
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 35; 2023 > Article
- Case Report A case of syncope in a villager with hypertrophic cardiomyopathy after hydrogen sulfide exposure by an unauthorized discharge of wastewater
-
Hyeonjun Kim1
 , Seunghyeon Cho2, Inho Jung1, Sunjin Jung1, Won-Ju Park1
, Seunghyeon Cho2, Inho Jung1, Sunjin Jung1, Won-Ju Park1 -
Annals of Occupational and Environmental Medicine 2023;35:e34.
DOI: https://doi.org/10.35371/aoem.2023.35.e34
Published online: August 21, 2023
1Department of Occupational and Environmental Medicine, Chonnam National University Medical School and Chonnam National University Hwasun Hospital, Hwasun, Korea.
2Department of Occupational and Environmental Medicine, Chonnam National University Hospital, Gwangju, Korea.
- Correspondence: Won-Ju Park. Department of Occupational and Environmental Medicine, Chonnam National University Medical School and Chonnam National University Hwasun Hospital, 322 Seoyang-ro, Hwasun 58128, Korea. wonjupark@jnu.ac.kr
• Received: March 31, 2023 • Revised: July 19, 2023 • Accepted: July 31, 2023
Copyright © 2023 Korean Society of Occupational & Environmental Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background Hydrogen sulfide is a toxic substance that humans can be exposed to occupationally, and cases of hydrogen sulfide poisoning of workers in industrial sites are commonly reported. However, there have been no cases of poisoning of the public due to an unauthorized discharge of wastewater, so it is important to describe this incident.
-
Case presentation In a small village in Jeollanam-do, Republic of Korea, accounts of a terrible stench had been reported. A 26-year-old man who lived and worked in a foul-smelling area was taken to the emergency room with a headache, dizziness, nausea, and repeated syncope. A subsequent police and Ministry of Environment investigation determined that the cause of the stench was the unauthorized discharge of 9 tons of wastewater containing hydrogen sulfide through a stormwater pipe while the villagers were sleeping. The patient had no previous medical history or experience of symptoms. Leukocytes and cardiac markers were elevated, an electrocardiogram indicated biatrial enlargement, left ventricular hypertrophy, and corrected QT interval prolongation. Myocardial hypertrophy was detected on a chest computed tomography scan, and hypertrophic cardiomyopathy was confirmed on echocardiography. After hospitalization, cardiac marker concentrations declined, symptoms improved, and the patient was discharged after 7 days of hospitalization. There was no recurrence of symptoms after discharge.
-
Conclusions We suspect that previously unrecognized heart disease manifested or was aggravated in this patient due to exposure to hydrogen sulfide. Attention should be paid to the possibility of unauthorized discharge of hydrogen sulfide, etc., in occasional local incidents and damage to public health. In the event of such an accident, it is necessary to have government guidelines in place to investigate health impact and follow-up clinical management of exposed residents.
BACKGROUND
Hydrogen sulfide is a colorless, highly toxic irritant and asphyxiant chemical gas.1 Hydrogen sulfide is a gas considered a chemical threat in oil production, well drilling, and gas refining industries. It can be created by various industrial processes and anaerobic reactions of wastewater, settling ponds, toilets, and sludge and appears to be an occupational hazard in many workplaces.2 Acute exposure to low concentrations of hydrogen sulfide causes eye and lung irritation, headache, arrhythmia, and nausea and exposure to hydrogen sulfide above 1,000 parts per million (ppm) can be lethal.3,4 After recovery from acute poisoning from hydrogen sulfide, peripheral neuropathy, and delirium can still occur, and there have been reports of bradycardia, cardiac hypertrophy, myocardial injury, and proteinuria.5,6,7
The toxic mechanism of hydrogen sulfide comprises the inactivation of cytochrome c oxidase activity and the interruption of the cellular metabolism of oxygen.8 By this mechanism, hypoxic brain damage, hypoxic cardiac damage, mucosal irritation, and pulmonary edema can be induced.6 Hydrogen sulfide is known to affect ion channels (calcium channels and adenosine triphosphate [ATP]-sensitive potassium channels). In an experimental study conducted based on this, hydrogen sulfide inhibits cell excitability, shortens the duration of action potentials, increases transmural dispersion of tissue repolarization, increases the sensitivity to tissue reentry initiation and maintenance, and causes pro-arrhythmic effects.9 Cases of hydrogen sulfide poisoning in existing industrial sites and unmanaged toilets have been frequently described, but there have been no cases reported of poisoning of the public due to an illegal discharge of wastewater. Therefore, we would like to communicate such a case report.
CASE PRESENTATION
In one area of Jeollanam-do, end of September, from 4:30 am to 3:00 pm, 127 villagers called emergency services (emergency number in Korea; 119 fire and ambulance service, 112 police service) due to discomfort due to a strong stench. The villagers complained of irritation of the nose and eyes, dizziness, nausea, and vomiting. The weather in the area was rainy with an average temperature of 18.4°C (minimum to maximum: 17.3 to 20.0°C), average wind speed of 1.1 m/s, average humidity of 92%, and daily precipitation of 13.5 mm. As a result of an investigation by the police and the Ministry of Environment, the causative substance was hydrogen sulfide. The concentration of hydrogen sulfide around the sewer was up to 160 ppm. A subsequent investigation revealed that a wastewater treatment company illegally discharged 9 tons of wastewater containing hydrogen sulfide into a stormwater pipe through a tank lorry at 3:30 am in the rain.
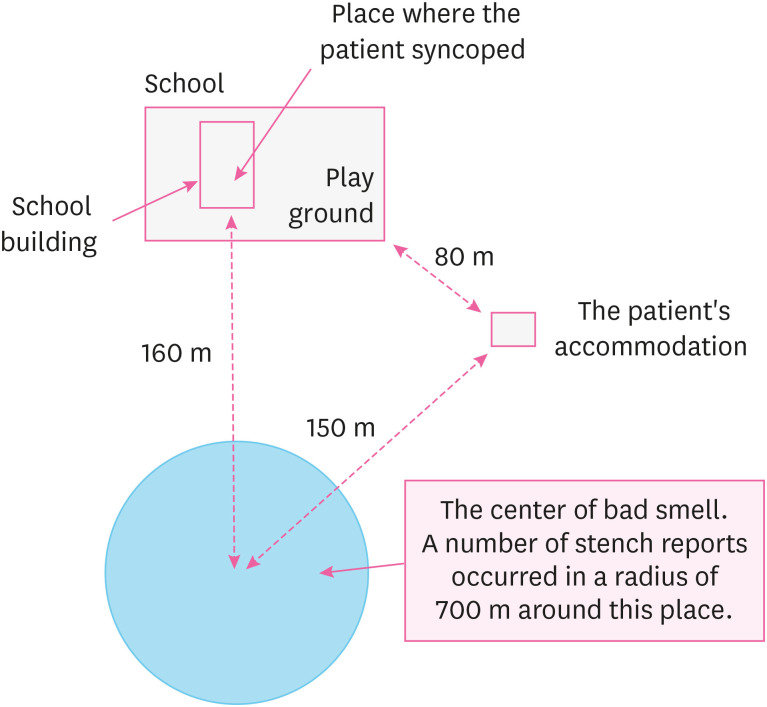
The patient was a 26-year-old Caucasian Canadian man who was employed as a foreign language teacher at a local high school. Living accommodations were provided to the patient near the school, at a distance less than 80 m. The living accommodations and school were included in the areas with high odor. The frequent odor exposure areas, including workplaces and residences were 150 to 160 m away. Due to the bad odor, the patient was affected with headache, dizziness, and nausea in his living quarters since dawn. The patient went to work and experienced 2 brief losses of consciousness lasting one to 2 minutes in the afternoon. While preparing to leave work around 4:30 pm, he fainted again and was transferred to the local emergency room through 119. Consciousness was restored at the local emergency room. After emergency treatment, the patient was transferred to the university hospital for further evaluation for poisoning (Fig. 1).
Chief complains
Loss of consciousness (3 or more times), alert when visiting the local emergency room.
Past medical history and family disease
None. No alcohol and drinking. No specific findings.
Vital signs
At the visit to the local emergency room, the patient’s blood pressure was 90/60 mmHg. After transfer to the university hospital, 3 hours after the loss of consciousness, the measured blood pressure was confirmed as 100/60 mmHg, respiratory rate was 20 breaths per minute, and pulse rate was 97 beats per minute. The patient’s body temperature was 36.4°C.
Laboratory results
Troponin-I measured after syncope at the first hospital visit was 112.0 pg/mL (normal range: 0.0–34.2), and creatinine kinase-myocardial band (CK-MB) was 23 U/L (normal range: 0.0–25.0). The results of the blood tests performed at the university hospital were as follows. White blood cell count increased (15.9 × 103/mm3), on differential count: neutrophils were amplified (85.8%), and lymphocytes decreased (8.2%). Tests within normal range were eosinophils (0.6%), basophils (0.2%), red blood cells (4.39 × 106/mm3), hemoglobin (12.9 g/dL), hematocrit (39.7%), and platelet count (204 × 103/mm3). Troponin-I and CK-MB mass concentrations were enhanced (Troponin-I: 0.816 ng/mL, CK-MB mass: 8.46 ng/mL). The pro-B-type natriuretic peptide (1,447 pg/mL) and prothrombin time both increased (15.3/61.9/1.32 sec/%/international normalized ratio) and activated partial thromboplastin time was within normal range.
Diagnostic test results
Prolonged corrected QT interval (QTc; 491 ms, normal < 450 ms) was observed on electrocardiogram (ECG). No significant abnormal findings were indicated on chest posterior-anterior . Chest computed tomography findings showed myocardial hypertrophy of the left ventricle (LV) wall.
Progression
After admission to the ward and supportive care (O2 inhalation, intravenous fluid therapy), troponin-I and CK-MB decreased (Fig. 2). After 4 days of inpatient treatment, echocardiography was performed. The results included an enlarged left atrium (46.3 mm), normal LV chamber size with diffuse thickened LV wall (interventricular septal dimension = 14.3 mm, relative wall thickness = 0.62, LV mass = 261 mL), and a mild amount of pericardial effusion at the right ventricle apical site. Left atrial enlargement was defined as a left atrial diameter of 41.0 mm or greater in men.10 The cardiologist diagnosed the patient with hypertrophic cardiomyopathy (HCMP) (Fig. 3).
Fig. 2
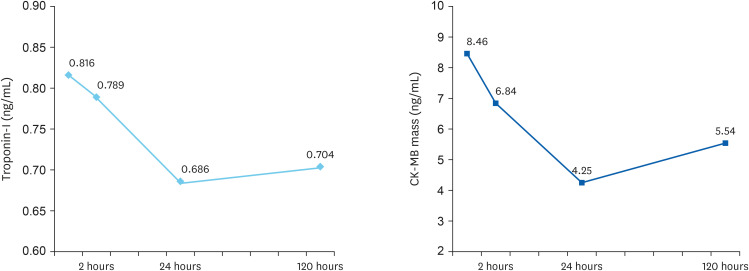
Changes in the cardiac enzymes of the patient. (A) Troponin-I (normal range: 0.0–0.3 ng/mL); (B) CK-MB mass (normal range: 0.00–4.87 ng/mL).
CK-MB: creatinine kinase-myocardial band.
Fig. 3
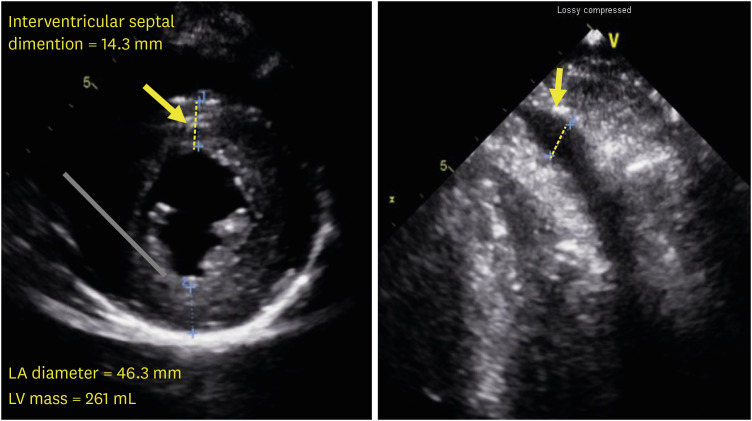
Echocardiography of the patient. (A) Thickened left ventricular wall. (B) Pericardial effusion at right ventricular apical site.
LA: left atrium; LV: left ventricle.
After 5 days of inpatient treatment, the 24-hour Holter test displayed no premature ventricular complexes, no ventricular tachycardia, bradyarrhythmia, and no ST-T change. The patient was discharged with no symptoms remaining on the day 7 of hospitalization. Ten days after discharge, he visited the hospital for a cardiac magnetic resonance imaging (MRI) examination. The results indicated diffuse hypertrophy of the LV wall, decreased LV global systolic function (ejection fraction: 48.1%), small amount of pericardial effusion. The patient visited the hospital 18 months after the incident and was administered echocardiography and an ECG. There were no symptoms for 18 months, and there were no issues with work performance. No significant interval change was observed on echocardiography, and HCMP was still confirmed (interventricular septal dimension = 12.4 mm, mid lateral segment = 16.0 mm). In the ECG, it was confirmed that the QTc was 465 ms, which was shorter than at the time of hospitalization.
The study protocol was approved by the Institutional Review Board (IRB) of Chonnam National University Hospital (IRB No. CNUHH-2023-074), and written informed consent was obtained from the patient for the publication of this report and any accompanying data.
DISCUSSION AND CONCLUSION
We report a case of syncope in a villager with HCMP after hydrogen sulfide exposure caused by illegally discharged wastewater. After inhaling the stench for several hours, the patient was hospitalized for syncope episodes and increased cardiac biomarkers. He was diagnosed with HCMP via ECG, echocardiography, and cardiac MRI. His workplace was unrelated to hydrogen sulfide exposure. This case is rare in that exposure and health effects occurred in the public rather than a workplace incident. In addition, many existing cases of hydrogen sulfide poisoning were caused by lung damage and suffocation, but in this case cardiac health effects occurred. There is a distinct possibility that HCMP, which was previously asymptomatic and not recognized by the patient, manifested or was aggravated due to exposure to hydrogen sulfide. After the patient was discharged from the hospital, his symptoms completely recovered, and there were no symptoms during the follow-up hospital visit.
Hydrogen sulfide has a very low odor threshold and high toxicity.11 Its smell of rotten eggs can be detected at a concentration as low as 0.02 ppm. Irritation to the mucosa, such as the eye, nose, and throat, occurs in individuals exposed to hydrogen sulfide at a range of up to 100 ppm. Paralysis of the olfactory nerve transpires when exposed to a range above 100 ppm, which makes it impossible to detect the hydrogen sulfide through the nasal warning. Exposure up to 1,000 ppm has more severe physiological effects, such as neurological, pulmonary, and cardiac symptoms. Table 1 summarizes the health effects of hydrogen sulfide at various exposure levels. Hydrogen sulfide is a chemical asphyxiant and causes histotoxic anoxia. Hydrogen sulfide inhibits cytochrome oxidase, preventing ATP formation and promoting production of reactive oxygen species.12 This is the mechanism of toxicity of hydrogen sulfide. Hydrogen sulfide significantly affects cardiovascular disease as a gaseous signaling molecule.9,10,11,12,13,14,15 Hydrogen sulfide cause inhibition of various cardiac ion channels and myocyte electrophysiology.
Table 1
Reported health effects of hydrogen sulfide at various exposure level
This patient encountered a foul smell and had a headache from the illegally discharged wastewater since dawn and fainted in the afternoon. Subsequent medical examination revealed elevated cardiac markers, QTc prolongation, and HCMP. HCMP is likely to be a previously unknown underlying disease. The typical mechanism of syncope in HCMP patients is believed to be caused by arrhythmias and primary hemodynamic mechanisms.16 It is also known that about 13% of HCMP patients were accompanied by QT interval prolongation, and in a recent study when next-generation sequencing analysis of people with these comorbidities was performed, the results were announced that they were related to genes related to ion channels.17 In addition, a previous study revealed that a group exposed to a low concentration of gas-containing sulfur compounds in a region of south Iran had an ECG alteration compared to a group without it.18 The following assumptions were made about the mechanism for the syncope that occurred after exposure to hydrogen sulfide in this case. Even at concentrations lower than the previously announced concentrations that cause cardiotoxicity, cardiogenic syncope occurred as ion channels, or myocytes were affected by gas exposure in a state where arrhythmias were likely to occur due to underlying diseases such as HCMP or long QT interval. It should be realized that people with pre-existing cardiomyopathy may be more susceptible than others to hydrogen sulfide exposure.
Hydrogen sulfide is generated naturally and as a by-product of many industrial processes, such as petroleum refining, sewage disposal, and mining.6 There have been many narratives of worker hydrogen sulfide poisoning cases due to workplace sewage treatment. Through these case experiences, measures to prevent hydrogen sulfide poisoning have been proposed. However, case reports of hydrogen sulfide exposure and intoxication in the public are lacking. It is always necessary to keep in mind the possibility of unauthorized discharge of hydrogen sulfide and occurrence of public health incidents, and in this process, sophisticated policies and systems are needed to minimize damage to the health of residents from exposure to harmful substances.
The Chemical Substances Control Act has been in effect in the Republic of Korea since January 1, 2015. According to this law, if the health of residents is damaged due to a chemical accident, the Minister of Environment must conduct a Health Impact Assessment (HIA). However, it is difficult to conduct a HIA properly due to administrative limitations. Since 2014, the National Institute of Chemical Safety has been writing chemical accident statistics, and from 2014 to February 2023, 757 chemical accidents occurred.19 However, it is judged that many accidents were omitted, and in this case, a large number of residents had been exposed to hydrogen sulfide, but HIA was not conducted. Currently, in the event of a chemical accident, a preliminary investigation is conducted to determine whether to conduct a HIA. In conclusion, since 2015, 5 HIAs have been conducted by the Chemical Accident HIA Support Center, which has signed a business agreement with the Ministry of Environment. Table 2 briefly summarizes the investigations conducted.
Table 2
Health Impact Assessments according to the Chemical Substances Control Act in the Republic of Korea
In this incident, HIA was not properly performed according to the law. Many villagers reported severe odor, nausea, and dizziness to emergency services (119 or 112), but the HIA on the entire village population was not conducted. So, confirming the estimated exposures, the progress of patients who visited the hospital, and medical records was impossible. It would have been nice if we had performed objective examinations (cardiac markers or echocardiography) had been performed through the investigation of additional exposed residents, but it was not. Therefore, the limitation of this study is that we cannot completely rule out the possibility of coincidence. Also, a limitation of this case report is that the patient’s exact level of exposure was not measured. Information on the exposure of this patient was obtained from medical records including emergency transport records, interviews with the patient and co-workers, and media reports from the fire department and the Ministry of Environment. Although we have not been able to measure the patient’s exact exposure level, the concentration of hydrogen sulfide measured in the sewer was estimated to be 160 ppm, and it was measured to be about 1 ppm in the village air. The American Conference of Governmental Industrial Hygienists revised the exposure limits for hydrogen sulfide to 1 ppm (time-weighted average) and 5 ppm (short-term exposure level). Because the patient was in an area with a strong odor for a long time, he was highly probably exposed to risk levels of hydrogen sulfide.
In case of similar incidents in the future, a preemptive and proactive HIA should be conducted, and management of the health effects of residents should be carefully considered. The government designates the Chemical Accident HIA Support Centers nationwide and encourages experts to participate in HIA. The interest and participation of occupational and environmental medicine experts are needed, and systematic education and training programs should also be established in the future. Additionally, at present, only myocardial infarction cases have been reported in many cases regarding the cardiotoxicity of hydrogen sulfide. Further studies and case reports on the health effects related to arrhythmias according to the concentration and exposure period of hydrogen sulfide will be needed.
Acknowledgements
We thank all the members of the Health Promotion Center at Chonnam National University Hwasun Hospital. We thank all the members of the Department of Occupational and Environmental Medicine at Chonnam National University Hwasun Hospital and Chonnam National University Hospital. We wish the patient good health and well-being.
Abbreviations
ATP
adenosine triphosphate
CK-MB
creatinine kinase-myocardial band
ECG
electrocardiogram
HCMP
hypertrophic cardiomyopathy
HIA
Health Impact Assessment
LA
left atrium
LV
left ventricle
MRI
magnetic resonance imaging
ppm
parts per million
QTc
corrected QT interval
-
Competing interests: Prof. Won-Ju Park has been a member of the editorial board of the Annals of Occupational and Environmental Medicine since 2021. He was not involved in the review process. Otherwise, no potential conflict of interest relevant to this article was reported.
-
Authors contributions:
NOTES
- 1. Environmental Protection Agency (EPA). Toxicological review of hydrogen sulfide (CAS No. 7783-06-04). Updated 2003]. Accessed March 30, 2023]. https://iris.epa.gov/static/pdfs/0061tr.pdf .
- 2. Kim JG, Lee KJ, Lee SW, Park JB. Acute hydrogen sulfide poisoning: two cases report. Korean J Occup Environ Med 2000;12(1):148–155.ArticlePDF
- 3. Guidotti TL. Hydrogen sulphide. Occup Med (Lond) 1996;46(5):367–371. 8918153.ArticlePubMed
- 4. Lewis RJ. Sax’s Dangerous Properties of Industrial Materials. 9th ed. New York, NY, USA: Van Nostrand Reinhold; 1996.
- 5. Gosselin RE, Smith RP, Hodge HC. Clinical Toxicology of Commercial Products. 5th ed. Baltimore, MD, USA: Williams and Wilkins; 1984.
- 6. Lee EC, Kwan J, Leem JH, Park SG, Kim HC, Lee DH, et al. Hydrogen sulfide intoxication with dilated cardiomyopathy. J Occup Health 2009;51(6):522–525. 19779278.ArticlePubMedPDF
- 7. Mo W, Shen J, Huang X, Zhang Y, Zhang Z. Acute myocardial injury following hydrogen sulfide poisoning. Toxicol Ind Health 2020;36(10):750–758. 32757890.ArticlePubMedPDF
- 8. Ng PC, Hendry-Hofer TB, Witeof AE, Brenner M, Mahon SB, Boss GR, et al. Hydrogen sulfide toxicity: mechanism of action, clinical presentation, and countermeasure development. J Med Toxicol 2019;15(4):287–294. 31062177.ArticlePubMedPMCPDF
- 9. Zhang S, Zhang S, Fan X, Wang W, Li Z, Jia D, et al. Pro-arrhythmic effects of hydrogen sulfide in healthy and ischemic cardiac tissues: insight from a simulation study. Front Physiol 2019;10:1482. 31920692.ArticlePubMedPMC
- 10. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr 2005;18(12):1440–1463. 16376782.ArticlePubMed
- 11. Guidotti TL. Hydrogen sulfide intoxication. Handb Clin Neurol 2015;131:111–133. 26563786.PubMed
- 12. Haouzi P, Sonobe T, Judenherc-Haouzi A. Developing effective countermeasures against acute hydrogen sulfide intoxication: challenges and limitations. Ann N Y Acad Sci 2016;1374(1):29–40. 26945701.ArticlePubMedPMC
- 13. Zhang R, Sun Y, Tsai H, Tang C, Jin H, Du J. Hydrogen sulfide inhibits L-type calcium currents depending upon the protein sulfhydryl state in rat cardiomyocytes. PLoS One 2012;7(5):e37073. 22590646.ArticlePubMedPMC
- 14. Paul BD, Snyder SH. H2S signalling through protein sulfhydration and beyond. Nat Rev Mol Cell Biol 2012;13(8):499–507. 22781905.ArticlePubMedPDF
- 15. Kolluru GK, Shackelford RE, Shen X, Dominic P, Kevil CG. Sulfide regulation of cardiovascular function in health and disease. Nat Rev Cardiol 2023;20(2):109–125. 35931887.ArticlePubMedPMCPDF
- 16. Williams L, Frenneaux M. Syncope in hypertrophic cardiomyopathy: mechanisms and consequences for treatment. Europace 2007;9(9):817–822. 17522079.ArticlePubMed
- 17. Cava F, Micolonghi C, Musumeci MB, Petrucci S, Savio C, Fabiani M, et al. Long QTc in hypertrophic cardiomyopathy: a consequence of structural myocardial damage or a distinct genetic disease? Front Cardiovasc Med 2023;10:1112759. 37089884.ArticlePubMedPMC
- 18. Bahaoddini A, Mohabbatkar H, Rivaz M, Saadat M. ECG alteration due to prolong exposure to natural gas leakage containing sulfur compounds in polluted areas of Masjid-I-Sulaiman (south of Iran). Ecotoxicol Environ Saf 2009;72(3):885–888. 18242699.ArticlePubMed
- 19. National Institute of Chemical Safety (NICS). Chemical accident status and cases. Updated 2023]. Accessed July 16, 2023]. https://icis.me.go.kr/ .
REFERENCES
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Assessment of the Impact of Blasting Operations on the Intensity of Gas Emission from Rock Masses: A Case Study of Hydrogen Sulfide Occurrence in a Polish Copper Ore Mine
Aleksandra Banasiewicz, Michalina Kotyla, Sebastian Gola
Applied Sciences.2025; 15(23): 12781. CrossRef
 Cite
CiteA case of syncope in a villager with hypertrophic cardiomyopathy after hydrogen sulfide exposure by an unauthorized discharge of wastewater
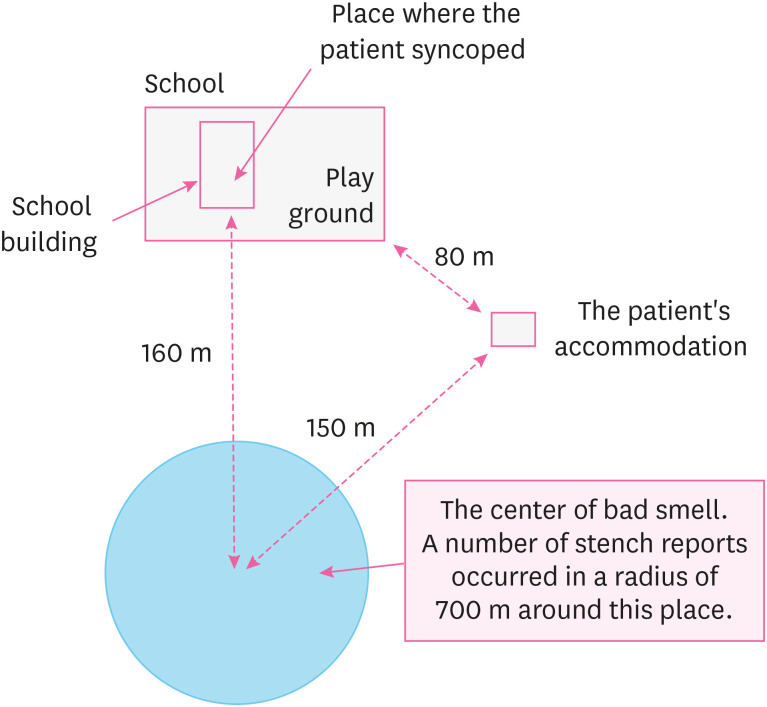
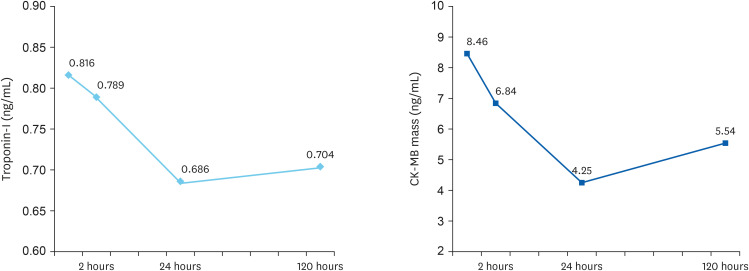
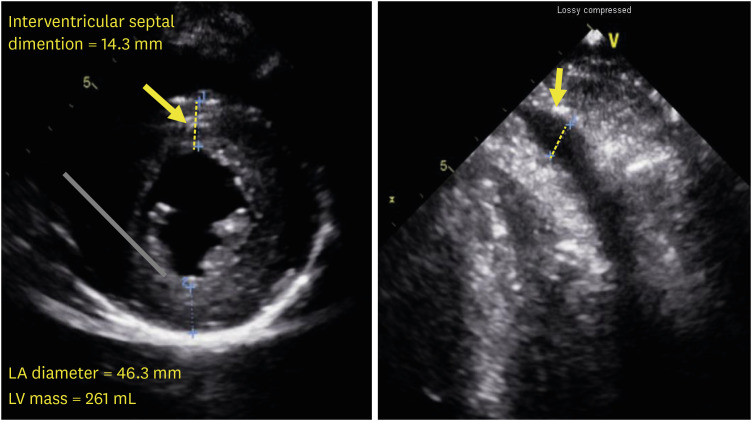
Fig. 1 Schematic map of the area where the patient was suspected of exposure to hydrogen sulfide.
Fig. 2 Changes in the cardiac enzymes of the patient. (A) Troponin-I (normal range: 0.0–0.3 ng/mL); (B) CK-MB mass (normal range: 0.00–4.87 ng/mL).CK-MB: creatinine kinase-myocardial band.
Fig. 3 Echocardiography of the patient. (A) Thickened left ventricular wall. (B) Pericardial effusion at right ventricular apical site.LA: left atrium; LV: left ventricle.
Fig. 1
Fig. 2
Fig. 3
A case of syncope in a villager with hypertrophic cardiomyopathy after hydrogen sulfide exposure by an unauthorized discharge of wastewater
| Concentration (ppm) | Effects |
|---|---|
| 0.01–0.03 | Smell is detectable |
| 1.5 | Maximal allowed concentration when exposed daily for 8 hours |
| 5–10 | Unpleasant penetrating smell |
| > 50 | Ocular conjunctiva irritation |
| 100–200 | Olfactory nerve paralysis, loss of the scent, upper respiratory tract irritation |
| 250–500 | Excitement, headache, cyanosis, pulmonary edema |
| 500–700 | Ataxia, nausea, dizziness, unconsciousness, respiratory paralysis; lethal after 30 minutes |
| > 1,000 | Nervous system paralysis, diaphragm paralysis after one breath; death within minutes |
| > 5,000 | Imminent death |
| Variables | Accident 1 | Accident 2 | Accident 3 | Accident 4 | Accident 5 |
|---|---|---|---|---|---|
| Date of accident | June 22, 2015 | June 4, 2016 | July 26, 2016 | April 13, 2018 | May 17, 2019 |
| Investigation period | 2015.06–2015.10 | 2016.06 | 2016.07–2016.08 | 2018.08–2018.12 | 2019.05.31–2020.03.30 |
| Accident area | Gunsan-si | Geumsan-gun | Sejong-si | Incheon | Seosan-si |
| Exposed substance | Silicon tetrachloride | Hydrofluoric acid | Hydrofluoric acid | Complex exposure due to fire | Oil vapor (styrene monomer) |
| Number of people investigated | 179 | 108 | 129 | 99 | 1,201 |
Table 1 Reported health effects of hydrogen sulfide at various exposure level
ppm: parts per million, 1 ppm of hydrogen sulfide (molecular weight 34) equals 1.4 mg hydrogen sulfide per m3.
Table 2 Health Impact Assessments according to the Chemical Substances Control Act in the Republic of Korea

