
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 35; 2023 > Article
- Original Article Risk of insomnia symptoms according to Work-Family Conflict by workers’ characteristics
-
Kwanghyun Seo1
 , Seungjun Ryu1, Saebomi Jeong1, Hee-Tae Kang1, Sung-Kyung Kim1, Sang-Baek Koh2, Kyoung Sook Jeong1, Sung-Soo Oh1
, Seungjun Ryu1, Saebomi Jeong1, Hee-Tae Kang1, Sung-Kyung Kim1, Sang-Baek Koh2, Kyoung Sook Jeong1, Sung-Soo Oh1 -
Annals of Occupational and Environmental Medicine 2023;35:e36.
DOI: https://doi.org/10.35371/aoem.2023.35.e36
Published online: August 23, 2023
1Department of Occupational and Environmental Medicine, Wonju Severance Christian Hospital, Wonju College of Medicine, Yonsei University, Wonju, Korea.
2Department of Preventive Medicine and Genomic Cohort Institute, Wonju College of Medicine, Yonsei University, Wonju, Korea.
- Correspondence: Kyoung Sook Jeong. Department of Occupational and Environmental Medicine, Wonju Severance Christian Hospital, Yonsei University Wonju College of Medicine, 20 Ilsan-ro, Wonju 26426, Korea. jeongks@yonsei.ac.kr
- Correspondence: Sung-Soo Oh. Department of Occupational and Environmental Medicine, Wonju Severance Christian Hospital, Yonsei University Wonju College of Medicine, 20 Ilsan-ro, Wonju 26426, Korea. oss0609@yonsei.ac.kr
• Received: February 21, 2023 • Revised: July 5, 2023 • Accepted: July 31, 2023
Copyright © 2023 Korean Society of Occupational & Environmental Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background Work-Family Conflict means that the demands of work and family roles cannot be met simultaneously, so one cannot concentrate on one’s work or family role. This conflict can negatively affect mental health and cause insomnia symptoms.
-
Methods This study was conducted on 20,442 subjects. Insomnia symptoms were assessed using the Minimal Insomnia Symptom Scale, and other variables were assessed using the questionnaire method. Logistic regression analyses were performed to evaluate the effect of Work-Family Conflict on insomnia symptoms, and subgroup logistic regression analyses were also performed.
-
Results The number of people with insomnia symptoms was 4,322 (15.1%). Compared with Low Work-Family Conflict, the odds ratios (ORs) for the risk of insomnia symptoms were 1.84 (95% confidence interval: 1.56–2.16) in High work-to-family conflict, 1.16 (1.02–1.32) in High family-to-work conflict, and 3.19 (2.87–3.55) in High Work-Family Conflict. The ORs were higher for men than women in High WFC but higher for women than men in High Work-Family Conflict.
-
Conclusions The risk of insomnia symptoms was highest in High Work-Family Conflict.
BACKGROUND
Insomnia in adults is characterized by sleep-related complaints, including difficulty falling asleep, frequent awakenings, and waking earlier than desired in the morning.1 The number of insomnia patients in Korea was approximately 680,000 in 2021, which is increasing every year.2 Several studies have shown that insomnia increases all-cause mortality3 and the risk of obesity, myocardial infarction, coronary artery disease, and congestive heart failure.4,5 In addition, insomnia is associated with an increased risk of anxiety, mood, impulsive, and substance abuse disorders,6 as well as increased suicidal ideation or suicide attempts.7
Work-Family Conflict occurs when the demands of work and family roles are not met simultaneously, and when this occurs, it becomes difficult to focus on either the work or family role.8 Work-Family Conflict is divided into 2 types: conflict at home caused by the role required at work (work-to-family conflict, WFC) and conflict at work caused by the role required at home (family-to-work conflict, FWC).9 The performance of the other roles is negatively affected by the stress of each conflict.10 Previous studies have shown that Work-Family Conflict is associated with poorer self-assessment mental health, physical health, and sleep.11 However, these studies often do not distinguish between the direction of Work-Family Conflict or analyze only WFC, and few have analyzed differences by gender or other social characteristics.
Insomnia can be caused by various internal medical diseases or conditions that interfere with sleep or sleep maintenance and can also be caused by psychiatric diseases or stressors.12 Work-Family Conflict negatively affects mental health by increasing the risk of developing mood, anxiety, and substance use disorders in both WFC and FWC.13 For this reason, we have tried to determine whether Work-Life Conflict increases the risk of insomnia symptoms.
Regarding gender, married women are more likely to have higher levels of Work-Family Conflict because they see housework as their role and do more of it, regardless of their occupation.14 In a study of front-line hotel workers in Türkiye, women suffered higher levels of WFC and FWC than men.15 Korea also has high traditional gender role stereotypes, so women are expected to have high levels of Work-Family Conflicts. However, over time, the proportion of men doing childcare and housework is gradually increasing.16 Therefore, it is increasingly important for men to understand the extent of Work-Family Conflict and confirm the impact of Work-Family Conflict.
Therefore, this study aims to show the relationship between Work-Family Conflict and insomnia symptoms according to various characteristics, including gender.
METHODS
Raw data were used from the 5th Korean Working Conditions Survey (KWCS) conducted in 2017 by the Occupational Safety and Health Research Institute (OSHRI), an affiliate of the Korea Occupational Safety and Health Agency. The KWCS is a nationwide survey of workers aged 15 and older to understand the overall work environment, including work patterns, occupations, industries, exposure to risk factors, and job stability.17 Of the 50,205 respondents, the following exclusion criteria were used to select wage earners aged 20 and over affected by Work-Family Conflict: one-person households, non-paid workers, teenagers, and military workers. We also excluded those who did not complete the survey or refused to answer the survey questions. Based on the exclusion criteria, 20,442 final participants were enrolled (Fig. 1). When standardization weights were applied to increase confidence, the study population was 28,576.
Fig. 1
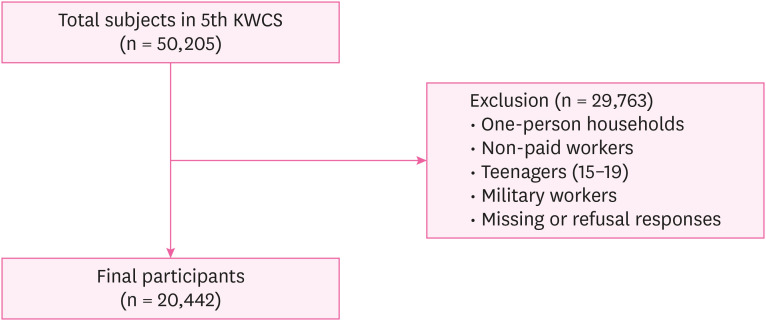
Classification of participants according to Work-Family Conflict.
KWCS: Korean Working Conditions Survey.
The questions used to assess Work-Family Conflict in the KWCS are as follows: the main question is “How often have you experienced any of the following in the past 12 months?,” and there are “I kept worrying about work when I was not working (lunchtime, after work, holiday, break),” “I felt too tired after work to do some of the household jobs which need to be done,” “I found that my job prevented me from giving the time I wanted to my family,” “I found it difficult to concentrate on my job because of my family responsibilities,” and “I found that my family responsibilities prevented me from giving the time should be given to my job” as sub-questions, and answer by selecting one of “Always, Most of the time, Sometimes, Rarely, Never” for each sub-question. Among the sub-questions, the first 3 questions examine WFC, and the remaining 2 examine FWC. The answers to the sub-questions were scored on a scale of 1 point from 5 to 1, starting with “Always,” and the scores were summed by dividing the WFC and FWC questions. As in previous studies,9,18 based on the median of the combined scores, the group was divided into a high group if it was at or above the median and a low group if it was below the median. This process divided it into 4 groups: Low Work-Family Conflict (low on WFC and FWC), High WFC, High FWC, and High Work-Family Conflict (high on both WFC and FWC). Of the total 28,576 subjects, there were 6,602 in the Low Work-Family Conflict group, 2,004 in the High WFC group, 6,663 in the High FWC group, and 13,307 in the High Work-Family Conflict group (Table 1).
Table 1
Four classifications of Work-Family Conflict
| Variables | WFC | ||
|---|---|---|---|
| Low | High | ||
| FWC | |||
| Low | Low Work-Family Conflict (n = 6,602) | High WFC (n = 2,004) | |
| High | High FWC (n = 6,663) | High Work-Family Conflict (n = 13,307) | |
The Minimal Insomnia Symptom Scale (MISS) was used to assess insomnia symptoms in the KWCS. The questions are as follows: The main question is “in the last 12 months, how often did you have any of the following sleep-related problems?,” and there are “Difficulty falling asleep,” “Waking up repeatedly during the sleep” and “Waking up with a feeling of exhaustion and fatigue” as sub-questions, and answer by selecting one of “Daily, Several times a week, Several times a month, Less often, Never” for each sub-question. Responses to each sub-question were summed on a scale of 1 point from 5 points to 1 point, starting with “Daily.” On the MISS questionnaire, a score of 6 or more can be considered insomnia between the ages of 20 and 64,19 and a follow-up study found that a score of 7 or more can be considered insomnia even in people 65 and older.20 Therefore, those with a total score of 7 or more were classified as having insomnia symptoms, and those with a 6 or fewer were classified as having no insomnia symptoms.
To understand the demographic characteristics of the subjects, sex, age, education level, and monthly income were examined. Age was divided into 5 categories: 20s, 30s, 40s, 50s, and 60s or older. Education level was divided into high school or below and university or above. Monthly income was divided into 4 categories: less than 1 million Korean won (KRW), 1 million to less than 2 million KRW, 2 million to less than 3 million KRW, and 3 million KRW or more. Then, to examine the mental health characteristics, depressive and anxiety symptoms were identified and classified into 2 categories, yes and no, respectively.
In addition, to identify the occupational characteristics of the subjects, workplace scale, weekly working time, occupational type, shift work, work intensity, job autonomy, job stress, and emotional labor were surveyed. The workplace scale was divided into 3 categories: less than 50 employees, 50 to less than 250 employees, and 250 or more employees. Weekly working time was divided into 3 categories: 40 hours or less, between 40 and 52 hours or less, and 53 hours or more. The occupational type was divided into 3 categories: blue-collar, service and sales, and white-collar. ‘Skilled Agricultural, Forestry, and Fishery Workers,’ ‘Craft and Related Trades Workers,’ ‘Equipment, Machine Operating and Assembling Workers,’ and ‘Elementary Workers’ were classified as blue-collar, ‘Service Workers’ and ‘Sales Workers’ as service and sales, and ‘Managers,’ ‘Professionals and Related Workers,’ and ‘Clerks’ as white-collar. Work intensity, job autonomy, and job stress were classified into 2 categories, high and low, and shift work and emotional labor were classified into 2 categories, yes and no.
χ2 and t-test were performed to examine the demographic characteristics of the subjects according to insomnia symptoms. Binomial logistic regression analyses examined the relationship between Work-Family Conflict and insomnia symptoms, with each model adjusted for confounders. As in previous studies,9,18 binomial logistic regression analyses identified the risk of insomnia symptoms for High WFC, High FWC, and High Work-Family Conflict, respectively, using the Low Work-Family Conflict group as a reference. Model 1 was adjusted for sex, age, and education level. Model 2 was adjusted for monthly income to examine the effect of monthly income separately from the confounding factors in Model 1. Model 3 was adjusted for occupational and mental health characteristics, including confounders in Model 2. In addition, subgroup logistic regression analyses were performed to identify differences by various characteristics. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated from the analysis, and the significance level was set at p < 0.05. Because the KWCS sampling design is a secondary probability proportion-stratified cluster sample survey, which can introduce significant bias if not weighted when performing statistical analyses, OSHRI recommends weighting for analysis. Therefore, the number of subjects, proportions (%), and p-values are presented using weighted data, and all analyses were performed using weighted data. All data were analyzed using IBM SPSS Statistics version 26.0 (IBM Corporation, Armonk, NY, USA).
This study used open and de-identified public data, so the exemption was approved by the Institutional Review Board of Wonju Severance Christian Hospital (CR322333).
RESULTS
Table 2 shows the characteristics of the subjects according to insomnia symptoms. Out of 28,576 subjects, 4,322 (15.1%) had insomnia. The mean age of all subjects was 43.2 ± 12.4 years (mean ± standard deviation), and the group with insomnia symptoms was 44.8 ± 12.9 years, statistically significantly higher than the group without insomnia symptoms. The number of people with symptoms of insomnia was statistically significantly higher with increasing age (19.2%), lower educational level (16.7%), and lower monthly income level (16.0%). In terms of mental health characteristics, people with depressive symptoms (33.7%) or anxiety symptoms (31.8%) were more likely to have symptoms of insomnia. Regarding occupational characteristics, the number of people with insomnia symptoms was statistically significantly higher in smaller workplaces (15.9%) and longer weekly working hours (20.5%). Regarding Work-Family Conflict, the High Work-Family Conflict group had the highest number of people with insomnia symptoms (22.6%).
Table 2
Characteristics of study subjects according to insomnia symptoms
Table 3 shows the distribution of Work-Family Conflict by general characteristics. The proportion of High Work-Family Conflict was significantly higher for males (46.3%), university or above (46.8%), higher weekly working time (59.7%), service and sales (48.7%), and shift work group (50.5%), and significantly lower for those aged 60 and over (39.4%).
Table 3
Distribution of Work-Family Conflict by general characteristics
Table 4 shows the results of the analysis of the relationship between Work-Family Conflict and insomnia symptoms. In the crude model, compared with Low Work-Family Conflict, the ORs for the risk of insomnia symptoms were 2.04 (95% CI: 1.74–2.39) with High WFC, 1.18 (1.04–1.34) with High FWC, and 3.73 (3.37–4.13) with High Work-Family Conflict. In Model 1, the ORs for the risk of insomnia symptoms were 2.14 (1.82–2.50) with High WFC, 1.20 (1.06–1.37) with High FWC, 3.85 (3.48–4.27) with High Work-Family Conflict. In Model 2, the ORs for the risk of insomnia symptoms were 2.21 (1.88–2.59) with High WFC, 1.22 (1.07–1.38) with High FWC, 3.97 (3.58–4.40) with High Work-Family Conflict. In Model 3, the ORs for the risk of insomnia symptoms were 1.84 (1.56–2.16) with High WFC, 1.16 (1.02–1.32) with High FWC, 3.19 (2.87–3.55) with High Work-Family Conflict.
Table 4
Odds ratios of insomnia symptoms according to Work-Family Conflict
Data are shown as odds ratio and 95% confidence intervals.
Sx: symptoms; WFC: work-to-family conflict; FWC: family-to-work conflict.
aModel 1: adjusted for sex, age, and education level.
bModel 2: adjusted for all variables in Model 1 and monthly income.
cModel 3: adjusted for all variables in Model 2, workplace scale, weekly working time, occupational type, shift work, work intensity, job autonomy, job stress, emotional labor, depressive symptom, and anxiety symptom.
Table 5 shows ORs for the risk of insomnia symptoms according to Work-Family Conflict in subgroups. For males, the ORs for the risk of insomnia symptoms were higher than for females at 1.98 (1.61–2.43) with High WFC and 1.19 (1.00–1.42) with High FWC, but for females, the OR was higher than for males at 3.62 (3.10–4.23) with High Work-Family Conflict. Among 20–29 years old, the OR for the risk of insomnia symptoms was highest with High Work-Family Conflict at 4.64 (3.50–6.15), compared with other age groups, while among 60+ year olds, the OR with High WFC was highest at 3.37 (2.20–5.16) compared with other age groups. For university or above, the OR for the risk of insomnia symptoms was 3.28 (3.10–4.14) with High Work-Family Conflict, and this OR was higher than for high school or below. Among those working 53 hours or more per week, the OR for the risk of insomnia symptoms was highest with High WFC at 2.22 (1.54–3.19), and among those working 40 hours or less per week, the OR with High Work-Family Conflict was highest at 3.82 (3.34–4.37). In the subgroup analysis by occupational type, service, and sales workers had the highest OR for risk of insomnia symptoms at 2.57 (1.78–3.72) with High WFC, and white-collar workers had the highest OR at 3.58 (3.04–4.2) with High Work-Family Conflict, but it was similar at 3.57 (2.81–4.55) in service and sales workers. In the shift work group, the OR for the risk of insomnia symptoms was 2.11 (1.43–3.11) with High WFC, which was higher than in the non-shift work group, but the OR for the non-shift work group was 3.29 (2.93–3.69) with High Work-Family Conflict, which was higher than in the shift work group.
Table 5
Adjusted odds ratios of insomnia symptoms according to Work-Family Conflict in subgroups
Data are shown as adjusted odds ratio and 95% confidence intervals.
WFC: work-to-family conflict; FWC: family-to-work conflict.
aAdjusted for sex, age, education level, monthly income, workplace scale, weekly working time, occupational type, shift work, work intensity, job autonomy, job stress, emotional labor, depressive symptom, and anxiety symptom.
DISCUSSION
In this study, the risk of insomnia symptoms was higher in the High Work-Family Conflict group. A previous meta-analysis study found that people with high job stress had a higher risk of insomnia,21 and the severity of sleep disturbance also increased when there were specific household stressors, such as parenting.18 It is also consistent with other research9,22 suggesting that a conflict between work and family roles causes insomnia symptoms. When looking at the High WFC and High FWC groups, the ORs for insomnia symptoms were higher in the High WFC group than in the High FWC group. It is consistent with a study of information technology workers in the United States,22 and it can be assumed that time at work is less flexible than time at home. Hence, the effect on insomnia symptoms is more remarkable.
In the subgroup analysis by sex, females had a higher OR than men with High Work-Family Conflict, and males had a higher OR than women with High WFC. Previous research has shown that women have higher levels of Work-Family Conflict than men because they feel more physically and emotionally burdened by what happens at home due to traditional gender role stereotypes, despite being in a dual-earner household.23 It is consistent with the results of this study, where women had a significantly higher risk of insomnia symptoms than men with High Work-Family Conflict. South Korea has the aforementioned traditional gender role stereotypes, but according to the Ministry of Gender Equality and Family’s 2021 Gender Equality Report, traditional gender role stereotypes have eased over the past 5 years.24 Therefore, the role of men in housework and caregiving has increased in recent years, and the influence of Work-Family Conflict is gradually increasing. In addition, in previous studies, the Work-Family Conflict experienced by men was often examined only for the effect of work environment variables rather than family-related variables, and there were many cases where the burden or lack of work environment variables affected the Work-Family Balance.25 Due to the nature of the survey, the KWCS has many questions about the work environment but few about the home environment. Therefore, it is most likely that Work-Family Conflict increased among men as awareness of traditional gender roles improved and as work-related stress was more fully included in the analysis, so it can be assumed that the difference in OR was higher in the High WFC group because the effect of Work-Family Conflict was further amplified.
In subgroup analyses by age, 20–29 years old had the highest OR with High Work-Family Conflict, and 60+ year olds had the highest OR with High WFC. Younger workers experience more psychological distress than any other generation due to impatience, skepticism, and lack of life and work experience.26 In a previous study, older people felt less negative work-family interaction,27 and younger people felt more Work-Family Conflict.25 For this reason, younger generations are likely to experience a great deal of stress when it comes to balancing work and family, and they are likely to be unfamiliar with how to deal with these conflicts. Therefore, younger people may be more susceptible to insomnia symptoms caused by Work-Family Conflict. However, the results of this study, where 60+ years old had the highest OR value with High WFC, are inconsistent with previous studies. It is thought that people over the age of 60 often re-enter the workforce after retiring from a previous job and that this process can be stressful due to their reduced occupational status and the need to learn new tasks, thus increasing their risk of developing insomnia symptoms due to WFC.
In the analysis by occupational type, the ORs for the risk of insomnia symptoms were higher in service and sales workers and in white collar workers than in blue collar workers. In addition, the ORs for the risk of insomnia symptoms with High Work-Family Conflict were higher in the university or above. Service and sales jobs involve the most emotional labor. Moreover, the more education you have, the more emotional labor you are exposed to.28 Previous studies have found that sleep disturbances increased significantly in both men and women who performed emotional labor,29 and other studies have suggested that emotional labor in the workplace can lead to Work-Family Conflict.30 Considering the results of these studies, due to the high frequency of exposure to emotional labor, the ORs for the risk of insomnia symptoms appeared higher in the High Work-Family Conflict of each subgroup.
When analyzing weekly working time and shift work, the ORs for the risk of insomnia symptoms increased in the High WFC group when the weekly working time was long or when shift work was performed. Conversely, the ORs increased in the High Work-Family Conflict group when the weekly working time was short or when shift work was not performed. According to previous studies, Work-Family Conflict increased for both men and women as working hours increased,10 and Work-Family Conflict increased for shift workers in a meta-analysis of 36 papers.31 Among men with children, the fewer hours they worked, the less Work-Family Conflict they had, and the less Work-Family Conflict they had, the more they tended to be involved in childcare.32 In addition, in a study that confirmed the linear relationship between working hours and WFC and FWC, as working hours increased, WFC increased linearly. However, FWC increased to a certain point and then decreased again, showing an inverted U-shape.33 Thus, our results are consistent with previous studies. It is thought to be because people who work long hours and shift work have much stress at work but little stress at home because they are not fulfilling their family roles, hence the statistically insignificant results. When Work-Family Conflict is high, employees who work fewer hours or do not work shifts are at higher risk for insomnia symptoms due to the co-occurrence of stress at home and work.
There are several limitations to this study. As a survey, the KWCS may be subject to recall bias. However, the KWCS is a large-scale survey of more than 20,000 Korean wage earners and reflects their reality. In addition, Work-Family Conflict may be influenced by family circumstances such as dual-income and number of children, and insomnia symptoms may be influenced by behaviors such as alcohol, tobacco, and caffeine use. However, these factors were not included in the KWCS, so we could not rule out the effects of these factors. Nevertheless, this study is meaningful in that it shows the association between Work-Family Conflict and insomnia symptoms by stratifying for factors such as gender and age in a large population.
CONCLUSIONS
Although there are various causes of insomnia symptoms, the risk of them is increased by stress caused by Work-Family Conflict. These risks were analyzed in subgroups by sex, age, occupation, and work environment. The risk was higher in females, as previously known, but the risk was also present in males. Based on these results, different policies or workplace-specific employee assistance programs can be implemented to manage insomnia symptoms in employees.
Acknowledgements
This study was conducted using the Korean Working Conditions Survey (KWCS) provided by the Occupational Safety and Health Research Institute (OSHRI). We are grateful to those who have made efforts to make these research materials available.
Abbreviations
CI
confidence interval
FWC
family-to-work conflict
KRW
Korean won
KWCS
Korean Working Conditions Survey
MISS
Minimal Insomnia Symptom Scale
OR
odds ratio
OSHRI
Occupational Safety and Health Research Institute
SD
standard deviation
Sx
symptoms
WFC
work-to-family conflict
-
Competing interests: The authors declare that they have no competing interests.
-
Authors contributions:
Conceptualization: Seo K.
Data curation: Seo K, Ryu S, Jeong S.
Formal analysis: Seo K.
Investigation: Ryu S, Jeong S, Jeong KS, Oh SS.
Methodology: Seo K, Oh SS.
Software: Seo K.
Supervision: Kang HT, Kim SK, Koh SB, Jeong KS, Oh SS.
Validation: Jeong KS, Oh SS.
Visualization: Seo K.
Writing - original draft: Seo K.
Writing - review & editing: Jeong KS, Oh SS.
NOTES
- 1. Owens JF, Matthews KA. Sleep disturbance in healthy middle-aged women. Maturitas 1998;30(1):41–50. 9819782.ArticlePubMed
- 2. HIRA Healthcare Bigdata Hub. Disease statistics of national interest. Updated 2022]. Accessed November 7, 2022]. http://opendata.hira.or.kr/op/opc/olapMfrnIntrsIlnsInfo.do .
- 3. Kripke DF, Simons RN, Garfinkel L, Hammond EC. Short and long sleep and sleeping pills. Is increased mortality associated? Arch Gen Psychiatry 1979;36(1):103–116. 760693.ArticlePubMed
- 4. Grandner MA, Jackson NJ, Pak VM, Gehrman PR. Sleep disturbance is associated with cardiovascular and metabolic disorders. J Sleep Res 2012;21(4):427–433. 22151079.ArticlePubMed
- 5. Pearson NJ, Johnson LL, Nahin RL. Insomnia, trouble sleeping, and complementary and alternative medicine: analysis of the 2002 national health interview survey data. Arch Intern Med 2006;166(16):1775–1782. 16983058.ArticlePubMed
- 6. Roth T, Jaeger S, Jin R, Kalsekar A, Stang PE, Kessler RC. Sleep problems, comorbid mental disorders, and role functioning in the national comorbidity survey replication. Biol Psychiatry 2006;60(12):1364–1371. 16952333.ArticlePubMedPMC
- 7. Pigeon WR, Pinquart M, Conner K. Meta-analysis of sleep disturbance and suicidal thoughts and behaviors. J Clin Psychiatry 2012;73(9):e1160–e1167. 23059158.ArticlePubMed
- 8. Greenhaus JH, Beutell NJ. Sources of conflict between work and family roles. Acad Manage Rev 1985;10(1):76–88.Article
- 9. Sato S, Liu Y, Ikeda A, Filomeno R, Suzuki Y, Maruyama K, et al. Work-family conflict and insomnia symptoms among women working in aged care services in Japan. Sleep Med 2021;82:155–158. 33930791.ArticlePubMed
- 10. Voydanoff P. Work role characteristics, family structure demands, and work/family conflict. J Marriage Fam 1988;50(3):749–761.Article
- 11. Borgmann LS, Rattay P, Lampert T. Health-related consequences of work-family conflict from a European perspective: results of a scoping review. Front Public Health 2019;7:189. 31338358.ArticlePubMedPMC
- 12. Thorpy MJ. Classification of sleep disorders. Neurotherapeutics 2012;9(4):687–701. 22976557.ArticlePubMedPMCPDF
- 13. Frone MR. Work-family conflict and employee psychiatric disorders: the National Comorbidity Survey. J Appl Psychol 2000;85(6):888–895. 11155895.ArticlePubMed
- 14. Sohn YM, Park CY. Influence of work-family related values on work-family conflict and facilitation: focused on married working woman. J Korea Contents Assoc 2015;15(7):203–215.Article
- 15. Yavas U, Babakus E, Karatepe OM. Attitudinal and behavioral consequences of work-family conflict and family-work conflict: does gender matter? Int J Serv Ind Manage 2008;19(1):7–31.
- 16. Son MG. The changes of father’s participation in the domestic activities of everyday life: focusing on statistics from time use survey in 1999 and 2014. J Korean Soc Trend Perspect 2016;6.
- 17. Choi Y, Park J. The Korean Working Conditions Survey (KWCS): a review on the utilization of the survey database. J Korean Soc Occup Environ Hyg 2019;29(4):431–441.
- 18. Eshak ES. Work-to-family conflict rather than family-to-work conflict is more strongly associated with sleep disorders in Upper Egypt. Ind Health 2019;57(3):351–358. 30101898.ArticlePubMed
- 19. Broman JE, Smedje H, Mallon L, Hetta J. The Minimal Insomnia Symptom Scale (MISS): a brief measure of sleeping difficulties. Ups J Med Sci 2008;113(2):131–142. 18509808.PubMed
- 20. Hellström A, Hagell P, Fagerström C, Willman A. Measurement properties of the Minimal Insomnia Symptom Scale (MISS) in an elderly population in Sweden. BMC Geriatr 2010;10(1):84. 21054878.PubMedPMC
- 21. Yang B, Wang Y, Cui F, Huang T, Sheng P, Shi T, et al. Association between insomnia and job stress: a meta-analysis. Sleep Breath 2018;22(4):1221–1231. 29959635.ArticlePubMedPDF
- 22. Buxton OM, Lee S, Beverly C, Berkman LF, Moen P, Kelly EL, et al. Work-family conflict and employee sleep: evidence from IT workers in the Work, Family and Health Study. Sleep 2016;39(10):1871–1882. 27568810.ArticlePubMedPMC
- 23. Fujimura Y, Sekine M, Tatsuse T. Sex differences in factors contributing to family-to-work and work-to-family conflict in Japanese civil servants. J Occup Health 2014;56(6):485–497. 25374422.ArticlePubMedPDF
- 24. Ministry of Gender Equality and Family (KR). 2021 Gender equality report. Updated 2022]. Accessed November 14, 2022]. http://www.mogef.go.kr/mp/pcd/mp_pcd_s001d.do?mid=plc500&bbtSn=704919 .
- 25. Yoon SY, Kim HJ. A Study on the subjective cognition and conflict degree of work-family balance and family strength of a dual career men. J Korean Fam Resour Manage Assoc 2013;17(2):19–35.
- 26. Sawang S, Newton CJ. Defining work stress in young people. J Employ Couns 2018;55(2):72–83.ArticlePDF
- 27. Choung SI, Lee KY. A study on the interaction between work-family of married employees. J Korean Fam Resour Manage Assoc 2007;11(1):83–107.
- 28. Park SH. Emotional labor job characteristics and policy implications using KNOW. Korean Longit Stud Elder Employ 2015;(10):2–13.
- 29. Kang D, Yang JW, Choi WJ, Ham S, Kang SK, Lee W. Anxiety, depression and sleep disturbance among customer-facing workers. J Korean Med Sci 2019;34(48):e313. 31833267.ArticlePubMedPMCPDF
- 30. Yanchus NJ, Eby LT, Lance CE, Drollinger S. The impact of emotional labor on work–family outcomes. J Vocat Behav 2010;76(1):105–117.Article
- 31. Wöhrmann AM, Müller G, Ewert K. Shift work and work-family conflict: a systematic review. Sozialpolitik Ch 2020;3:1–6.
- 32. Lee S, Kwon Y. The mediating effect of work-family conflict on the relationship between family-friendly workplace culture and paternal involvement. Fam Cult 2009;21(1):1–28.Article
- 33. Adkins CL, Premeaux SF. Spending time: the impact of hours worked on work–family conflict. J Vocat Behav 2012;80(2):380–389.Article
REFERENCES
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Longitudinal trajectories and risk factors of insomnia symptoms among Chinese bus drivers
Jingbo Zhao, Huatao Yang, Qiling Fan, Zijie Ma, Yang Yang, Zicong Guan, Guoxi He
Frontiers in Public Health.2026;[Epub] CrossRef - The relationship between sleep quality and occupational identity among psychiatric night shift nurses
Qianqian Qin, Haiyan Zhu, Mu Yu, Juan Bao, Zejun Ma, Xueyan Zhu, Kaihong Tang, Peiyun Zhang
Frontiers in Psychiatry.2026;[Epub] CrossRef - Insomnia and women: exploring vulnerability, impact, and intervention
Hae Ri Kim, Soo In Kim, Weon-Jeong Lim, Somi Jeong, So Hyun Ahn, Eunju Jeong, Sun-Young Kim
Sleep and Breathing.2026;[Epub] CrossRef - Benefits and Drawbacks of 12-hour Shifts in Steel Manufacturing: a Comprehensive Qualitative Investigation of Workers, Managers, and Family Perspectives
Alireza Choobineh, Mahnaz Shakerian, Majid Faraji, Hossein Modaresifar, Javad Kiani, Mehdi Hatami, Reza Tahmasebi
Occupational Health Science.2025; 9(4): 1075. CrossRef - Female workers with long working hours are more likely to have depressive symptoms when having family-to-work conflict
Garin Lee, Ji-Hwan Kim, Seung-Sup Kim
International Archives of Occupational and Environmental Health.2024; 97(2): 199. CrossRef - Association between long working hours and engagement in preventive healthcare services in Korean workers: Findings from the Korean National Health and Nutrition Examination Survey
Seong-Uk Baek, Yu-Min Lee, Jin-Ha Yoon
Preventive Medicine.2024; 180: 107849. CrossRef - Difficulty Falling Asleep, Nocturnal Awakening, Sleep Dissatisfaction, and Irritability in the General Population
Tetsuya Akaishi
The Tohoku Journal of Experimental Medicine.2024; 263(4): 261. CrossRef - Association between single-person household wage workers in South Korea and insomnia symptoms: the 6th Korean Working Conditions Survey (KWCS)
Yoon Ho Lee, Yong-Jin Lee, Eun-Chul Jang, Young-Sun Min, Soon-Chan Kwon
Ann Occup Environ Med.2024; 36: e25. CrossRef
 Cite
CiteRisk of insomnia symptoms according to Work-Family Conflict by workers’ characteristics
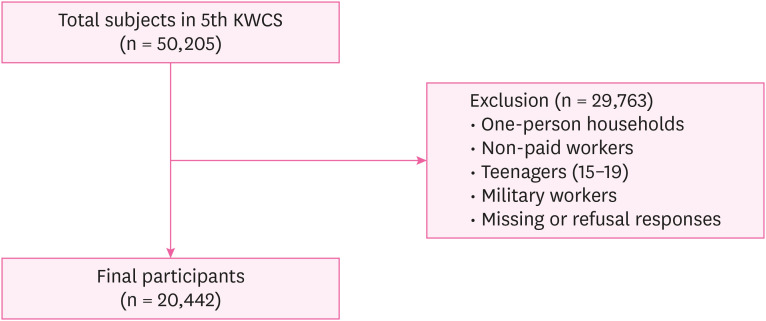
Fig. 1 Classification of participants according to Work-Family Conflict.KWCS: Korean Working Conditions Survey.
Fig. 1
Risk of insomnia symptoms according to Work-Family Conflict by workers’ characteristics
| Variables | WFC | ||
|---|---|---|---|
| Low | High | ||
| FWC | |||
| Low | Low Work-Family Conflict (n = 6,602) | High WFC (n = 2,004) | |
| High | High FWC (n = 6,663) | High Work-Family Conflict (n = 13,307) | |
| Variables | Total (n = 28,576)a | Insomnia Sx | |||
|---|---|---|---|---|---|
| Yes (n = 4,322)a | No (n = 24,254)a | ||||
| Sex | < 0.001 | ||||
| Male | 16,302 (57.0) | 2,336 (14.3) | 13,966 (85.7) | ||
| Female | 12,274 (43.0) | 1,986 (16.2) | 10,288 (83.8) | ||
| Age (years) | < 0.001 | ||||
| 20–29 | 4,631 (16.2) | 633 (13.7) | 3,998 (86.3) | ||
| 30–39 | 7,388 (25.9) | 981 (13.3) | 6,407 (86.7) | ||
| 40–49 | 7,743 (27.1) | 1,136 (14.7) | 6,607 (85.3) | ||
| 50–59 | 5,879 (20.6) | 1,008 (17.1) | 4,871 (82.9) | ||
| ≥ 60 | 2,936 (10.3) | 564 (19.2) | 2,372 (80.8) | ||
| Mean ± SD | 43.2 ± 12.4 | 44.8 ± 12.9 | 42.9 ± 12.3 | < 0.001 | |
| Education level | < 0.001 | ||||
| High school or below | 10,943 (38.3) | 1,825 (16.7) | 9,118 (83.3) | ||
| University or above | 17,633 (61.7) | 2,496 (14.2) | 15,137 (85.8) | ||
| Monthly income (10,000 Korean won) | 0.003 | ||||
| < 100 | 1,896 (6.6) | 304 (16.0) | 1,592 (84.0) | ||
| 100–199 | 6,987 (24.5) | 1,142 (16.3) | 5,845 (83.7) | ||
| 200–299 | 8,176 (28.6) | 1,188 (14.5) | 6,988 (85.5) | ||
| 300 | 11,517 (40.3) | 1,687 (14.6) | 9,830 (85.4) | ||
| Depressive symptom | < 0.001 | ||||
| No | 27,985 (97.9) | 4,122 (14.7) | 23,863 (85.3) | ||
| Yes | 590 (2.1) | 199 (33.7) | 391 (66.3) | ||
| Anxiety symptom | < 0.001 | ||||
| No | 27,759 (97.1) | 4,062 (14.6) | 23,697 (85.4) | ||
| Yes | 817 (2.9) | 260 (31.8) | 557 (68.2) | ||
| Workplace scale (persons) | < 0.001 | ||||
| 1–49 | 20,744 (72.6) | 3,304 (15.9) | 17,440 (84.1) | ||
| 50–249 | 5,026 (17.6) | 676 (13.5) | 4,350 (86.5) | ||
| ≥ 250 | 2,806 (9.8) | 342 (12.2) | 2,464 (87.8) | ||
| Weekly working time (hours) | < 0.001 | ||||
| ≤ 40 | 17,065 (59.7) | 2,330 (13.7) | 14,735 (86.3) | ||
| 41–52 | 7,871 (27.5) | 1,245 (15.8) | 6,626 (84.2) | ||
| ≥ 53 | 3,640 (12.7) | 746 (20.5) | 2,894 (79.5) | ||
| Occupational type | < 0.001 | ||||
| Blue-collar | 8,889 (31.1) | 1,408 (15.8) | 7,481 (84.2) | ||
| Service and sales | 5,523 (19.3) | 943 (17.1) | 4,580 (82.9) | ||
| White-collar | 14,163 (49.6) | 1,970 (13.9) | 12,193 (86.1) | ||
| Shift work | < 0.001 | ||||
| No | 25,306 (88.6) | 3,676 (14.5) | 21,630 (85.5) | ||
| Yes | 3,270 (11.4) | 646 (19.8) | 2,624 (80.2) | ||
| Work intensity | < 0.001 | ||||
| Low | 13,359 (46.7) | 1,369 (10.2) | 11,990 (89.8) | ||
| High | 15,217 (53.3) | 2,953 (19.4) | 12,264 (80.6) | ||
| Job autonomy | 0.017 | ||||
| High | 14,187 (49.6) | 2,073 (14.6) | 12,114 (85.4) | ||
| Low | 14,389 (50.4) | 2,249 (15.6) | 12,140 (84.4) | ||
| Job stress | < 0.001 | ||||
| Low | 19,786 (69.2) | 2,505 (12.7) | 17,281 (87.3) | ||
| High | 8,790 (30.8) | 1,817 (20.7) | 6,973 (79.3) | ||
| Emotional labor | < 0.001 | ||||
| No | 16,784 (58.7) | 2,265 (13.5) | 14,519 (86.5) | ||
| Yes | 11,793 (41.3) | 2,057 (17.4) | 9,736 (82.6) | ||
| Work-Family Conflict | < 0.001 | ||||
| Low Work-Family Conflict | 6,602 (23.1) | 478 (7.2) | 6,124 (92.8) | ||
| High WFC | 2,004 (7.0) | 275 (13.7) | 1,729 (86.3) | ||
| High FWC | 6,663 (23.3) | 564 (8.5) | 6,099 (91.5) | ||
| High Work-Family Conflict | 13,307 (46.6) | 3,004 (22.6) | 10,303 (77.4) | ||
| Subgroup | Work-Family Conflict | |||||
|---|---|---|---|---|---|---|
| Low Work-Family Conflict (n = 6,602)a | High WFC (n = 2,004)a | High FWC (n = 6,663)a | High Work-Family Conflict (n = 13,307)a | |||
| Sex | < 0.001 | |||||
| Male | 3,654 (22.4) | 1,274 (7.8) | 3,830 (23.5) | 7,544 (46.3) | ||
| Female | 2,948 (24.0) | 730 (5.9) | 2,833 (23.1) | 5,763 (47.0) | ||
| Age (years) | < 0.001 | |||||
| 20–29 | 1,213 (26.2) | 312 (6.7) | 1,158 (25.0) | 1,947 (42.1) | ||
| 30–39 | 1,504 (20.4) | 541 (7.3) | 1,768 (23.9) | 3,575 (48.4) | ||
| 40–49 | 1,749 (22.6) | 597 (7.7) | 1,646 (21.3) | 3,751 (48.4) | ||
| 50–59 | 1,274 (21.7) | 389 (6.6) | 1,338 (22.8) | 2,878 (49.0) | ||
| ≥ 60 | 863 (29.4) | 164 (5.6) | 753 (25.6) | 1,156 (39.4) | ||
| Education level | < 0.001 | |||||
| High school or below | 2,686 (24.5) | 702 (6.4) | 2,497 (22.8) | 5,058 (46.2) | ||
| University or above | 3,917 (22.2) | 1,302 (7.4) | 4,166 (23.6) | 8,249 (46.8) | ||
| Weekly working time (hours) | < 0.001 | |||||
| ≤ 40 | 4,449 (26.1) | 972 (5.7) | 4,534 (26.6) | 7,110 (41.7) | ||
| 41–52 | 1,666 (21.2) | 611 (7.8) | 1,570 (19.9) | 4,024 (51.1) | ||
| ≥ 53 | 488 (13.4) | 421 (11.6) | 558 (15.3) | 2,173 (59.7) | ||
| Occupational type | < 0.001 | |||||
| Blue-collar | 2,121 (23.9) | 656 (7.4) | 2,016 (22.7) | 4,097 (46.1) | ||
| Service and sales | 1,213 (22.0) | 321 (5.8) | 1,297 (23.5) | 2,692 (48.7) | ||
| White-collar | 3,268 (23.1) | 1,027 (7.3) | 3,349 (23.6) | 6,519 (46.0) | ||
| Shift work | < 0.001 | |||||
| No | 5,907 (23.3) | 1,715 (6.8) | 6,028 (23.8) | 11,656 (46.1) | ||
| Yes | 695 (21.3) | 289 (8.8) | 635 (19.4) | 1,651 (50.5) | ||
| Work-Family Conflict | Insomnia Sx | |||
|---|---|---|---|---|
| Crude | Model 1a | Model 2b | Model 3c | |
| Low Work-Family Conflict | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) |
| High WFC | 2.04 (1.74–2.39) | 2.14 (1.82–2.50) | 2.21 (1.88–2.59) | 1.84 (1.56–2.16) |
| High FWC | 1.18 (1.04–1.34) | 1.20 (1.06–1.37) | 1.22 (1.07–1.38) | 1.16 (1.02–1.32) |
| High Work-Family Conflict | 3.73 (3.37–4.13) | 3.85 (3.48–4.27) | 3.97 (3.58–4.40) | 3.19 (2.87–3.55) |
| Subgroup | Work-Family Conflicta | ||||
|---|---|---|---|---|---|
| Low Work-Family Conflict | High WFC | High FWC | High Work-Family Conflict | ||
| Sex | |||||
| Male | 1 (Ref.) | 1.98 (1.61–2.43) | 1.19 (1.00–1.42) | 2.91 (2.52–3.37) | |
| Female | 1 (Ref.) | 1.60 (1.23–2.09) | 1.13 (0.93–1.36) | 3.62 (3.10–4.23) | |
| Age (years) | |||||
| 20–29 | 1 (Ref.) | 2.46 (1.61–3.77) | 1.36 (0.97–1.90) | 4.64 (3.50–6.15) | |
| 30–39 | 1 (Ref.) | 1.80 (1.26–2.56) | 1.38 (1.04–1.83) | 3.35 (2.64–4.26) | |
| 40–49 | 1 (Ref.) | 1.94 (1.41–2.67) | 1.28 (0.98–1.69) | 3.43 (2.75–4.28) | |
| 50–59 | 1 (Ref.) | 1.23 (0.85–1.78) | 1.02 (0.78–1.33) | 2.60 (2.10–3.23) | |
| ≥ 60 | 1 (Ref.) | 3.37 (2.20–5.16) | 0.88 (0.64–1.21) | 3.15 (2.41–4.11) | |
| Education level | |||||
| High school or below | 1 (Ref.) | 1.63 (1.26–2.10) | 1.13 (0.94–1.37) | 2.77 (2.37–3.24) | |
| University or above | 1 (Ref.) | 2.02 (1.64–2.50) | 1.18 (0.99–1.41) | 3.28 (3.10–4.14) | |
| Weekly working time (hours) | |||||
| ≤ 40 | 1 (Ref.) | 1.35 (1.05–1.74) | 1.09 (0.93–1.28) | 3.82 (3.34–4.37) | |
| 41–52 | 1 (Ref.) | 1.76 (1.29–2.41) | 1.37 (1.06–1.78) | 3.14 (2.54–3.87) | |
| ≥ 53 | 1 (Ref.) | 2.22 (1.54–3.19) | 1.10 (0.76–1.61) | 1.79 (1.32–2.42) | |
| Occupational type | |||||
| Blue-collar | 1 (Ref.) | 1.56 (1.18–2.07) | 1.05 (0.85–1.30) | 2.62 (2.20–3.13) | |
| Service and sales | 1 (Ref.) | 2.57 (1.78–3.72) | 1.26 (0.94–1.67) | 3.57 (2.81–4.55) | |
| White-collar | 1 (Ref.) | 1.83 (1.44–2.34) | 1.22 (1.00–1.48) | 3.58 (3.04–4.20) | |
| Shift work | |||||
| No | 1 (Ref.) | 1.76 (1.47–2.10) | 1.15 (1.00–1.32) | 3.29 (2.93–3.69) | |
| Yes | 1 (Ref.) | 2.11 (1.43–3.11) | 1.20 (0.85–1.70) | 2.62 (1.97–3.49) | |
Table 1 Four classifications of Work-Family Conflict
Number of workers was weighted.
WFC: work-to-family conflict; FWC: family-to-work conflict.
Table 2 Characteristics of study subjects according to insomnia symptoms
Unit: person (%).
Sx: symptoms; WFC: work-to-family conflict; FWC: family-to-work conflict; SD: standard deviation.
aWeighted numbers of workers.
bχ2 test for binomial variables and t-test for numeric variables.
Table 3 Distribution of Work-Family Conflict by general characteristics
Unit: person (%).
WFC: work-to-family conflict; FWC: family-to-work conflict.
aWeighted numbers of workers.
bχ2 test for binomial variables and t-test for numeric variables.
Table 4 Odds ratios of insomnia symptoms according to Work-Family Conflict
Data are shown as odds ratio and 95% confidence intervals.
Sx: symptoms; WFC: work-to-family conflict; FWC: family-to-work conflict.
aModel 1: adjusted for sex, age, and education level.
bModel 2: adjusted for all variables in Model 1 and monthly income.
cModel 3: adjusted for all variables in Model 2, workplace scale, weekly working time, occupational type, shift work, work intensity, job autonomy, job stress, emotional labor, depressive symptom, and anxiety symptom.
Table 5 Adjusted odds ratios of insomnia symptoms according to Work-Family Conflict in subgroups
Data are shown as adjusted odds ratio and 95% confidence intervals.
WFC: work-to-family conflict; FWC: family-to-work conflict.
aAdjusted for sex, age, education level, monthly income, workplace scale, weekly working time, occupational type, shift work, work intensity, job autonomy, job stress, emotional labor, depressive symptom, and anxiety symptom.

