 (7.4) | 0.003 |
| 3,000–4,999 | 4,195 (48.9) | 3,805 (90.7) | 390 (9.3) | |
| ≥5,000 | 1,265 (14.7) | 1,136 (89.8) | 129 (10.2) | |
| Smoking status | ||||
| Never smoker | 3,218 (37.5) | 2,918 (90.7) | 300 (9.3) | 0.047 |
| Ex-smoker | 2,934 (34.2) | 2,667 (90.9) | 267 (9.1) | |
| Current smoker | 2,435 (28.4) | 2,251 (92.4) | 184 (7.6) | |
| Alcohol consumption | ||||
| No | 2,356 (27.4) | 2,127 (90.3) | 229 (9.7) | 0.049 |
| Yes | 6,231 (72.6) | 5,709 (91.6) | 522 (8.4) | |
| Caffeine intake | ||||
| No | 1,374 (16.0) | 1,227 (89.3) | 147 (10.7) | 0.005 |
| Yes | 7,213 (84.0) | 6,609 (91.6) | 604 (8.4) | |
| Exercise | ||||
| No | 2,741 (31.9) | 2,468 (90.0) | 273 (10.0) | 0.006 |
| Yes | 5,846 (68.1) | 5,368 (91.8) | 478 (8.2) | |
| Variable | Total (n = 8,587) | Insomnia |
p-value |
|
|---|---|---|---|---|
| No (n = 7,836, 91.25%) | Yes (n = 751, 8.75%) | |||
| Hypertension | ||||
| Yes | 779 (9.1) | 661 (84.9) | 118 (15.1) | <0.001 |
| No | 7,808 (90.9) | 7,175 (91.9) | 633 (8.1) | |
| Dyslipidemia | ||||
| Yes | 751 (8.7) | 987 (86.7) | 151 (13.3) | <0.001 |
| No | 7,836 (91.3) | 6,849 (91.9) | 600 (8.1) | |
| Cardiac disease | ||||
| Yes | 177 (2.1) | 138 (78.0) | 39 (22.0) | <0.001 |
| No | 8,410 (97.9) | 7,398 (91.5) | 712 (8.5) | |
| Skin disease | ||||
| Yes | 949 (11.1) | 787 (82.9) | 162 (17.1) | <0.001 |
| No | 7,638 (88.9) | 7,049 (92.3) | 589 (7.7) | |
| Depressive symptom |
||||
| Yes | 1,454 (16.9) | 982 (67.5) | 472 (32.5) | <0.001 |
| No | 7,133 (83.1) | 6,854 (96.1) | 279 (3.1) | |
| Anxiety symptom |
||||
| Yes | 981 (11.4) | 614 (62.6) | 367 (37.4) | <0.001 |
| No | 7,606 (88.6) | 7,222 (95.0) | 384 (5.0) | |
| PTSD symptom |
||||
| Yes | 826 (9.6) | 558 (67.6) | 268 (32.4) | <0.001 |
| No | 7,761 (90.4) | 7,278 (93.8) | 483 (6.2) | |
| Variable | Total (n = 8,587) | Insomnia |
p-value |
|
|---|---|---|---|---|
| No (n = 7,836, 91.25%) | Yes (n = 751, 8.75%) | |||
| Type of shift | ||||
| 3-Day cycle | 667 (7.8) | 618 (92.7) | 49 (7.3) | 0.552 |
| 6-Day cycle | 156 (1.8) | 140 (89.7) | 16 (10.3) | |
| 9-Day cycle | 1,169 (13.6) | 1,058 (90.5) | 111 (9.5) | |
| 21-Day cycle | 6,215 (72.4) | 5,675 (91.3) | 540 (8.7) | |
| Others | 380 (4.4) | 345 (90.8) | 35 (9.2) | |
| Job | ||||
| Administration | 96 (1.1) | 89 (92.7) | 7 (7.3) | 0.014 |
| Fire suppression | 2,956 (34.4) | 2,684 (90.8) | 272 (9.2) | |
| EMS | 2,496 (29.1) | 2,258 (90.5) | 238 (9.5) | |
| Rescue | 952 (11.1) | 897 (94.2) | 55 (5.8) | |
| Fire investigation | 220 (2.6) | 198 (90.0) | 22 (10.0) | |
| Others | 1,867 (21.7) | 1,710 (91.6) | 157 (8.4) | |
| Monthly number of substitute work |
||||
| <1 | 3,778 (44.0) | 3,522 (93.2) | 256 (6.8) | <0.001 |
| 1–2 | 3,893 (45.3) | 3,525 (90.2) | 368 (9.5) | |
| 3–5 | 731 (8.5) | 633 (86.6) | 98 (13.4) | |
| >5 | 185 (2.2) | 156 (84.3) | 29 (15.7) | |
| Timing of schedule change notification |
||||
| No change or several weeks before | 2,151 (25.0) | 2,034 (94.6) | 117 (5.4) | <0.001 |
| Several days before | 2,900 (33.8) | 2,670 (92.1) | 230 (7.9) | |
| One day before or on the day | 1,590 (18.5) | 1,412 (88.8) | 178 (11.2) | |
| Irregularly notification | 1,946 (22.7) | 1,720 (88.4) | 226 (11.6) | |
| Work schedule stability |
||||
| Good/Good | 4,591 (53.5) | 4,304 (93.7) | 287 (6.3) | <0.001 |
| Good/Bad | 3,080 (35.9) | 2,743 (89.1) | 337 (10.9) | |
| Bad/Good | 460 (5.4) | 400 (87.0) | 60 (13.0) | |
| Bad/Bad | 456 (5.3) | 389 (85.3) | 67 (14.7) |
| Crude | Model 1 |
Model 2 |
Model 3 |
|
|---|---|---|---|---|
| Monthly number of substitute work |
||||
| <1 | 1 (ref.) | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| 1–2 | 1.436 (1.216–1.696) | 1.375 (1.064–1.778) | 1.298 (1.083–1.556) | 1.327 (1.103–1.597) |
| 3–5 | 2.130 (1.663–2.729) | 2.234 (1.741–2.867) | 1.738 (1.320–2.289) | 1.794 (1.355–2.375) |
| >5 | 2.558 (1.687–3.878) | 2.694 (1.773–4.092) | 1.783 (1.121–2.835) | 1.823 (1.142–2.910) |
| Timing of schedule change notification |
||||
| No change or several weeks before | 1 (ref.) | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| Several days before | 1.498 (1.190–1.885) | 1.517 (1.205–1.910) | 1.449 (1.132–1.854) | 1.448 (1.130–1.855) |
| One day before or on the day | 2.192 (1.719–2.794) | 2.130 (1.669–2.717) | 1.729 (1.329–2.249) | 1.719 (1.320–2.238) |
| Irregular notification | 2.284 (1.811–2.882) | 2.285 (1.810–2.885) | 1.810 (1.407–2.327) | 1.816 (1.410–2.338) |
| Work schedule stability |
||||
| Good/Good | 1 (ref.) | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| Good/Bad | 1.842 (1.563–2.172) | 1.801 (1.527–2.125) | 1.475 (1.233–1.763) | 1.480 (1.237–1.771) |
| Bad/Good | 2.249 (1.672–3.026) | 2.314 (1.719–3.115) | 1.789 (1.290–2.481) | 1.862 (1.340–2.588) |
| Bad/Bad | 2.583 (1.942–3.436) | 2.609 (1.959–3.473) | 1.851 (1.347–2.544) | 1.885 (1.366–2.602) |
Table 1. The distribution of participants and prevalence of insomnia by general characteristics
Values are presented as number (%) or mean ± standard error. SD: standard deviation; BMI: body mass index; KRW: Korean Won; ISI: Insomnia Severity Index. Insomnia was classified with No or Yes by ISI score (No: <15; Yes: ≥15); Calculated by chi-square test for binomial variables and t-test for numeric variables.
Table 2. The distribution of participants and prevalence of insomnia by underlying diseases and psychological symptoms
Values are presented as number (%). PTSD: post-traumatic stress disorder; ISI: Insomnia Severity Index; PHQ-9: Patient Health Questionnaire-9; GAD-7: Generalized Anxiety Disorder-7; PC-PTSD: Primary Care-PTSD screen. Insomnia was classified with No or Yes by ISI score (No: <15, Yes: ≥15); Calculated by chi-square test; Depressive symptom was classified with No or Yes by PHQ-9 score (No: <5, Yes: ≥5); Anxiety symptom was classified with No or Yes by GAD-7 score (No: <5, Yes: ≥5); PTSD symptom was classified with No or Yes by PC-PTSD (No: <3, Yes: ≥3 items).
Table 3. The distribution of participants and prevalence of insomnia by work-related variables
Values are presented as number (%). EMS: emergency medical services; ISI: Insomnia Severity Index. Insomnia was classified with No or Yes by ISI score (No: <15, Yes: ≥15); Calculated by chi-square test; Monthly number of substitute works was classified with Good or Bad (Good: monthly number <3; Bad: monthly number ≥3); Timing of schedule change notification was classified with Good or Bad (Good: no change or notification several weeks before or several days before; Bad: notification one day before or on the day or irregular notification); Work schedule stability was classified by monthly number of substitute work and timing of schedule change notification.
Table 4. The odds ratios of insomnia by work schedule change
The adjusted odds ratio (95% confidence interval) was calculated via binomial logistic regression analyses. Model 1: adjusted for sex and age; Model 2: adjusted for all variables in Model 1, body mass index, education, smoking status, alcohol consumption, caffeine intake, exercise, hypertension, dyslipidemia, cardiac disease, skin disease, and depressive symptom; Model 3: adjusted for all variables in model 2, shift type, and job; Monthly number of substitute work was classified with Good or Bad (Good: monthly number <3; Bad: monthly number ≥3); Timing of schedule change notification was classified with Good or Bad (Good: no change or notification several weeks before or several days before; Bad: notification one day before or on the day or irregular notification); Work schedule stability was classified by monthly number of substitute work and timing of schedule change notification.

