
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 34; 2022 > Article
- Case Report A case report of toxic hepatitis caused by chloroform in automotive parts manufacturer coating process
-
Jong Hyun Hwang1
 , Jung Il Kim2
, Jung Il Kim2 -
Annals of Occupational and Environmental Medicine 2022;34:e22.
DOI: https://doi.org/10.35371/aoem.2022.34.e22
Published online: August 29, 2022
1Department of Occupational and Environmental Medicine, Dong-A University Hospital, Busan, Korea.
2Department of Occupational and Environmental Medicine, College of Medicine, Dong-A University, Busan, Korea.
- Correspondence: Jung Il Kim. Department of Occupational and Environmental Medicine, College of Medicine, Dong-A University, 32 Daesingongwon-ro, Seo-gu, Busan 49201, Korea. kimji@dau.ac.kr
• Received: July 15, 2022 • Revised: August 17, 2022 • Accepted: August 26, 2022
Copyright © 2022 Korean Society of Occupational & Environmental Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background Several cases of chloroform-induced hepatotoxicity have been reported worldwide, but only 2 cases have been reported in Korea. We encountered a case of toxic hepatitis due to chloroform exposure in February 2022 and report the diagnosis process and clinical findings.
-
Case presentation A 38-year-old employee in charge of the coating after washing (degreasing) at an automotive parts manufacturer complained of jaundice and was diagnosed with acute toxic hepatitis. After the initial diagnosis, he continued to work, his symptoms worsened, and he was hospitalized for 8 days. Liver ultrasonography (elastography) revealed acute hepatitis. The washing agent contained chloroform, which was not listed on the materials safety data sheet, and the concentrations of chloroform in the workplace were up to 4.7 times the time-weighted average.
-
Conclusions This patient showed typical toxic hepatitis with chloroform; further follow-up studies are required. Both employers and workers should be aware of information on toxic substances and take precautions to avoid exposure.
BACKGROUND
Chloroform (trichloromethane, CHCl3) is a clear volatile liquid with a pleasant etheric odor. Chloroform is being gradually replaced by a safe substance due to its carcinogenicity (International Agency for Research on Cancer grade 2B) and toxicity,1 but it is still used in various ways throughout the industry and is mostly used as the main raw material for chlorinated polymers of chlorodifluoromethane (HCFC-22). It is also used in pesticides, fat, oil, rubber, alkaloids, waxes, gutta-percha, resins, fire extinguishers, and in the rubber industry.2
Chloroform is well absorbed mainly through the respiratory tract, ingestion, and dermal exposure and is excreted, exhaled, or metabolized to carbon dioxide in the liver. The target organs of chloroform are the central nervous system, the liver, and the kidneys. When exposed to high concentrations for a short period, patients present with central nervous system toxicity, while chronic exposure causes liver and kidney toxicity. Most chloroform toxicity results from inhalation exposure, and few reports have included oral intake.3
Toxic hepatitis caused by chloroform has been reported in a few cases worldwide,4,5,6,7 and only 2 cases have been reported in Korea.8,9 In February 2022, a patient with jaundice visited our hospital in Busan and was finally diagnosed with chloroform-induced toxic hepatitis. We report in detail the exposure route, diagnostic process, and clinical features of this patient.
CASE PRESENTATION
A 38-year-old man who had been working in an automotive parts manufacturing plant for 5 years developed jaundice in the middle of January 2022.
The patient visited a local hospital on January 28, 2022. The patient’s aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels were very high (AST 1,140 IU/L, ALT 2,650 IU/L), gamma glutamyl transpeptidase was 215 IU/L, and total bilirubin (TB) and direct bilirubin (DB) were 9.41 mg/dL and 6.77 mg/dL, respectively. Abdominal computed tomography revealed acute hepatitis with mild hepatosplenomegaly (Fig. 1). The patient was immediately transferred to the department of gastroenterology for further evaluation and treatment.

The patient had not recently taken hepatotoxic medications such as herbal medicines, antifungal drugs, anti-tuberculosis drugs, or anti-inflammatory drugs and did not have a history of drug allergies. He had no specific familial or genetic problems and had never smoked. He drank a bottle of soju twice per week. He was diagnosed with acute hepatitis; however, the exact cause of hepatitis was not identified. The patient’s general condition was tolerable; therefore, he was treated on an outpatient basis. Though he was diagnosed with acute hepatitis, he continued to work until hospitalization.
One week later, on February 4th, the patient visited the hospital for follow-up treatment. The jaundice improved and there were no other symptoms. In addition, the liver enzyme values showed a tendency to decrease (AST 662 IU/L, ALT 482 IU/L, TB 5.5 mg/dL, DB 2.7 mg/dL).
He visited the department of occupational and environmental medicine of the same hospital on February 9th. The patient reported that his condition was tolerable and jaundice and other symptoms continued to improve.
On February 15th, during an outpatient examination, the patient reported that abdominal discomfort and jaundice had recurred 4–5 days earlier. He was hospitalized in the gastroenterology department due to poor general condition and increased liver enzymes (AST 937 IU/L, ALT 409 IU/L, TB 18.8 mg/dL, DB 9.9 mg/dL). The complete blood count was normal, and coagulation factors were also normal (prothrombin time 23.3 seconds, prothrombin time/international normalized ratio 2.00, 32.7%, and activated partial thromboplastin time 41.4 seconds). Antibody tests were performed to exclude viral and autoimmune hepatitis, and the results were as follows: anti-HAV IgG (−), anti-HAV IgM (−), HBs Ag (−), anti-HCV (−), HIV Ag/Ab (−), ANA (IF) (1:320 dilution), anti-smooth muscle Ab (−), ANCA (−), AMA (−), anti-LKM Ab (−), and anti-dsDNA IgG (20.6, within normal range). Abdominal ultrasonography findings were compatible with acute hepatopathy and reactive gallbladder wall thickening. For a more accurate differentiation of acute hepatitis, elastography was performed. The mean shear wave velocity was 3.26 ± 0.24 m/s, suggesting stage 4 fibrosis (> 1.86 m/s) (Fig. 2). Although stage 4 fibrosis indicates liver cirrhosis, it was determined to be a change due to acute inflammatory findings based on the clinical correlation with other symptoms and test results. The laboratory findings during the hospitalization period are summarized in Table 1. The patient’s general condition and liver function were restored after hydration and conservative treatment. He was discharged on the 8th day of hospitalization. The AST and ALT levels 20 days after discharge were 33 and 13 IU/L, respectively.
Fig. 2
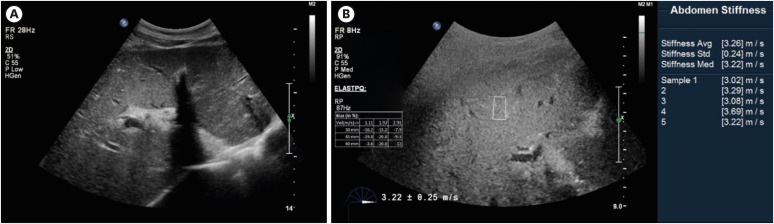
Abdominal ultrasonography. (A) The liver shows diffuse decreased parenchymal echogenicity with prominent portal venular wall echogenicity. The gallbladder shows diffuse wall edema. (B) Elastography: the mean shear wave velocity was 3.26 ± 0.24 m/s.
Table 1
Summary of biochemical analysis of patient by date
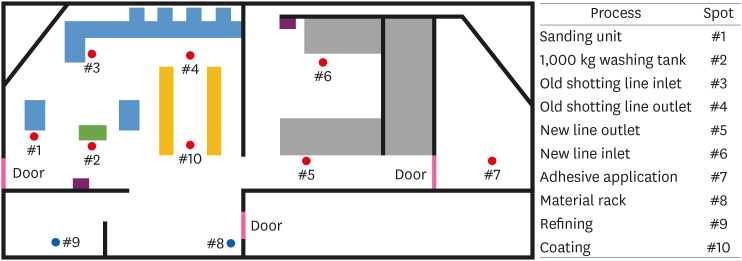
On February 9th, the patient visited the occupational and environmental medicine department for consultation regarding occupational accidents. The patient’s liver function was normal during regular health check-ups conducted in May 2021. The patient worked for an automotive parts manufacturer that produced powertrain mounting products, chassis, hoses, and dampers. He had worked on coating using organic solvents on spot 10 in Fig. 3 since June 2016, and he always wore the provided personal protective equipment including respirator, gloves and apron while working. He worked two shifts. The two groups worked in shifts at weekly intervals and worked five days a week. The day shift was from 8 am to 8 pm, and the night shift was from 8 pm to 8 am the next day. His actual working time during a 12-hour shift was 10 hours 40 minutes and the remaining time was used for meals and rest (50 minutes for lunch and 30 minutes for dinner, including the time for rest). The main process consists of six parts: sanding, shotting, washing, coating, refining, and adhesive application. After washing the manufactured goods, the patient worked on the coating part. Organic solvents are mainly used in washing and coating processes. The patient reported that the residues of the washing agent used in the washing process were almost always present in the coating process. In addition, some solvents were changed a month before the onset of jaundice (December 2021). The patient showed us several material safety data sheets (MSDSs), but none of them showed hepatotoxicity. He said that the material had recently changed, but he did not see the data. He promised to bring it to the next visit, but he was hospitalized five days later.
The Ministry of Employment and Labor conducted the workplace inspections. As a result of analyzing the sample for the washing agent, it was found that it contained chloroform, which was not mentioned in the MSDS, and the content was very high (28%–38%). A time-weighted average (TWA) was used to measure the workplace environment, and 8 individual samples and 2 area samples were analyzed. The measurement time was approximately 360 minutes. They reported that the washing agent contained chloroform, and that concentrations in the workplace were up to 4.7 times the TWA when corrected (based on the Korean occupational exposure limit; 10 ppm for 8 hours TWA). However, as workers worked more than 8 hours in this case, it was necessary to calculate the corrected exposure limit according to actual working hours (7.5 ppm for 10 hours 40 minutes TWA). It has been determined to be the main cause of toxic hepatitis.
Consent for publication of this case report and any accompanying data was obtained from the study participant on July 1, 2022. This study was approved by the Institutional Review Board of Dong-A University Hospital (DAUHIRB-22-134).
DISCUSSION AND CONCLUSION
We report a case of toxic hepatitis caused by exposure to chloroform in an automotive parts manufacturing facility. The patient was hospitalized for increased liver enzyme levels and general weakness. He was diagnosed with toxic hepatitis by laboratory tests and ultrasonography (elastography), but the cause was unknown. The Ministry of Employment and Labor conducted workplace investigations and announced that chloroform, which could cause hepatotoxicity, was detected and that the MSDS was mislabeled. Of 470 employees at the company, 94 workers who appeared to be exposed to the same washing agent were examined for medical checks. Thirteen employees, including this case, were diagnosed with toxic hepatitis. All of them were restricted from work.
The toxic effects of chloroform on the liver are well known.3 It can undergo both oxidative and reductive metabolism, depending on oxygen and substrate concentration. At low levels, chloroform is primarily converted to phosgene by CYP2E1. When the CYP2E1-mediated reaction is saturated, the predominant role in phosgene production is for CYP2A6 that is efficient even in highly hypoxic conditions and only at high substrate concentrations. The phosgene produced by chloroform bind to hepatocellular glutathione and depletes it, preventing its reaction with the reactive metabolites. As a result, it may cause hepatocellular steatosis and necrosis.10
Since most of the chemicals used throughout the industry are detoxified by the liver, various substances other than chloroform can cause toxic hepatitis.11 Although workers’ awareness of health and environmental issues has improved and attempts have been made to replace various hazardous substances with safe substances gradually,12 the potential threat of abnormal exposure, where many substances are still used, will not disappear completely.
Table 2 summarizes the occupational liver diseases reported in the Annals of Occupational and Environmental Medicine until recently.8,9,13,14,15,16,17,18 Cases of toxic hepatitis caused by various xlink:types of organic solvents were reported in Korea, and there were 2 cases of toxic hepatitis caused by chloroform. The first reported case was suspected chloroform-induced hepatotoxicity in a laboratory engineer in 2012,8 and the second case was hepatotoxicity of the 2 patients who worked in the clean room at a medical endoscopic manufacturer in 2014.9
Table 2
Occupational liver diseases reported in the Annals of Occupational and Environmental Medicine
| Exposed chemicals | Year | Number of patients | Diagnosis | Ultrasonography | Elastography | CT | Biopsy |
|---|---|---|---|---|---|---|---|
| Trichloroethylene13 | 1999 | 1 | Toxic hepatitis, exfoliative dermatitis | Enhanced intrahepatic echo | - | - | - |
| Dimethylacetamide14 | 2000 | 7 | Toxic hepatitis | Normal | - | - | - |
| Methylene Chloride15 | 2003 | 1 | Toxic hepatitis | Enhanced intrahepatic echo, GB wall thickening | - | Enhanced echo, hepatomegaly, GB wall thickening | - |
| Dimethylformamide16 | 2003 | 1 | Toxic hepatitis | Diffuse hepatocellular disease | - | - | - |
| Trichloroethylene17 | 2005 | 3 | Toxic hepatitis, Stevens-Johnson syndrome | Hepatomegaly | - | - | Hepatocellular necrosis, intracellular cholestasis, ballooning degeneration |
| Chloroform8 | 2010 | 1 | Toxic hepatitis | - | - | Normal | - |
| Chloroform9 | 2014 | 2 | Toxic hepatitis | Normal | - | - | - |
| Mild fatty liver | |||||||
| HCFC-12318 | 2017 | 2 | Toxic hepatitis | - | - | - | Portal and panlobular infiltration of mixed inflammatory cells, multifocal spotty and confluent necrosis, minimal macrovesicular and microvesicular steatosis |
The authors experienced only one case; however, this accident was the first large-scale exposure to chloroform in Korea. Of course, an MSDS with accurate substance labeling must be provided in the workplace, and even if a patient suspected of poisoning does not present with a reasonable MSDS, occupational and environmental medicine physicians must always be alert to potential toxic exposure. Moreover, although the solvent was changed, the employer did not properly provide MSDS for the changed substance and did not provide health education. This incident would not have occurred if the workplace had followed the basic rules. In conclusion, this is a rare case report of toxic hepatitis induced by chloroform. At the same time, it suggests the importance of accurate information delivery of chemicals and appropriate health education for the people who deal with it.
Abbreviations
AST
aspartate aminotransferase
ALT
alanine aminotransferase
CT
computed tomography
DB
direct bilirubin
GB
gallbladder
γ-GTP
gamma glutamyl transpeptidase
HAV
hepatitis A virus
IgG
immunoglobulin G
INR
international normalized ratio
MSDS
material safety data sheet
PT
prothrombin time
SWV
shear wave velocity
TB
total bilirubin
TWA
time-weighted average
-
Competing interests: The authors declare that they have no competing interests.
-
Author contributions:
NOTES
- 1. Komulainen H. Experimental cancer studies of chlorinated by-products. Toxicology 2004;198(1-3):239–248. 15138047.ArticlePubMed
- 2. Watts P, Long G, Meek ME. Concise international chemical assessment document; 58. Updated 2004]. Accessed July 3, 2022]. https://inchem.org/documents/cicads/cicads/cicad58.htm .
- 3. Brautbar N, Williams J 2nd. Industrial solvents and liver toxicity: risk assessment, risk factors and mechanisms. Int J Hyg Environ Health 2002;205(6):479–491. 12455270.ArticlePubMed
- 4. Bomski H, Sobolewska A, Strakowski A. Toxische schädigung der leber durch chloroform bei chemiebetriebswerkern. Int Arch Gewerbepathol Gewerbehyg 1967;24(2):127–134.ArticlePDF
- 5. Bai C, Canfield PJ, Stacey NH. Individual serum bile acids as early indicators of carbon tetrachloride- and chloroform-induced liver injury. Toxicology 1992;75(3):221–234. 1455431.ArticlePubMed
- 6. Gambini G, Farina G. Hepatic function in workers exposed to inhalation of chloroform vapors. Med Lav 1973;64(11):432–436. 4793806.PubMed
- 7. Phoon WH, Goh KT, Lee LT, Tan KT, Kwok SF. Toxic jaundice from occupational exposure to chloroform. Med J Malaysia 1983;38(1):31–34. 6633331.PubMed
- 8. Lee DG, Lee CH, Jang KH, Chae HJ, Moon JD. A suspicious case of chloroform induced acute toxic hepatitis in laboratory worker. Korean J Occup Environ Med 2012;24(3):304–310.ArticlePDF
- 9. Kang YJ, Ahn J, Hwang YI. Acute liver injury in two workers exposed to chloroform in cleanrooms: a case report. Ann Occup Environ Med 2014;26(1):49. 25411642.ArticlePubMedPMCPDF
- 10. Gemma S, Vittozzi L, Testai E. Metabolism of chloroform in the human liver and identification of the competent P450s. Drug Metab Dispos 2003;31(3):266–274. 12584152.ArticlePubMed
- 11. Malaguarnera G, Cataudella E, Giordano M, Nunnari G, Chisari G, Malaguarnera M. Toxic hepatitis in occupational exposure to solvents. World J Gastroenterol 2012;18(22):2756–2766. 22719183.ArticlePubMedPMC
- 12. Clark JH, Tavener SJ. Alternative solvents: shades of green. Org Process Res Dev 2007;11(1):149–155.Article
- 13. Chae HJ, Lee SK, Lee KJ, Kim JY, Lee SC, Shin DH, et al. Exfoliative dermatitis and toxic hepatitis associated with occupational exposure to trichloroethylene. Korean J Occup Environ Med 2003;15(1):111–117.ArticlePDF
- 14. Choi TS, Woo KH, Kim JS, Park WS, Ham JH, Jung SJ, et al. Toxic hepatitis induced by occupational dimethylacetamide exposure. Korean J Occup Environm Med 2001;13(2):164–170.ArticlePDF
- 15. Ha BG, Kim JS, Yu JY, Woo KH, Ham JO, Yoon SY, et al. A case of toxic hepatitis in a worker exposed to a cleansing agent mainly composed of methylene chloride. Korean J Occup Environ Med 2004;16(2):210–219.ArticlePDF
- 16. Roh JR, Sohn JG, Kim JH, Park SJ. A case of acute toxic hepatitis induced by brief exposure to dimethylformamide. Korean J Occup Environ Med 2005;17(2):144–148.ArticlePDF
- 17. Lee SW, Kim EA, Kim DS, Koh DH, Kang SK, Kim BK, et al. Exposure level of trichloroethylene in Stevens-Johnson syndrome due to occupational exposure: 3 case reports and a review of other cases. Korean J Occup Environ Med 2008;20(2):132–146.ArticlePDF
- 18. Shin MY, Park JS, Park HD, Lee J. HCFC-123-induced toxic hepatitis and death at a Korean fire extinguisher manufacturing facility: a case series. Ann Occup Environ Med 2018;30(1):20. 29610668.ArticlePubMedPMCPDF
REFERENCES
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Hepatoprotective Potential of Indian Medicinal Plants
Arti Kumari, Nisha Chandila, Rubina Bhutani, Inderjeet Yadav
Combinatorial Chemistry & High Throughput Screening.2026; 29(3): 387. CrossRef - Occupational disease monitoring by the Korea Occupational Disease
Surveillance Center: a narrative review
Dong-Wook Lee, Inah Kim, Jungho Hwang, Sunhaeng Choi, Tae-Won Jang, Insung Chung, Hwan-Cheol Kim, Jaebum Park, Jungwon Kim, Kyoung Sook Jeong, Youngki Kim, Eun-Soo Lee, Yangwoo Kim, Inchul Jeong, Hyunjeong Oh, Hyeoncheol Oh, Jea Chul Ha, Jeehee Min, Chul
The Ewha Medical Journal.2025;[Epub] CrossRef - Morbidity of aircraft workers with temporary disability
Olga A. Molchanova, Olga G. Bogdanova, Vladimir A. Pankov, Mikhail Yu. Itygilov
Hygiene and sanitation.2023; 102(8): 836. CrossRef
 Cite
CiteA case report of toxic hepatitis caused by chloroform in automotive parts manufacturer coating process

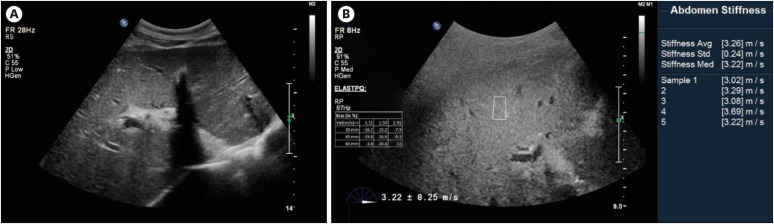
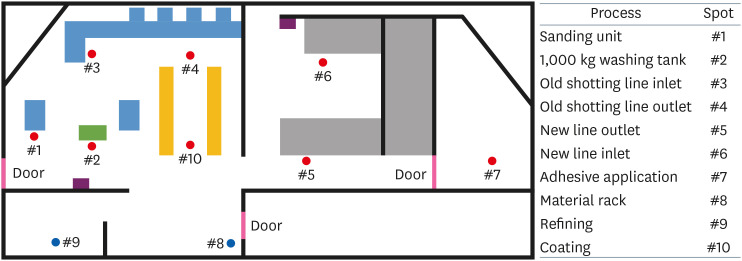
Fig. 1 Abdominal computed tomography shows acute hepatitis with mild hepatosplenomegaly.
Fig. 2 Abdominal ultrasonography. (A) The liver shows diffuse decreased parenchymal echogenicity with prominent portal venular wall echogenicity. The gallbladder shows diffuse wall edema. (B) Elastography: the mean shear wave velocity was 3.26 ± 0.24 m/s.
Fig. 3 Schematic diagram of workplace.
Fig. 1
Fig. 2
Fig. 3
A case report of toxic hepatitis caused by chloroform in automotive parts manufacturer coating process
| Date | 22.1.28a | 22.2.4 | 22.2.15 | 22.2.16b | 22.2.17 | 22.2.18 | 22.2.19 | 22.2.20 | 22.2.22 | 22.2.28c | 22.3.15 | Reference range |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total protein (g/dL) | 7.1 | 7.3 | - | - | 5.6 | - | - | 5.1 | 6.1 | 7.1 | - | 6.6–8.3 |
| Albumin (g/dL) | 4.5 | 4.4 | - | 3.9 | 3.3 | 3.1 | 3.1 | 3.0 | 3.7 | 3.8 | - | 3.5–5.2 |
| Total bilirubin (mg/dL) | 9.41 | 5.5 | 18.8 | 21.9 | 24.0 | 24.5 | 24.7 | 23.7 | 22.4 | 11.7 | 5.1 | 0.2–1.2 |
| Direct bilirubin (mg/dL) | 6.77 | 2.7 | 9.9 | 12.9 | 13.4 | 13.9 | 14.0 | 13.6 | 12.1 | 5.4 | 2.2 | 0.0–0.4 |
| AST (IU/L) | 1,140 | 662 | 937 | 1,324 | 1,106 | 756 | 567 | 387 | 240 | 107 | 31 | 0–40 |
| ALT (IU/L) | 2,650 | 482 | 409 | 451 | 408 | 367 | 324 | 269 | 228 | 83 | 13 | 0–40 |
| γ-GTP (IU/L) | 215 | 99 | 88 | - | 79 | 77 | 75 | 70 | 68 | 53 | - | 9–64 |
| PT (seconds) | 13.6 | 13.9 | - | 23.3 | 25.4 | 25.1 | 24.2 | 23.0 | 18.3 | 14.6 | 13.7 | 10.8–14.0 |
| PT (INR) | 1.23 | 1.18 | - | 2.00 | 2.19 | 2.16 | 2.08 | 1.98 | 1.56 | 1.24 | 1.16 | 0.85–1.20 |
| Exposed chemicals | Year | Number of patients | Diagnosis | Ultrasonography | Elastography | CT | Biopsy |
|---|---|---|---|---|---|---|---|
| Trichloroethylene | 1999 | 1 | Toxic hepatitis, exfoliative dermatitis | Enhanced intrahepatic echo | - | - | - |
| Dimethylacetamide | 2000 | 7 | Toxic hepatitis | Normal | - | - | - |
| Methylene Chloride | 2003 | 1 | Toxic hepatitis | Enhanced intrahepatic echo, GB wall thickening | - | Enhanced echo, hepatomegaly, GB wall thickening | - |
| Dimethylformamide | 2003 | 1 | Toxic hepatitis | Diffuse hepatocellular disease | - | - | - |
| Trichloroethylene | 2005 | 3 | Toxic hepatitis, Stevens-Johnson syndrome | Hepatomegaly | - | - | Hepatocellular necrosis, intracellular cholestasis, ballooning degeneration |
| Chloroform | 2010 | 1 | Toxic hepatitis | - | - | Normal | - |
| Chloroform | 2014 | 2 | Toxic hepatitis | Normal | - | - | - |
| Mild fatty liver | |||||||
| HCFC-123 | 2017 | 2 | Toxic hepatitis | - | - | - | Portal and panlobular infiltration of mixed inflammatory cells, multifocal spotty and confluent necrosis, minimal macrovesicular and microvesicular steatosis |
Table 1 Summary of biochemical analysis of patient by date
aBefore admission; bOn admission; cDischarge & follow-up.
AST: aspartate aminotransferase; ALT: alanine aminotransferase; γ-GTP: gamma glutamyl transpeptidase; PT: prothrombin time; INR: international normalized ratio.
Table 2 Occupational liver diseases reported in the Annals of Occupational and Environmental Medicine
GB: gallbladder; CT: computed tomography.

