
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 35; 2023 > Article
- Original Article Incidence rates of injury, musculoskeletal, skin, pulmonary and chronic diseases among construction workers by classification of occupations in South Korea: a 1,027 subject-based cohort of the Korean Construction Worker’s Cohort (KCWC)
-
Seungho Lee1
 , Yoon-Ji Kim2, Youngki Kim1,2, Dongmug Kang1,2, Seung Chan Kim3, Se-Yeong Kim1,2
, Yoon-Ji Kim2, Youngki Kim1,2, Dongmug Kang1,2, Seung Chan Kim3, Se-Yeong Kim1,2 -
Annals of Occupational and Environmental Medicine 2023;35:e26.
DOI: https://doi.org/10.35371/aoem.2023.35.e26
Published online: July 24, 2023
1Department of Occupational and Environmental Medicine, Pusan National University Yangsan Hospital, Yangsan, Korea.
2Department of Preventive, and Occupational & Environmental Medicine, School of Medicine, Pusan National University, Yangsan, Korea.
3Department of Biostatistics Cooperation Center, Gyeongsang National University Hospital, Jinju, Korea.
- Correspondence: Se-Yeong Kim. Department of Preventive, and Occupational & Environmental Medicine, School of Medicine, Pusan National University, 49 Busandaehak-ro, Yangsan 50612, Korea. 30white@pusan.ac.kr
• Received: December 26, 2022 • Revised: May 23, 2023 • Accepted: June 12, 2023
Copyright © 2023 Korean Society of Occupational & Environmental Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background The objective of this study is to investigate the differences in incidence rates of targeted diseases by classification of occupations among construction workers in Korea.
-
Methods In a subject-based cohort of the Korean Construction Worker’s Cohort, we surveyed a total of 1,027 construction workers. As occupational exposure, the classification of occupations was developed using two axes: construction business and job type. To analyze disease incidence, we linked survey data with National Health Insurance Service data. Eleven target disease categories with high prevalence or estimated work-relatedness among construction workers were evaluated in our study. The average incidence rates were calculated as cases per 1,000 person-years (PY).
-
Results Injury, poisoning, and certain other consequences of external causes had the highest incidence rate of 344.08 per 1,000 PY, followed by disease of the musculoskeletal system and connective tissue for 208.64 and diseases of the skin and subcutaneous tissue for 197.87 in our cohort. We especially found that chronic obstructive pulmonary disease was more common in construction painters, civil engineering welders, and civil engineering frame mold carpenters, asthma in construction painters, landscape, and construction water proofers, interstitial lung diseases in construction water proofers.
-
Conclusions This is the first study to systematically classify complex construction occupations in order to analyze occupational diseases in Korean construction workers. There were differences in disease incidences among construction workers based on the classification of occupations. It is necessary to develop customized occupational safety and health policies for high-risk occupations for each disease in the construction industry.
BACKGROUND
The construction industry has a higher disease burden on its workers than other industries.1,2 According to Korea’s employment and labor statistics, the number of occupational injuries and illnesses per 100 construction workers has steadily increased from 0.84 in 2015 to 1.17 in 2020. Furthermore, the number of occupational fatality per 10,000 construction workers has steadily increased from 1.76 in 2015 to 2.48 in 2020.3 Despite of the increasing health threat to Korean construction workers, the epidemiology of integrated Korean construction workers’ diseases has not yet been studied. In the United States and some European countries, there are many epidemiological studies conducted about work-related disease burdens in construction industry.4,5,6,7,8 It has been reported that musculoskeletal diseases, skin diseases, respiratory diseases, injury, certain other consequences of external causes occur frequently among construction workers.7,8,9
There are several kinds of occupations in the construction industry. There are 126 occupations in the Korean construction industry based on the unit wages by job family in 2022.10 Each type of occupations is exposed to a variety of different risk factors, depending on their characteristics of job type and working environment.11,12,13 Various diseases occur depending on the occupations due to the difference of the exposed risk factors. However, few studies focused on these differences by classification of occupations in the construction industry. Previous studies on the health effects in the construction industry have focused on specific diseases such as rheumatologic diseases, sarcoidosis, lung cancer, or skin diseases14,15,16,17,18 or specific risk factors such as asbestos or ergonomic factors.19,20 These studies did not cover all occupations in the construction industry.
To understand the health status of construction workers in Korea, it is necessary to understand the differences of health burden by classification of occupations in the construction industry. Such findings may be useful in customized preventing health problems in all construction occupations. Therefore, it is necessary to systematically classify construction industry worker’s occupations. The Korean Construction Worker’s Cohort (KCWC) was established at 2018 due to this necessity. This paper was based on the 1,027 subject-based cohort, a sub-cohort of KCWC, and analyzed to find out the health status based on classification of occupations among workers in construction industry.
METHODS
This study used data from the KCWC established in 2018. The KCWC was designed as a hybrid of a subject-based cohort and a data-based cohort using nationwide representative data. From 2018 to 2019, 1,027 construction workers who visited the Busan branch of the Construction Workers’ Mutual Aid Association (CWMAA) were recruited for the subject-based cohort. We conducted a survey on construction workers who are over 20 years old and have objectively proven occupational history in the construction industry for at least one year through the retirement mutual aid fund of CWMAA. This survey was conducted face-to-face by trained two investigators. The questionnaire included socio-demographic information (including sex, age, height, weight, and resident registration number), medical history (disease morbidity likewise hypertension, diabetes mellitus, dyslipidemia, stroke, ischemic heart diseases, osteoarthritis, etc.), lifestyle (smoking and drinking habit), and occupational history, etc.
The occupational history included not only careers in the construction industry, but also careers in other industries. Essentially, the relevant occupation’s starting date (year-month) and working period were investigated. For occupational history in other industries, occupations according to the 6th Korean Standard Classification of Occupations,21 industries according to the 9th Korean Standard Industrial Classification22 were investigated. For occupational history in the construction industry, construction businesses, job types, and hazardous material exposure were investigated in depth. We classified construction worker’s occupations systematically based on construction businesses and job type. Each construction worker’s classification of occupations was determined by the occupation with the longest employment. There were total of 106 classifications of occupations. Construction businesses were surveyed according to classification based on Korean enforcement decree of the framework act on the construction industry. Job types were surveyed according to a 2018 survey report on the unit wages of the construction industry by the Construction Association of Korea.10 Classifications of construction businesses and job types are shown in Supplementary Table 1. Working duration was classified according to the skill class system (beginner [< 3 years], intermediate [≥ 3, < 9 years], advanced [≥ 9, < 21 years], and expert [≥ 21 years]).23
The National Health Insurance (NHI) database, formed by the NHIS, is a nationwide public information data on health care utilization, health screening, socio-demographic variables, and disease morbidity for almost the entire population of South Korea.24 We obtained the “Customized health information data” from the NHIS using resident registration numbers.25 Through integrated literature reviews, we evaluated eleven target disease categories with high prevalence or estimated work-relatedness among construction workers. Injuries, poisonings, musculoskeletal diseases, skin diseases, and respiratory diseases (emphysema, chronic obstructive pulmonary disease [COPD] [except MacLeod’s syndrome with diagnosis code J43.0], asthma and interstitial lung diseases) were chosen as study target diseases.7,8,9 In addition, cancers, general chronic diseases (hypertensive diseases and diabetes mellitus) and overwork-related diseases (ischemic heart diseases and stroke) were chosen26 to understand the overall health burden of the construction workers.
We examined the disease occurrence in the NHI claim data of 1,027 construction workers from 2002 to 2018. It made used of the seventh revision of the Korean Classification of Diseases (KCD-7). KCD-7 is the Korean version of the World Health Organization’s International Classification of Diseases, 10th Edition.27
Fig. 1 depicts the study design. To define a new occurred disease, all participants had past history period. We excluded the workers attacked cases within past history period before the first employment. The past period were mostly 3 years of all diseases (except: injuries and skin diseases had not past history period). For accuracy, we selected the disease code in both the inpatient and outpatient medical charts but severe diseases such as cancers, ischemic heart diseases, and stroke were searched from only inpatient medical charts. In addition, stroke patients were enrolled only with computed tomography or magnetic resonance imaging prescription codes. Only those with hypertensive diseases and diabetes mellitus who took medications at least twice a year for three years during the observation period were enrolled (Supplementary Table 2).
Fig. 1

Subject-based cohort study design in Korean Construction Worker’s Cohort. Example of a new onset disease in 2010 in a person who started working in construction industry since 2005.
Based on the survey results, basic socio-demographic characteristics and occupational history in the construction industry were extracted and descriptive analysis with stratification was performed. Age and work duration were expressed as mean ± standard deviation. The independent t-test and χ2 test were used to compare the sex differences. A p-value of < 0.05 was considered statistically significant. The mean follow-up period and the average incidence rates for each disease were calculated. The mean follow-up period was calculated as total of each period from the beginning of observation to the occurrence of diseases divided by the occurrence number of diseases. Average incidence rates were calculated as below.
The average incidence rates were calculated based on classification of occupations. We examined twelve occupations out of 106; 6 job types in construction (frame mold carpenters, concrete reinforcing iron workers, bricklayers, water proofers, plasterers, and painters), three job types in civil engineering (frame mold carpenters, concrete reinforcing iron workers, and welders) and three construction businesses (plant, landscape, and specialized construction). When selecting a classification of occupations for analysis, we considered the frequency and the degree of exposure to risk factors. All statistical analyses were performed using SPSS software v26 (IBM, Armonk, NY, USA) for Windows.
The study was carried out in accordance with the Helsinki Declaration, and was approved by the Pusan National University Yangsan Hospital’s Institutional Review Board Committee (IRB No. 04-2018-014 and date of approval was June 18, 2018). All subjects provided informed consent when they were surveyed and enrolled.
RESULTS
From 2018 to 2019, we surveyed 1,029 workers, with 2 of them being excluded due to duplicates. So, a total of 1,027 enrollees of cohort were analyzed. Table 1 showed basic socio-demographic and occupational characteristics. The average age of all workers was 59.3 years old. The average age of female was 61.1 years, which was older than that of male (59.2 years). The proportion of smoker (current and ex-smoker) in male was 82.3%, which was significantly higher than that of females (7.7%).
Table 1
Socio-demographic and occupational characteristics of the subject-based cohort in Korean Construction Worker’s Cohort
Current and ex-smokers are both classified as smokers. The p-values were calculated by t-test for continuous variables and χ2 for categorical variables.
*p < 0.05, **p < 0.01, ***p < 0.001.
aThe p-values were calculated using an independent sample t-test.
bThe p-values were calculated using Pearson’s χ2 test.
In classification of 5 construction industry businesses, construction was the most common (64.7%) and the landscaping was the lowest proportion (2.8%). Males were more likely to work in civil engineering or specialized construction than females. Distribution of job types in each construction industry business is presented in Supplementary Tables 3, 4, 5, 6, 7. In the construction and civil engineering, frame mold carpenters except for others accounted for a large portion with 24.5% and 30.8%, respectively. The workers have worked for more than 21 years were the most (40.9%) in total subjects. The average working duration of male workers was 19.9 years, which was significantly longer than that of females (11.4 years).
In cohort, the follow-up period for interstitial lung diseases was the longest for 10.35 years, followed by ischemic heart diseases for 10.30 years, stroke for 10.26 years (Table 2). The follow-up period for injury, poisoning, and certain other external causes was the shortest for 2.62 years.
Table 2
Mean follow-up period and targeted disease incidence rates of the subject-based cohort in Korean Construction Worker’s Cohort
Among targeted diseases, the highest incidence rate was 344.08 per 1,000 person-years (PY) in injury, poisoning, and certain other external causes. The second was the diseases of the musculoskeletal system and connective tissue as 208.64 per 1,000 PY and third was the diseases of the skin and subcutaneous tissue as 197.87 per 1,000 PY. There was a sex difference that the diseases of the musculoskeletal system and connective tissue in male and diseases of the skin and subcutaneous tissue in female were the second highest in each sex (Table 2).
The incidence rates for targeted diseases of a total of 1,027 people in the cohort were compared and analyzed according to the classification of occupations with high frequency (Table 3, Fig. 2). Total cancer was not analyzed due to the small number of subjects. In Table 3, the occupations with the highest incidence rate for each target disease were boldly labeled from first to third. The occupations with the highest incidence rate for each target disease were indicated by red dots from first to third in Fig. 2. The incidence rate for injury, poisoning, and certain other consequences of external causes was the highest in civil engineering welders at 619.05 per 1,000 PY. The incidence rate for diseases of the musculoskeletal system and connective tissue was the highest in construction bricklayers at 571.43 per 1,000 PY and the incidence rate for disease of the skin and subcutaneous tissue was the highest in construction bricklayers at 327.27 per 1,000 PY. In the respiratory diseases, the incidence rate for emphysema and other COPD was the highest in construction painters at 16.53 per 1,000 PY, asthma in construction painters at 67.80 per 1,000 PY, and interstitial lung diseases in construction water proofers at 4.70 per 1,000 PY. In chronic diseases, the incidence rate for hypertensive diseases was the highest in construction painters at 53.33 per 1,000 PY, and diabetes mellitus in construction bricklayers at 10.64 per 1,000 PY. In cardio-cerebrovascular diseases, the incidence rate for ischemic heart diseases was the highest in construction painters at 7.69 per 1,000 PY, and stroke in civil engineering concrete reinforcing iron workers at 11.17 per 1,000 PY.
Table 3
Targeted disease incidence rates based on classification of occupations of the subject-based cohort in Korean Construction Worker’s Cohort
Fig. 2
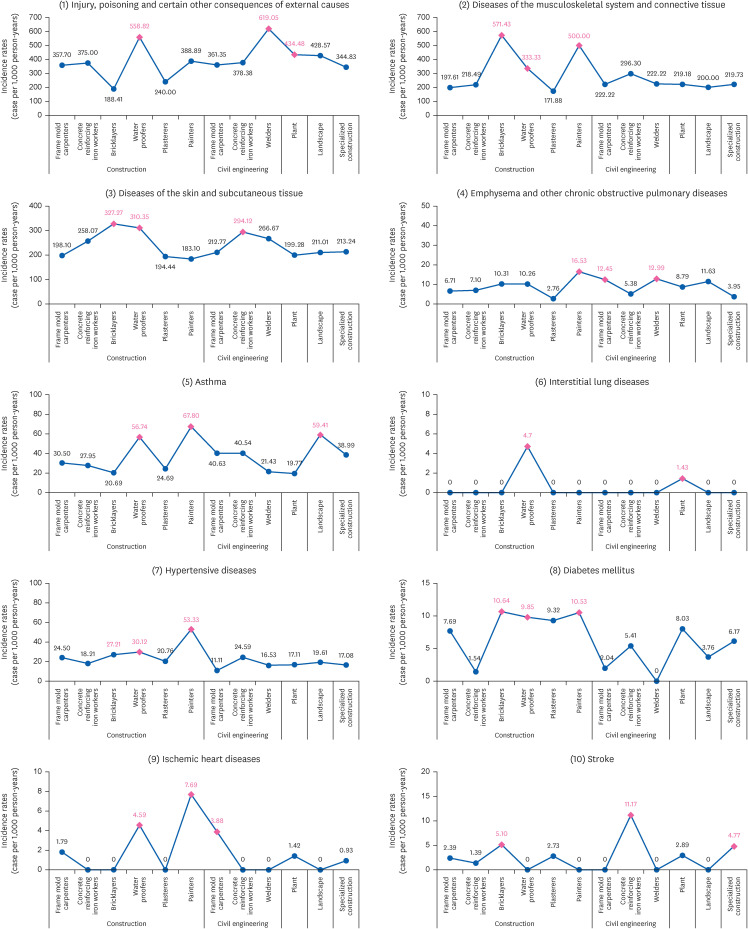
Target disease incidence rates based on classification of occupations of the subject-based cohort in Korean Construction Worker’s Cohort.
DISCUSSION
In this study, we conducted a face-to-face survey to establish the subject-based cohort of KCWC. A total of 1,027 construction workers responded. Through a linkage based on the resident registration number, we combined and analyzed exposure (survey) data and their health status (NHIS) data. The incidence rate of diseases among all construction workers was the highest, at 344.08 per 1,000 PY for injury, poisoning, and certain other consequences of external causes. The next highest was diseases of the musculoskeletal system and connective tissue with 208.64 per 1,000 PY, followed by disease of the skin and subcutaneous tissue with 197.85 per 1,000 PY.
Construction workers commonly face considerable health risk due to injury, musculoskeletal diseases, and skin diseases. In our study, the incidence of injury, poisoning, and certain other consequences of external causes was the highest. We thought that this is attributed to a higher number of injuries compared to poisoning cases. In our recent study analyzed the compensation insurance data for occupational diseases among construction workers in Korea from 2009 to 2018, the cases of poisoning were fewer claims than injuries such as rupture, laceration, amputation and abrasion.28 A German cohort study reported that male construction workers had a significantly higher standardized incidence rate ratio (SIRR) of disability from injuries for (SIRR: 2.5) and musculoskeletal diseases (SIRR: 2.16) and higher but not significant SIRR of disability from skin diseases (SIRR: 1.61) in comparison with general work force.29 A United Kingdom cohort study found the significantly higher SIRRs of musculoskeletal disorders (SIRR: 1.9) and skin disorders (SIRR: 1.6).7
We also compared and analyzed the disease incidence rates according to the classification of occupations based on construction businesses and job types. For injury, poisoning, and certain other consequences of external causes, civil engineering welders; for diseases of the musculoskeletal system and connective tissues, construction; for skin and subcutaneous tissue diseases, construction bricklayer showed the highest incidence rate. Previous studies also reported various occupations with high incidence of these diseases. There were significantly higher SIRR of disability from accidents for carpenters (SIRR: 2.31), plasterers (SIRR: 3.00), and bricklayers (SIRR: 1.63) compared with blue collar workers.29 In United Kingdom, there were significantly higher SIRR of disability due to musculoskeletal disorders for welders (SIRR: 1.7), road construction operatives (SIRR: 6.1) than other workers. In addition, there were significant higher SIRR of contact dermatitis for metalworking production and maintenance fitters (SIRR: 1.4) and construction trades n.e.c. (SIRR: 1.4).11 Injury and musculoskeletal disease were the major causes of worker’s compensation claims in the construction industry.28 This may be because of the dangers of the construction site, excessive workload, and inappropriate safety perception. Common occupational hygiene interventions for the construction industry are required rather than a detailed classification of occupations.30,31 Occupational skin diseases were correlated with high-temperature exposure and skin contact with chemical products. Specifically, high-temperature exposure was significantly associated with the construction industry.32 Among construction workers, high incidence rates were reported for floor layers, tile setters, bricklayers, concrete placers, and concrete finishers. 71% of these cases were allergic contact dermatitis and more than half of allergic contact dermatitis was due to epoxy chemical.33 Future studies assessing heat exposure and skin contact with chemical products in the classification of occupations and identifying risk factors will facilitate reduction of occupational skin diseases in construction workers.28
For asthma, construction painters, construction water proofers, and landscape workers showed a higher incidence rate than other occupations in this study. There were significantly higher SIRR of asthma for welding trades (SIRR: 4.7), metalworking production and maintenance fitters (SIRR: 2.0) and painters and decorators (SIRR: 1.9) in other study. In addition, chest physicians picked wood and wood dust, paints and dyes and isocyanate as suspected causal agents for asthma among construction workers.11 These substances could be suspected as the causative agents of classification of occupations with a high incidence rate for asthma in this study. These results warrant the need of research to explore and manage the relevant allergic substance exposures.
Previous studies have shown an increased risk in construction workers for chronic pulmonary diseases such as COPD and interstitial lung diseases. The United States cohort study reported significantly higher adjusted odds ratio (OR) for chronic lung disease (OR: 1.93). A Sweden cohort study reported that mortality due to COPD was significantly increased by occupational exposure factors such as vapors, dusts, gases, and fumes.34 In addition, a United States cohort study reported that high exposure to these factors was associated with a yearly decline of forced expiratory volume in 1 second and forced vital capacity.35 In our study, construction painters had the highest incidence rate of COPD, and construction water proofers had the highest incidence rate of interstitial lung diseases. Occupational exposure to dust, fumes, and particular matters may be ascribed to the occurrence of chronic respiratory diseases in construction workers.36,37 Thus, industrial hygiene management is required for the classification of occupations with relatively high incidence.
In this study, the incidence rates for ischemic heart diseases, stroke, hypertensive diseases and diabetes mellitus showed differences by occupations. The work-relevance of these diseases among construction workers is still unclear. There are studies that found no increasing risk of these diseases among construction workers,4,29 but there are also study that found significantly increased relative risks (RRs) for stroke (RR: 1.85) and ischemic heart disease (RR: 1.59).38 In addition, there are studies that investigate the influence of poor lifestyles including smoking, heavy drinking, and bad diet that are risk factors for the above diseases among construction workers,39,40,41 while there is study suggested that occupational exposure to noise, cold environment, particulate air pollution and underground environment can increase the risk of cardiovascular diseases.12,42,43 However, we think it is difficult to define the work-relevance of it because the non-occupational risk factors such as age and lifestyle contribute to high.
There were similarities and differences on disease incidence rates according to classification of occupations between studies. These may be due to differences in classification of occupations, operational definitions of target diseases, or working environments across countries, even within the same occupations. In the case of occupational injuries in the construction workers, it has been reported to be associated with various factors such as work duration, vibration tools, hazard awareness, alcohol consumption, and working environment.42,44
This study has several limitations. First, we had no reference group. As a result, it is difficult to find that diseases affect construction workers more frequently than the general population. This is because the subject-based cohort of KCWC focused on practically investigating the differences on disease incidence by occupations among construction industry. Further, we did not adjust confounders such as age, sex, and smoking. As the total number of subjects was 1,027, it was challenging to adjust the confounders because the number of subjects in the classification of occupations was insufficient. Particularly, because a majority of the surveys participants were male, the disease incidence rates could be seen as representative health status of male construction workers. Moreover, we did not consider changes in the type of jobs of workers in the construction industry. This was difficult to evaluate because the size of the cohort was small compared with the various classifications of occupations. However, these limitations are expected to be overcome through data-based cohorts to be reported by ours in the future. A data-based cohort, which is a sub-cohort other than a subject-based cohort of KCWC, was established following the employment insurance database and CWMAA database. This data-based cohort included more than 5 million Korean construction workers with most daily workers and comprised public officials as a control group. In that, we aimed to analyze the health effects adjusted for confounding variables following a detailed classification of occupations.
Nevertheless, our study is very meaningful in that it is the first study to examine the incidence rates of various diseases using a systematically classification of construction workers’ occupations. Finding the differences in disease incidence rates among construction workers according to classification of occupations can be the first step in searching for risk factors such as hazardous work environment or substance exposures. Through face-to-face survey, we investigated exactly careers in the construction industry. In addition, we systematically classified construction workers’ occupations based on the two axes of business and job type. After that, we linked the survey result and the NHIS data for the accurate diagnosis. Therefore, our subject-based cohort of KCWC can be considered as the result of linking relatively accurate exposure assessment with health status.
CONCLUSIONS
We presented the targeted disease incidence rates among Korean construction workers based on classification of occupations. The most common health problems were injuries, musculoskeletal diseases, and skin diseases. We discovered that emphysema and COPD were more common in construction painters, civil engineering welders, and civil engineering frame mold carpenters, asthma in construction painters, landscape, and construction water proofers, interstitial lung diseases in construction water proofers. It is meaningful because this is the first study that analyzed health problems of Korean construction workers by systematically classifying complex occupations. Through this subject-based study of KCWC, it is expected to be used to customized occupational safety and health policies for high-risk occupations by disease in the construction industry.
ACKNOWLEDGEMENTS
We would like to express our gratitude to the Occupational Safety and Health Research Institute (OSHRI) for funding this research. The contents of the paper are solely the author’s responsibility and do not necessarily represent the official views of the OSHRI.
Abbreviations
COPD
chronic obstructive pulmonary disease
CWMAA
Construction Workers’ Mutual Aid Association
KCD
Korean Standard Classification of Diseases
KCWC
Korean Construction Worker’s Cohort
NHI
National Health Insurance
NHIS
National Health Insurance Service
OR
odds ratio
PY
person-years
RR
relative risk
SIRR
standardized incidence rate ratio
-
Funding: This study was supported by Occupational Safety and Health Research Institute, Korea Occupational Safety and Health Agency in the Republic of Korea (grant number: 202204166DO-00) and 2022 research grant from Pusan National University Yangsan Hospital.
-
Competing interests: The authors declare that they have no competing interests.
-
Author contributions:
Conceptualization: Kim SY.
Data curation: Kim SY, Kim YJ.
Formal analysis: Kim SY, Lee S, Kim SC.
Funding acquisition: Kim SY.
Investigation: Kim SY, Kim YJ.
Methodology: Kim SY, Lee S.
Project administration: Kim SY.
Resources: Kim SY.
Software: Kim SY, Kim SC.
Supervision: Kim SY, Kang D, Kim Y, Validation.
Visualization: Kim YJ.
Writing - original draft: Kim SY, Lee S.
Writing - review & editing: Kim SY, Lee S, Kim YJ.
NOTES
SUPPLEMENTARY MATERIALS
Supplementary Table 1
Classifications of occupations based on construction businesses and job types among construction workers
Supplementary Table 2
Operational definition of targeted diseases of the subject-based cohort in Korean Construction Worker’s Cohort
Supplementary Table 3
Job type distribution among construction workers in construction business
Supplementary Table 4
Job type distribution among construction workers in civil engineering business
Supplementary Table 5
Job type distribution among construction workers in plant business
Supplementary Table 6
Job type distribution among construction workers in landscape business
Supplementary Table 7
Job type distribution among construction workers in specialized construction business
- 1. Yang L, Branscum A, Smit E, Dreher D, Howard K, Kincl L. Work-related injuries and illnesses and their association with hour of work: analysis of the Oregon construction industry in the US using workers’ compensation accepted disabling claims, 2007-2013. J Occup Health 2020;62(1):e12118. 32515883.ArticlePubMedPMCPDF
- 2. Ringen K, Dong XS, Goldenhar LM, Cain CT. Construction safety and health in the USA: Lessons from a decade of turmoil. Ann Work Expo Health 2018;62(suppl_1):S25–S33. 30212888.ArticlePubMed
- 3. Korean Statistical Information Service. Summary of occupational accidents by industry (divisions). Updated 2022]. Accessed October 18, 2022]. https://kosis.kr/statHtml/statHtml.do?orgId=118&tblId=DT_11806_N000&conn_path=I2&language=en .
- 4. Dong XS, Wang X, Daw C, Ringen K. Chronic diseases and functional limitations among older construction workers in the United States: a 10-year follow-up study. J Occup Environ Med 2011;53(4):372–380. 21407096.PubMed
- 5. Arndt V, Rothenbacher D, Daniel U, Zschenderlein B, Schuberth S, Brenner H. All-cause and cause specific mortality in a cohort of 20 000 construction workers; results from a 10 year follow up. Occup Environ Med 2004;61(5):419–425. 15090662.ArticlePubMedPMC
- 6. Söderberg M, Stattin M, Robroek SJ, Burdorf A, Järvholm B. Industry mobility and disability benefits in heavy manual jobs: a cohort study of Swedish construction workers. Scand J Work Environ Health 2021;47(3):217–223. 33165622.ArticlePubMedPMC
- 7. Stocks SJ, McNamee R, Carder M, Agius RM. The incidence of medically reported work-related ill health in the UK construction industry. Occup Environ Med 2010;67(8):574–576. 20647381.ArticlePubMed
- 8. van der Molen HF, de Vries SC, Stocks SJ, Warning J, Frings-Dresen MH. Incidence rates of occupational diseases in the Dutch construction sector, 2010-2014. Occup Environ Med 2016;73(5):350–352. 26940576.ArticlePubMed
- 9. Alicandro G, Bertuccio P, Sebastiani G, La Vecchia C, Frova L. Mortality among Italian male workers in the construction industry: a census-based cohort study. Eur J Public Health 2020;30(2):247–252. 31504442.ArticlePubMedPDF
- 10. Korean Statistical Information Service. Unit wages by job family. Updated 2022]. Accessed October 18, 2022]. https://kosis.kr/statHtml/statHtml.do?orgId=365&tblId=TX_36504_A001_1&vw_cd=MT_ETITLE&list_id=P1_2&scrId=&seqNo=&language=en&obj_var_id=&itm_id=&conn_path=A6&path=%252Feng%252Fsearch%252FsearchList.do .
- 11. Stocks SJ, Turner S, McNamee R, Carder M, Hussey L, Agius RM. Occupation and work-related ill-health in UK construction workers. Occup Med (Lond) 2011;61(6):407–415. 21752940.ArticlePubMed
- 12. Pettersson H, Olsson D, Järvholm B. Occupational exposure to noise and cold environment and the risk of death due to myocardial infarction and stroke. Int Arch Occup Environ Health 2020;93(5):571–575. 31915923.ArticlePubMedPMCPDF
- 13. Sauvé JF, Beaudry C, Bégin D, Dion C, Gérin M, Lavoué J. Silica exposure during construction activities: statistical modeling of task-based measurements from the literature. Ann Occup Hyg 2013;57(4):432–443. 23223272.PubMed
- 14. Blanc PD, Järvholm B, Torén K. Prospective risk of rheumatologic disease associated with occupational exposure in a cohort of male construction workers. Am J Med 2015;128(10):1094–1101. 26007670.ArticlePubMed
- 15. Jonsson E, Järvholm B, Andersson M. Silica dust and sarcoidosis in Swedish construction workers. Occup Med (Lond) 2019;69(7):482–486. 31504840.ArticlePubMedPMCPDF
- 16. Järvholm B, Aström E. The risk of lung cancer after cessation of asbestos exposure in construction workers using pleural malignant mesothelioma as a marker of exposure. J Occup Environ Med 2014;56(12):1297–1301. 25479300.ArticlePubMedPMC
- 17. Calvert GM, Luckhaupt S, Lee SJ, Cress R, Schumacher P, Shen R, et al. Lung cancer risk among construction workers in California, 1988-2007. Am J Ind Med 2012;55(5):412–422. 22237930.ArticlePubMed
- 18. Meding B, Wrangsjö K, Burdorf A, Järvholm B. Disability pensions due to skin diseases: a cohort study in Swedish construction workers. Acta Derm Venereol 2016;96(2):232–236. 26280897.ArticlePubMed
- 19. Järvholm B, Englund A. The impact of asbestos exposure in Swedish construction workers. Am J Ind Med 2014;57(1):49–55. 24108505.ArticlePubMed
- 20. Jackson JA, Olsson D, Punnett L, Burdorf A, Järvholm B, Wahlström J. Occupational biomechanical risk factors for surgically treated ulnar nerve entrapment in a prospective study of male construction workers. Scand J Work Environ Health 2019;45(1):63–72. 30132781.ArticlePubMed
- 21. Statistics Korea. 6th Korean Standard Classification of Occupations. Updated 2017]. Accessed October 18, 2022]. https://kssc.kostat.go.kr:8443/ksscNew_web/kssc/ccc/forwardPage.do?gubun=001_1# .
- 22. Statistics Korea. 9th Korean Standard Industrial Classification. Updated 2017]. Accessed October 18, 2022]. https://kssc.kostat.go.kr:8443/ksscNew_web/kssc/main/main.do?gubun=1# .
- 23. Construction Workers Mutual Aid Association. Construction worker skill class system. Accessed October 18, 2022]. https://cw.or.kr/plus/skill/system/introduction.do .
- 24. Cheol Seong S, Kim YY, Khang YH, Heon Park J, Kang HJ, Lee H, et al. Data resource profile: the National Health Information database of the National Health Insurance Service in South Korea. Int J Epidemiol 2017;46(3):799–800. 27794523.PubMed
- 25. National Health Insurance Sharing Service. What is customized health information data?. Accessed October 18, 2022]. http://nhiss.nhis.or.kr/bd/ab/bdaba032eng.do .
- 26. Jang TW, Kim HR, Lee HE, Myong JP, Koo JW, Ye BJ, et al. Overwork and cerebrocardiovascular disease in Korean adult workers. J Occup Health 2015;57(1):51–57. 25410266.ArticlePubMedPDF
- 27. Statistics Korea. The introduction page of Korean Standard Classification of Diseases. Accessed October 18, 2022]. http://kssc.kostat.go.kr/ksscNew_web/ekssc/common/selectIntroduce.do?part=2&top_menu=102&bbsId=icd_s&categoryNameCode=802&categoryMenu=001 .
- 28. Jung S, Kim TK, Kim YJ, Kim YK, Kang D, Kim SY. Epidemiology of occupational injuries in construction workers between 2009 and 2018 in South Korea. Am J Ind Med 2023;66(2):155–166. 36433706.ArticlePubMedPMCPDF
- 29. Arndt V, Rothenbacher D, Daniel U, Zschenderlein B, Schuberth S, Brenner H. Construction work and risk of occupational disability: a ten year follow up of 14,474 male workers. Occup Environ Med 2005;62(8):559–566. 16046609.ArticlePubMedPMC
- 30. Khosravi Y, Asilian-Mahabadi H, Hajizadeh E, Hassanzadeh-Rangi N, Bastani H, Behzadan AH. Factors influencing unsafe behaviors and accidents on construction sites: a review. Int J Occup Saf Ergon 2014;20(1):111–125. 24629873.ArticlePubMed
- 31. Kaur H, Wurzelbacher SJ, Bushnell PT, Grosch JW, Tseng CY, Scholl JC, et al. Workers’ compensation claim rates and costs for musculoskeletal disorders related to overexertion among construction workers - Ohio, 2007-2017. MMWR Morb Mortal Wkly Rep 2021;70(16):577–582. 33886534.ArticlePubMedPMC
- 32. Park JS, Park EK, Kim HK, Choi GS. Prevalence and risk factors of occupational skin disease in Korean workers from the 2014 Korean Working Conditions Survey. Yonsei Med J 2020;61(1):64–72. 31887801.ArticlePubMedPMCPDF
- 33. Aalto-Korte K, Koskela K, Pesonen M. Construction workers’ skin disorders in the Finnish Register of Occupational Diseases 2005-2016. Contact Dermat 2020;83(6):437–441.ArticlePDF
- 34. Torén K, Järvholm B. Effect of occupational exposure to vapors, gases, dusts, and fumes on COPD mortality risk among Swedish construction workers: a longitudinal cohort study. Chest 2014;145(5):992–997. 24264472.ArticlePubMed
- 35. Dement JM, Welch LS, Ringen K, Cranford K, Quinn P. Longitudinal decline in lung function among older construction workers. Occup Environ Med 2017;74(10):701–708. 28515054.ArticlePubMed
- 36. Dement JM, Cloeren M, Ringen K, Quinn P, Chen A, Cranford K, et al. COPD risk among older construction workers-updated analyses 2020. Am J Ind Med 2021;64(6):462–475. 33728649.ArticlePubMedPDF
- 37. Sekhavati E, Yengejeh RJ. Particulate matter exposure in construction sites is associated with health effects in workers. Front Public Health 2023;11:1130620. 36960377.ArticlePubMedPMC
- 38. Wada K, Eguchi H, Prieto-Merino D. Differences in stroke and ischemic heart disease mortality by occupation and industry among Japanese working-aged men. SSM Popul Health 2016;2:745–749. 29349185.ArticlePubMedPMC
- 39. Tannis C, Chernov C, Perlman S, McKelvey W, Toprani A. Cardiovascular health risk behaviors by occupation in the NYC Labor Force. J Occup Environ Med 2020;62(9):757–763. 32890215.ArticlePubMed
- 40. Chung JW, Wong BY, Yan VC, Chung LM, So HC, Chan A. Cardiovascular health of construction workers in Hong Kong: a cross-sectional study. Int J Environ Res Public Health 2018;15(6):1251. 29895813.ArticlePubMedPMC
- 41. Thabit H, Burns N, Shah S, Brema I, Crowley V, Finnegan F, et al. Prevalence and predictors of diabetes and cardiometabolic risk among construction workers in Ireland: the Construction Workers Health Trust screening study. Diab Vasc Dis Res 2013;10(4):337–345. 23624762.ArticlePubMedPDF
- 42. Ghimire R, Neupane GP. Prevalent health problems among Nepalese underground construction workers. J Environ Public Health 2020;2020:9436068. 33488740.ArticlePubMedPMCPDF
- 43. Torén K, Bergdahl IA, Nilsson T, Järvholm B. Occupational exposure to particulate air pollution and mortality due to ischaemic heart disease and cerebrovascular disease. Occup Environ Med 2007;64(8):515–519. 17303673.ArticlePubMedPMC
- 44. Berhanu F, Gebrehiwot M, Gizaw Z. Workplace injury and associated factors among construction workers in Gondar town, Northwest Ethiopia. BMC Musculoskelet Disord 2019;20(1):523. 31706352.ArticlePubMedPMCPDF
REFERENCES
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Work-Related Asthma: An Occupational Medicine Perspective
Yangwoo Kim, Inah Kim, Jaechul Song
Allergy, Asthma & Immunology Research.2026; 18(3): 323. CrossRef - Occupational disease monitoring by the Korea Occupational Disease
Surveillance Center: a narrative review
Dong-Wook Lee, Inah Kim, Jungho Hwang, Sunhaeng Choi, Tae-Won Jang, Insung Chung, Hwan-Cheol Kim, Jaebum Park, Jungwon Kim, Kyoung Sook Jeong, Youngki Kim, Eun-Soo Lee, Yangwoo Kim, Inchul Jeong, Hyunjeong Oh, Hyeoncheol Oh, Jea Chul Ha, Jeehee Min, Chul
The Ewha Medical Journal.2025;[Epub] CrossRef - A systematic review and meta-analysis on the prevalence and demographic risk factors of work-related musculoskeletal disorders in construction workers
Weiner Santos, Alejandro Lorente, Carmen Rojas, Rui Isidoro, Ana Dias, Gonzalo Mariscal, Ahmed Hamdy Zabady, Rafael Lorente
Frontiers in Public Health.2025;[Epub] CrossRef - Work Performance Among Workers without Disabilities after Industrial Accidents: A Longitudinal Study
Chong Min Hong
The Open Public Health Journal.2024;[Epub] CrossRef
 Cite
CiteIncidence rates of injury, musculoskeletal, skin, pulmonary and chronic diseases among construction workers by classification of occupations in South Korea: a 1,027 subject-based cohort of the Korean Construction Worker’s Cohort (KCWC)

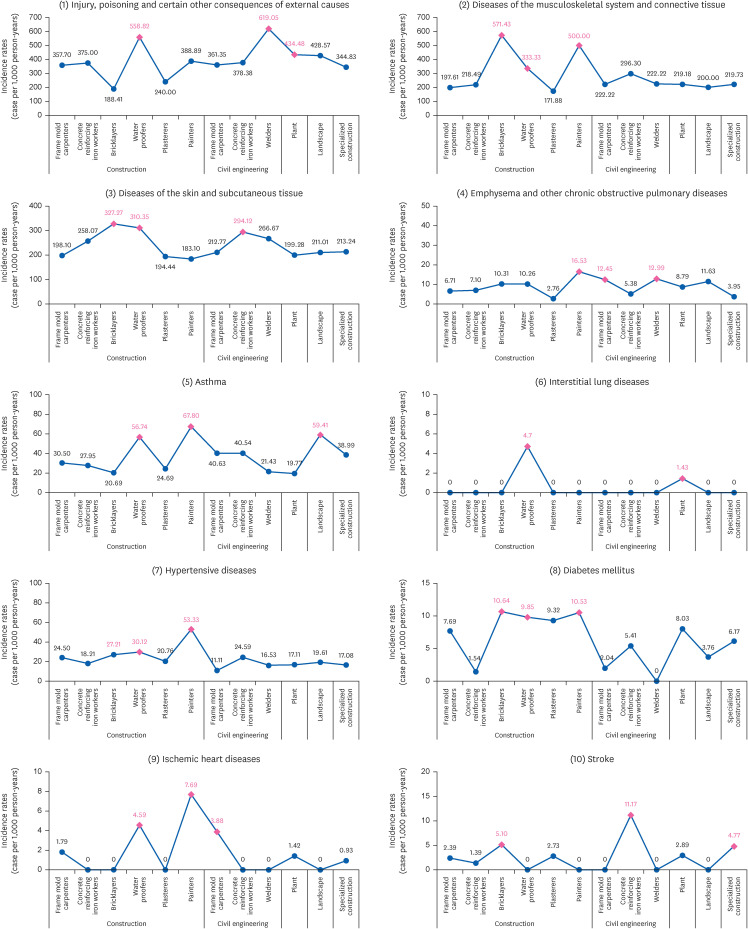
Fig. 1 Subject-based cohort study design in Korean Construction Worker’s Cohort. Example of a new onset disease in 2010 in a person who started working in construction industry since 2005.
Fig. 2 Target disease incidence rates based on classification of occupations of the subject-based cohort in Korean Construction Worker’s Cohort.
Fig. 1
Fig. 2
Incidence rates of injury, musculoskeletal, skin, pulmonary and chronic diseases among construction workers by classification of occupations in South Korea: a 1,027 subject-based cohort of the Korean Construction Worker’s Cohort (KCWC)
| Variable | Total (n = 1,027) | Male (n = 949) | Female (n = 78) | |||||
|---|---|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | |||
| Age (years) | ||||||||
| Mean ± SD | 59.3 ± 8.9 | 59.2 ± 9.0 | 61.1 ± 6.9 | 0.022*a | ||||
| < 30 | 9 | 0.9 | 8 | 0.8 | 1 | 1.3 | 0.512b | |
| 30–39 | 28 | 2.7 | 27 | 2.8 | 1 | 1.3 | ||
| 40–49 | 110 | 10.7 | 102 | 10.7 | 8 | 10.3 | ||
| 50–59 | 256 | 24.9 | 241 | 25.4 | 15 | 19.2 | ||
| 60–69 | 530 | 51.6 | 488 | 51.4 | 42 | 53.4 | ||
| ≥ 70 | 94 | 9.2 | 83 | 8.7 | 11 | 14.1 | ||
| Smoking | < 0.001***b | |||||||
| Smoker | 845 | 82.3 | 839 | 88.4 | 6 | 7.7 | ||
| Non-smoker | 182 | 17.7 | 110 | 11.6 | 72 | 92.3 | ||
| Body mass index (kg/m2) | 0.021*b | |||||||
| Under weight (< 18.5) | 19 | 1.8 | 14 | 1.5 | 5 | 6.4 | ||
| Normal weight (≥ 18.5, < 25.0) | 734 | 71.5 | 681 | 71.8 | 53 | 67.9 | ||
| Over weight (≥ 25.0, < 30.0) | 258 | 25.1 | 239 | 25.2 | 19 | 24.4 | ||
| Obesity (≥ 30.0) | 16 | 1.6 | 15 | 1.6 | 1 | 1.3 | ||
| Construction businesses | < 0.001***b | |||||||
| Construction | 664 | 64.7 | 608 | 64.1 | 56 | 71.8 | ||
| Civil engineering | 142 | 13.8 | 137 | 14.4 | 5 | 6.4 | ||
| Plant | 72 | 7.0 | 66 | 7.0 | 6 | 7.7 | ||
| Landscape | 29 | 2.8 | 20 | 2.1 | 9 | 11.5 | ||
| Specialized construction | 120 | 11.7 | 118 | 12.4 | 2 | 2.6 | ||
| Work duration in construction industry (years) | ||||||||
| Mean ± Standard deviation | 19.2±13.1 | 19.9±13.2 | 11.4±8.7 | 0.001**a | ||||
| Beginner (< 3 years) | 99 | 9.6 | 80 | 8.4 | 19 | 24.4 | < 0.001***b | |
| Intermediate (≥ 3, < 9 years) | 180 | 17.5 | 164 | 17.3 | 16 | 20.5 | ||
| Advanced (≥ 9, < 21 years) | 328 | 31.9 | 299 | 31.5 | 29 | 37.2 | ||
| Expert (≥ 21 years) | 420 | 40.9 | 406 | 42.8 | 14 | 17.9 | ||
| Disease | KCD-7 | Sex | Mean follow-up period (years) | Number of events | Total person-years | Incidence rates (per 1,000 person-years) |
|---|---|---|---|---|---|---|
| Total cancer | C00-097 | Total | 10.14 | 46 | 10,167 | 4.52 |
| Male | 41 | 9,509 | 4.31 | |||
| Female | 5 | 658 | 7.60 | |||
| Injury, poisoning, and certain other consequences of external causes | S00-T98 | Total | 2.62 | 907 | 2,636 | 344.08 |
| Male | 841 | 2,472 | 340.21 | |||
| Female | 66 | 164 | 402.44 | |||
| Diseases of the musculoskeletal system and connective tissue | M00-99 | Total | 4.27 | 425 | 2,037 | 208.64 |
| Male | 414 | 2,002 | 206.79 | |||
| Female | 11 | 35 | 314.29 | |||
| Diseases of the skin and subcutaneous tissue | L00-99 | Total | 4.10 | 816 | 4,124 | 197.87 |
| Male | 749 | 3,949 | 189.67 | |||
| Female | 67 | 175 | 382.86 | |||
| Allergic contact dermatitis | L23 | Total | 6.90 | 532 | 6,940 | 76.66 |
| Male | 484 | 6,566 | 73.71 | |||
| Female | 48 | 374 | 128.34 | |||
| Irritant contact dermatitis | L24 | Total | 9.29 | 193 | 9,344 | 20.66 |
| Male | 174 | 8,768 | 19.85 | |||
| Female | 19 | 576 | 32.99 | |||
| Undifferentiated contact dermatitis | L25 | Total | 9.62 | 136 | 9,676 | 14.06 |
| Male | 126 | 9,058 | 13.91 | |||
| Female | 10 | 618 | 16.18 | |||
| Emphysema and other chronic obstructive pulmonary diseases | J43-44 (Except J43.0) | Total | 10.03 | 66 | 9,969 | 6.62 |
| Male | 63 | 9,302 | 6.77 | |||
| Female | 3 | 667 | 4.50 | |||
| Asthma | J45-46 | Total | 9.05 | 242 | 8,430 | 28.71 |
| Male | 226 | 7,982 | 28.31 | |||
| Female | 16 | 448 | 35.71 | |||
| Interstitial lung diseases | J84 | Total | 10.35 | 3 | 10,414 | 0.29 |
| Male | 3 | 9,727 | 0.31 | |||
| Female | 0 | 687 | 0.00 | |||
| Hypertensive diseases | I10-13, I15 | Total | 9.35 | 150 | 8,235 | 18.22 |
| Male | 140 | 7,714 | 18.15 | |||
| Female | 10 | 521 | 19.19 | |||
| Diabetes mellitus | E10-14 | Total | 10.07 | 53 | 9,262 | 5.72 |
| Male | 51 | 8,667 | 5.88 | |||
| Female | 2 | 595 | 3.36 | |||
| Ischemic heart diseases | I20-25 | Total | 10.30 | 18 | 10,324 | 1.74 |
| Male | 17 | 9,646 | 1.76 | |||
| Female | 1 | 678 | 1.48 | |||
| Stroke | I60-69 | Total | 10.26 | 27 | 10,272 | 2.63 |
| Male | 26 | 9,585 | 2.71 | |||
| Female | 1 | 687 | 1.46 |
| Classifications of occupations | Diseases and diagnostic codes, incidence rates for diseases (per 1,000 person-years) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Injury, poisoning, and certain other consequences of external causes | Diseases of the musculoskeletal system and connective tissue | Diseases of the skin and subcutaneous tissue | Emphysema and other chronic obstructive pulmonary diseases | Asthma | Interstitial lung diseases | Hypertensive diseases | Diabetes mellitus | Ischemic heart diseases | Stroke | ||
| S00-T98 | M00-99 | L00-99 | J43-44 (Except J43.0) | J45-46 | J84 | I10-13, I15 | E10-14 | I20-25 | I60-69 | ||
| Construction | |||||||||||
| Frame mold carpenters | 357.70 | 197.61 | 198.10 | 6.71 | 30.50 | 0.00 | 24.50 | 7.69 | 1.79 | 2.39 | |
| Concrete reinforcing iron workers | 375.00 | 218.49 | 258.07 | 7.10 | 27.95 | 0.00 | 18.21 | 1.54 | 0.00 | 1.39 | |
| Bricklayers | 188.41 | 571.43a | 327.27a | 10.31 | 20.69 | 0.00 | 27.21a | 10.64a | 0.00 | 5.10a | |
| Water proofers | 558.82a | 333.33a | 310.35a | 10.26 | 56.74a | 4.70a | 30.12a | 9.85a | 4.59a | 0.00 | |
| Plasterers | 240.00 | 171.88 | 194.44 | 2.76 | 24.69 | 0.00 | 20.76 | 9.32 | 0.00 | 2.73 | |
| Painters | 388.89 | 500.00a | 183.10 | 16.53a | 67.80a | 0.00 | 53.33a | 10.53a | 7.69a | 0.00 | |
| Civil engineering | |||||||||||
| Frame mold carpenters | 361.35 | 222.22 | 212.77 | 12.45a | 40.63 | 0.00 | 11.11 | 2.04 | 3.88a | 0.00 | |
| Concrete reinforcing iron workers | 378.38 | 296.30 | 294.12a | 5.38 | 40.54 | 0.00 | 24.59 | 5.41 | 0.00 | 11.17a | |
| Welders | 619.05a | 222.22 | 266.67 | 12.99a | 21.43 | 0.00 | 16.53 | 0.00 | 0.00 | 0.00 | |
| Plant | 434.48a | 219.18 | 199.28 | 8.79 | 19.77 | 1.43a | 17.11 | 8.03 | 1.42 | 2.89 | |
| Landscape | 428.57 | 200.00 | 211.01 | 11.63 | 59.41a | 0.00 | 19.61 | 3.76 | 0.00 | 0.00 | |
| Specialized construction | 344.83 | 219.73 | 213.24 | 3.95 | 38.99 | 0.00 | 17.08 | 6.17 | 0.93 | 4.77a | |
Table 1 Socio-demographic and occupational characteristics of the subject-based cohort in Korean Construction Worker’s Cohort
Current and ex-smokers are both classified as smokers. The
*
aThe
bThe
Table 2 Mean follow-up period and targeted disease incidence rates of the subject-based cohort in Korean Construction Worker’s Cohort
KCD-7: seventh revision of the Korean Classification of Diseases.
Table 3 Targeted disease incidence rates based on classification of occupations of the subject-based cohort in Korean Construction Worker’s Cohort
aTop 3 occupations for each target disease.

