
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 34; 2022 > Article
- Special Article Standards for recognition and approval rate of occupational cerebro-cardiovascular diseases in Korea
-
Ui-Jin Kim1,2
 , Won-Jun Choi1,2,3, Seong-Kyu Kang1,2,3, Wanhyung Lee1,2,3, Seunghon Ham1,2,3, Junhyeong Lee1,2, Yongho Lee1,2, Eunseun Han1,2, Sanghyuk Lee1,2, Yongkyu Kim4, Inah Kim5
, Won-Jun Choi1,2,3, Seong-Kyu Kang1,2,3, Wanhyung Lee1,2,3, Seunghon Ham1,2,3, Junhyeong Lee1,2, Yongho Lee1,2, Eunseun Han1,2, Sanghyuk Lee1,2, Yongkyu Kim4, Inah Kim5 -
Annals of Occupational and Environmental Medicine 2022;34:e30.
DOI: https://doi.org/10.35371/aoem.2022.34.e30
Published online: October 25, 2022
1Department of Medicine, Graduate School of Gachon University, Incheon, Korea.
2Department of Occupational and Environmental Medicine, Gachon University Gil Medical Center, Incheon, Korea.
3Department of Occupational and Environmental Medicine, Gachon University College of Medicine, Incheon, Korea.
4Department of Occupational and Environmental Medicine, Korea Workers’ Compensation & Welfare Service Incheon Hospital, Incheon, Korea.
5Department of Occupational and Environmental Medicine, Hanyang University, Seoul, Korea.
- Correspondence: Won-Jun Choi. Department of Occupational and Environmental Medicine, College of Medicine, Gachon University, 38-13 Dokjeom-ro 3beon-gil, Namdong-gu, Incheon 21565, Korea. wjchoi@gachon.ac.kr
• Received: April 23, 2022 • Revised: July 8, 2022 • Accepted: October 11, 2022
Copyright © 2022 Korean Society of Occupational & Environmental Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background Although working hours have decreased in Korea, they are still high compared to that of other countries. In Korea, cardiovascular and cerebrovascular diseases (CCVDs) related to overwork in Korea continually occur, and the social burden from overwork is estimated to be high. This study investigated the amendment of regulations affecting the approval rate of occupational CCVDs.
-
Methods The change in approval rate of occupational CCVDs and related regulations were investigated using the Act and public notice on the standards for recognition of occupational CCVDs and the yearbooks of the Ministry of Employment and Labor. The CCVD mortality was estimated using data on the number of deaths according to the cause of death, the number of employed people, and resident registration population aged 15–64 years. The cumulative mortality of CCVDs was estimated using the Kaplan-Meier method.
-
Results Since the establishment of the standards for recognition in Korea in 1982, the scope of occupational diseases has been expanded to include intracerebral hemorrhage, subarachnoid hemorrhage, cerebral infarction, myocardial infarction, and aortic dissection. In 2013, the concept of working hours was introduced in chronic overwork. The approval rate of occupational CCVDs was 44.7% in 2006, which decreased to 12.9% in 2011. After the improvement of related regulations, the approval rate increased to 41.3% in 2018. From 2000 to 2017, the CCVD mortality of both the unemployed and employed tended to decrease, and their cumulative CCVD mortalities were 549.3 and 319.7 per 100,000 people, respectively.
-
Conclusions CCVDs are recognized as occupational diseases in Korea. The amendments to the standards for recognition, the introduction of the Occupational Disease Adjudication Committee, the principle of presumption, and the reduction of working hours have changed the approval rate of occupational CCVDs. A strategic approach is needed to further reduce the incidence of CCVDs.
BACKGROUND
With the revision of the Labor Standard Act in 2018, the annual working hours in Korea have been declining steadily as the statutory maximum working hours were decreased, and the scope of the place of business for which these revised working hours should be applied was expanded.1,2 However, according to the statistics from the Organisation for Economic Co-operation and Development (OECD), the annual working hours per capita wage of workers in Korea was 1,927 hours in 2020, the third longest among OECD countries.3
Japan is the first country to compensate for cardiovascular and cerebrovascular diseases (CCVDs) similarly to that for industrial accidents.4 In 1969, a young 29-year-old man working as a newspaper delivery man died of subarachnoid hemorrhage. The cause of the cerebral hemorrhage was not obvious and could not be identified, so assumed that it was caused by overwork.5 Since then, more than 100 similar cases have occurred in Japan. At the 51st annual meeting of the Japan Association of Industrial Health in 1978, Uehata6 first used the word “Karoshi” to describe “death from acute circulatory disease due to the exacerbation of underlying diseases, such as hypertension and atherosclerosis, caused by prolonged overwork.” Karoshi has been used internationally since 1991. In 1997, the term “Karoshi - Death from overwork” was published in the International Journal of Health Service, and the Oxford Medical Dictionary defined it as “death from overwork or work-related fatigue”.5 Subsequently, Japan enacted the Karoshi Prevention Measures Promotion Act on November 1, 2014, stipulating that the country is responsible for promoting effective measures to prevent Karoshi.
Although the world’s occupational health community has paid attention to Karoshi, there are still questions about the possibility of CCVDs being caused by long hours of work, i.e., the relevance of Karoshi to CCVDs. Karoshi has been dismissed in East Asia, mainly in Japan, Korea, and Taiwan, as a special phenomenon caused by excessive working hours. However, a large-scale meta-analysis conducted jointly by the World Health Organization (WHO) and International Labour Organization (ILO) indicated that long working hours were associated with ischemic heart disease and stroke.7,8
In Korea, the average working hours have decreased over the years. Studies have been conducted, and various policies, such as the Five-Year Plan for Industrial Accident Prevention Plan9 of the Ministry of Employment and Labor and the Revised Rules on Occupational Safety and Health Standards10 have been developed to prevent CCVDs in workers. However, CCVD cases recognized as industrial accidents related to overwork continue to occur. In Korea, cerebrovascular or heart disease caused by occupational overwork is defined as an occupational disease under the Industrial Accident Compensation Insurance Act.11 Workers can be compensated by insurance if they develop health problems due to their work.12 The requirements for recognizing CCVDs as occupational diseases are set and notified by the Minister of Employment and Labor. The requirements are largely divided into the occurrence of sudden unpredictable events and/or rapid changes in the working environment, short-term occupational overwork, and chronic overwork (Supplementary Table 1).13
In this study, we aimed to summarize the state of occupational CCVDs in Korea and changes in the policies involved to draw implications.
METHODS
The standards for recognition of occupational accidents regarding occupational diseases or deaths due to occupational diseases based on the revised period of the Enforcement Regulation of the Industrial Accident Compensation Insurance Act were searched through the Korean Law Information Center.14,15,16 In addition, public notices by the Ministry of Employment and Labor17,18,19,20,21 were searched for data on standards for approval of CCVDs as occupational diseases, and the changes in standards for recognition were summarized.
Disclosure data relating to the approval status of occupational accidents published by the Ministry of Employment and Labor22 and the literature23,24 stating previous approval rates of CCVDs were used to determine the numbers of applications for and approvals of CCVDs as occupational diseases. We calculated the occupational disease approval rate by dividing the number of occupational disease approvals by the number of applications and investigated changes in the industrial accident approval rate resulting from changes in policy and standards for recognition.
From 2000 to 2017, the numbers of deaths from CCVDs and their cumulative mortality rates among the unemployed and employed were investigated. The numbers of deaths and mortality rates of CCVDs for the employed and unemployed were identified using the Korean Statistical Information Service data on the numbers of deaths25 and mortality rates26 of those aged 15–64 years according to the cause of deaths well as data on the employed,27 resident registration population,28,29 and resident registration mid-year population.30 The sex and age-specific mid-year populations of Korea were calculated using the resident registration mid-year population derived from the resident registration population.31 Among the participants of the Economically Active Population Survey, the employed were defined as those who worked for more than an hour to obtain income, unpaid family workers, and temporarily unemployed workers.32 In this study, employed persons aged 15–64 years were selected as the study participants. The unemployed population was defined as the remaining population in Korea aged 15–64 years after the employed population in this age group was excluded. The unemployed were defined as the remaining resident registered population per year after excluding the employed population. The mortality rate of the unemployed was calculated as the number of deaths per year by the specific cause of death divided by the unemployed population of the corresponding year. The number of CCVD deaths of the employed was defined as the number of CCVD deaths by occupation, excluding students, homemakers, and the unemployed, and the CCVD mortality rate of the employed was calculated as the number of CCVD deaths of the employed divided by the number of employed people. The cumulative mortality rates of the unemployed and employed for CCVDs were calculated using the Kaplan-Meier method.33,34
RESULTS
The history of revisions of the standards for approval of CCVDs as occupational diseases is shown in Table 1. In 1982, the standards for recognizing CCVDs as occupational accidents were enacted for the first time in Korea. According to the standards at that time, only stroke and sudden cardiac death caused by an occupational injury or by occupational work were recognized. In addition, a CCVD was recognized only if the occupational factor was a medically sufficient cause of the disease (the established rule of the Ministry of Labor, No. 71).35 In the 1983 amendment, a CCVD was recognized as an occupational disease “when workers with predispositions or underlying diseases develop central nervous system disorders and circulatory diseases in connection with their work under employment subordinate and controlling management” (the established rule of the Ministry of Labor, No. 92). Subsequently, the standards were relaxed to recognize occupational accidents with disease onsets that are work-related as occupational accidents, while previously, occupational factors had to be a sufficient cause of disease onsets. A subsequent amendment in 1989 made it possible for pre-existing diseases such as intraparenchymal or subarachnoid hemorrhage to be recognized as occupational accidents if they developed in the course of work (the established rule of the Ministry of Labor, No. 167). In May 1993, the scope of recognized diseases was expanded to intraparenchymal hemorrhage, subarachnoid hemorrhage, cerebral infarction, hypertensive encephalopathy, primary cardiac arrest, angina, and myocardial infarction (the established rule of the Ministry of Labor, No. 234). However, primary cardiac arrest was excluded from the list of recognized diseases (the established rule of the Ministry of Labor, No. 247).
Table 1
Revision history of standards for the approval of CCVDs as occupational diseases
In the early 1990s, cases of CCVDs in driving and sales adjuncts, cement mixers in apartment construction sites were recognized as industrial accidents.36,37 The Supreme Court decided that even if the main cause of the disease is not directly related to work performance and at least occupational overwork, in addition to the main cause of the disease, caused or worsened the disease, a causal relationship should be considered. The court also ruled that diseases caused by overwork include those that usually allow normal work to continue or existing diseases that rapidly worsen due to overwork. Based on these precedents, the standards for recognition were relaxed in 1994 to recognize accidents that occurred in the course of work as occupational accidents unless there was clear medical evidence that they were spontaneous. In 2001, the concepts of “rapid changes in the working environment” and “chronic overwork” were introduced38 (the established rule of the Ministry of Labor, No. 247). In 1995, with a complete revision of the Industrial Accident Compensation Insurance Act, the standards for recognition of CCVDs, which had been specified in the provision of standards for recognition of occupational accidents in the established rule of the Ministry of Labor, were transferred to the Enforcement Regulation of the Industrial Accident Compensation Insurance Act.22 In this act, the standards for recognition of occupational accidents were divided into standards for recognition of occupational accidents and occupational diseases. In 1999, dissecting aortic aneurysm was included in the list of recognized diseases. With the revision of the Industrial Accident Compensation Insurance Act in 2008, the provision on the standards for recognizing CCVDs was transferred to the Enforcement Decree of the Industrial Accident Compensation Insurance Act. The act stated that the Minister of Employment and Labor was in charge of the notification of the requirements for occupational disease recognition. Intraparenchymal and subarachnoid hemorrhages that developed during work were removed from the standards for recognition. The diseases such as hypertensive encephalopathy and angina were also removed because the mechanism of these diseases was considered to be different from that of typical CCVDs. Since 2013, the concept of working hours has been introduced to recognize chronic overwork.
Since 2018, the provision that the health status of workers should be considered has been removed from the short-term overwork criteria, in which more specific criteria have been established, such as dividing chronic overwork into three levels according to working hours. In 2017, Song et al. reviewed the results of existing studies on occupational triggers for CCVDs, recognition precedents of CCVDs as occupational diseases, and international standards for recognition. They investigated other factors that intensify workload in addition to working hours (Supplementary Table 2).39 Consequently, night working hours were being calculated by adding 30% of daytime working hours. In evaluating chronic overwork, jobs with schedules that are difficult to predict, shift jobs, jobs with insufficient holidays, jobs in which workers are exposed to harmful work environments (cold, temperature change, and noise), jobs with high physical loads, jobs that required frequent business travels with a long jet lag, jobs with high mental strain, etc. were considered as weighting factors of work burden.
Fig. 1 shows the number of CCVD deaths and mortality rates as well as occupational disease approvals and approval rates for the years 2000 to 2020. The numbers of occupational disease approvals were 1,006 in 2000, reached a peak of 2,017 in 2004,23,24 and dropped to 319 in 2011.40,41 The number of approvals increased to 471 in 2014 and decreased slightly to 421 in 2016, followed by an increase to 1,265 in 2019 and a later decrease to 929 in 2020. The occupational disease approval rate was 81.0% in 2000, reached 44.7% in 2006 and 45.0% in 2007, and it began to decline again in 2008, further declined to 12.9% in 2011, increased to 23.5% in 2015, decreased to 22.0% in 2016, increased to 41.3% in 2018, and decreased slightly to 38.2% in 2020.
Fig. 1
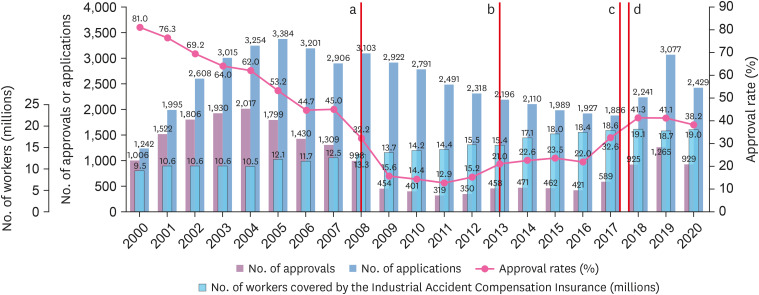
Numbers of applications and approvals of CCVDs as occupational diseases per year and their approval rate as well as numbers of workers covered by the Industrial Accident Compensation Insurance (2000–2020).
aIn July 2008, the standards for recognition of CCVDs were tightened (removing the provision that recognized cerebral hemorrhage as an occupational disease in the course of work) and the Occupational Disease Review Commission system was introduced; bIn July 2013, the standards for recognition of CCVDs were relaxed (working hours added); cIn September 2017, the principle of estimation was applied; and dIn January 2018, the standards for recognition of CCVDs were relaxed (eliminating the duty for health status considerations of short-term overwork workers, subdividing standard time for chronic overwork, and taking into account weighting factors of workload and night shifts).
CCVD: cardiovascular and cerebrovascular disease.
Fig. 2 shows the number of deaths, mortality rate, and cumulative mortality rate of CCVDs by year in the unemployed and employed aged 15–64 years from 2000 to 2017. In unemployed, mortality rates per 100,000 by each disease tended to decrease from 2000 to 2017 as follows: from 48.2 to 20.8 for CCVDs, 12.0 to 7.8 for cardiovascular diseases, and 36.3 to 13.0 for cerebrovascular diseases. Similarly, in employed, mortality rates per 100,000 by each disease also tended to decrease from 2000 to 2017 as follows: from 29.1 to 15.9 for CCVDs, 9.5 to 7.4 for cardiovascular diseases, and 19.6 to 8.5 for cerebrovascular diseases. The cumulative mortality rates of each disease per 100,000 unemployed and employed from 2000 to 2017 are as follows: 549.3 and 319.7 for CCVDs, 167.1 and 134.4 for cardiovascular diseases, and 382.2 and 185.3 for cerebrovascular diseases, respectively, with the unemployed showing higher cumulative mortality rates for all diseases than those of the employed.
Fig. 2
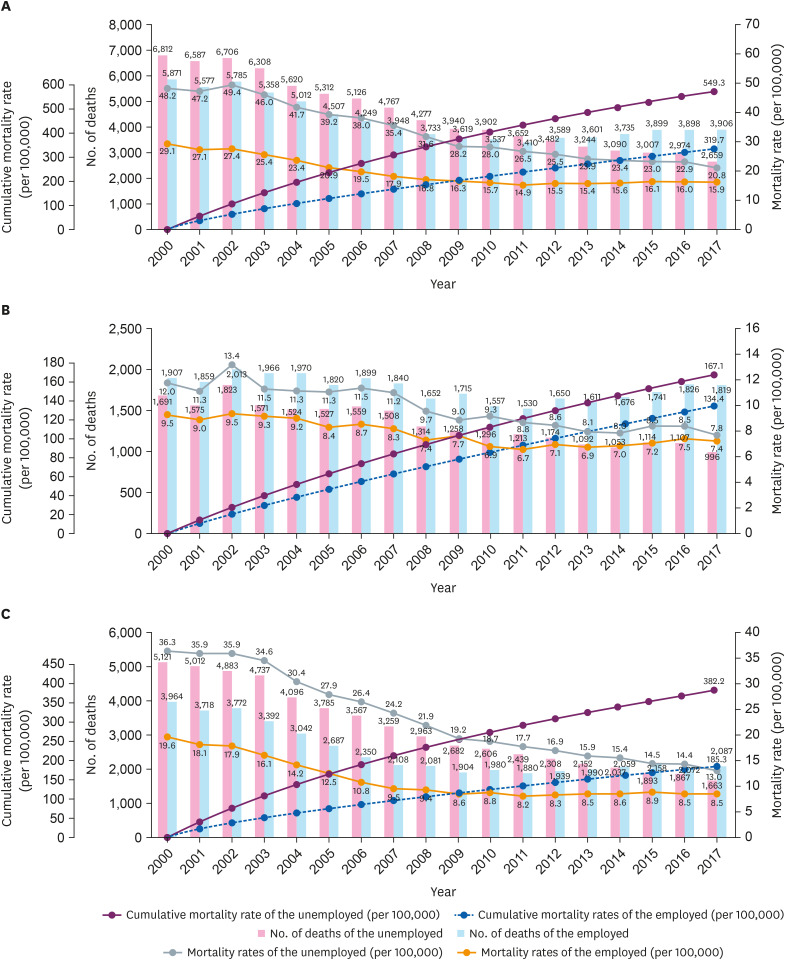
Numbers of deaths, mortality rates, and cumulative mortality rates per year (2000–2017) of the unemployed and employed. (A) Cardiovascular and cerebrovascular diseases, (B) cardiovascular disease, and (C) cerebrovascular disease.
DISCUSSION
Based on previous findings, the WHO/ILO has proposed two possible mechanisms by which long work hours affect CCVDs.7,8 Working for long hours can increase the risk of CCVDs by causing adverse health behaviors, such as smoking, alcohol consumption, inadequate diet, and lack of physical activity, as well as sleep disturbances and poor recovery. In addition, high-intensity repetitive work accelerates the autonomic nervous system and stress pathways, such as the sympathetic-adrenal axis and the hypothalamus-pituitary-adrenal axis, to release stress hormones excessively. When the stress pathway is repeatedly activated over a long period of time, persistent hypertension due to decreased heart rate control and sympathovagal balance disorder and structural lesions of the cardiovascular system, such as coronary atherosclerotic lesions, can occur, which can increase the risk of CCVDs.
In Fig. 1, the number of industrial accident applications due to CCVDs continued to decline from 2006 to 2017. According to the Ministry of Employment and Labor’s survey report on the status of working conditions by type of employment, the average monthly working hours of wage workers in Korea decreased from 193.4 hours in 2006 to 152.4 hours in 2019.42 According to the Korean Working Conditions Survey, the proportion of wage workers working more than 45 hours a week decreased from 53.1% in 2006 to 47.9% in 2010,43,44 and the proportion of wage workers working more than 53 hours a week decreased from 18.8% in 2014 to 12.9% in 2017.45,46 It is speculated that the decline in the average working hours of wage workers affected reducing the number of industrial accident applications during the period. In addition, the CCVD mortality rate of the employed decreased from 10.8 per 100,000 to 8.5 per 100,000 from 2006 to 2017 (Fig. 2C). This decrease may also be associated with a reduction in the number of industrial accident applications. In other words, it is possible that the employee did not submit an industrial accident application if they return to work even after a CCVD has occurred. In cases of the death of workers, on the other hand, their bereaved may have applied more aggressively, so the decrease in the CCVD mortality rate may have affected the reduced number of industrial accident applications. The increase in the number of industrial accident applications from 2018 appears to have been influenced by the rise in the industrial accident approval rate due to the introduction of the principle of estimation in 2017 and the easing of standards for recognition in 2018, which has led to an increase in the awareness of the Industrial Accident Compensation Insurance Compensation System regarding CCVDs.
The approval rate of CCVDs as occupational diseases continued to decline from 2000 to 2006, and there were no changes in standards for recognition during this period. A study that analyzed precedents related to CCVDs as industrial accidents reported that the defeat rate of the Korea Workers’ Compensation and Welfare Service (KCOMWEL) in administrative lawsuits filed by workers disobeying the administrative disposition decisions of the KCOMWEL decreased from 52.5% in 1999 to 17.0% in 200423. The decline in the approval rate during this period without a change in standards for recognition may also be attributable to the court’s improved confidence in the administrative disposition of the KCOMWEL. The approval rate of CCVDs as occupational diseases that reached a plateau in 2006–2007 declined significantly in 2008. In July 2008, the standards for recognition were tightened by removing the provision that recognized cerebral hemorrhage as an occupational disease. The Occupational Disease Review Commission has been established in July 2008. It also may have affected the decrement in occupational disease approval rates.47 In 2012, the occupational disease approval rate increased by 2.3%p compared to that of the previous year, which was due to improvements to the deliberation system of the Occupational Disease Review Commission, such as the division of specialists by disease to participate in the deliberation of the Occupational Disease Review Commission along the disease determination procedure in 2011.48 In 2013, the occupational disease approval rate rose by 5.8%p compared to that of the previous year, which appears to be attributable to the effect of relaxing the standards for recognition, such as the addition of work-hour criteria to the standards for recognition of chronic overwork. The increase in the approval rate of CCVDs as occupational diseases in 2017 was due to the relaxation or change in the burden of proof borne by the applicant (worker) through the application of the principle that “if the criteria set forth in the specific standards for recognition are met, it shall be recognized as an occupational disease unless disproved.”
A study analyzing Karoshi cases found that when the revised CCVD standards for recognition were implemented, the industrial accident approval rate in 2018 was not as high as that in 2017 when working hours per week were less than 52 hours and more than 60 hours. However, in more than 52-hour and less than 60-hour of work-hour, the approval rate increased by 22.7%p.49 This could have occurred because the working hours corresponding to chronic overwork in 2018 were subdivided based on 52 hours, and the work relevance was judged by considering the weighting factors of the workload. According to a Korean report on the approval of overwork and CCVDs as industrial accidents, the industrial accident approval rate of CCVDs caused not only by chronic overwork but also by short-term overwork increased from January to December 2020 compared from February 2013 to June 2016.38,50 This increase seemed to be due to the removal of the provision in the standards for recognition in 2018 that the health status of workers should be considered. The approval rate, which was 41.3% in 2018, decreased slightly from 41.2% in 2019 to 38.2% in 2020, and the number of applications decreased from 3,077 to 2,429. The revision of the Labor Standard Act in 2018 reduced the statutory maximum working hours. The average working hours decreased as the workplaces covered by the revised Labor Standard Act gradually expanded. The decline in the number of industrial accident applications and the rate of applications after 2019 appears to be because of these revisions.
In Fig. 2, the CCVD mortality rates of the unemployed and employed tended to decline over time from 2000 to 2017. The overall reduction in CCVD mortality rate seems to be due to the management of underlying diseases such as hypertension, diabetes, and hyperlipidemia as well as improvement of lifestyle and increase in the effectiveness of therapeutic interventions.51 The CCVD cumulative mortality rate of the unemployed was higher than that of the employed, and the difference grew larger over the years. As shown in Fig. 1, various changes in policies regarding CCVDs in workers may have not only changed the occupational disease approval rate but may have also contributed to lowering the cumulative CCVD death rate of the employed. However, there are some statistical limitations in this study. For example, this study may have overestimated the difference in the cumulative mortality rate between the employed and unemployed because the employment status may be changed. Some employed persons may have changed to an unemployed status when their health deteriorates, which means they became vulnerable to death from CCVDs. A healthy worker effect may be another reason for overestimating. No data were available to calculate the CCVD incidence or mortality rate of a group of workers covered by the Industrial Accident Compensation Insurance Act, so we compared the CCVD cumulative mortality rate between the unemployed and employed in this study. Further studies using CCVD statistics of workers that are covered by the Industrial Accident Compensation Insurance should be performed to analyze the approval statistics.
CONCLUSIONS
CCVDs are recognized as occupational diseases in Korea. The approval rate of CCVDs as occupational diseases has fluctuated with the revision of occupational disease standards for recognition, the introduction of the Occupational Disease Review Commission system, the introduction of the principle of estimation, and the reduction of average working hours. CCVDs pose a high economic burden but are preventable. Strategic approaches, such as ongoing prevention initiatives, are needed to prevent CCVDs in workers.
Abbreviations
CCVD
cardiovascular and cerebrovascular disease
ILO
International Labour Organization
KCOMWEL
Korea Workers’ Compensation and Welfare Service
OECD
Organisation for Economic Co-operation and Development
WHO
World Health Organization
-
Competing interests: The authors declare that they have no competing interests.
-
Author contributions:
Conceptualization: Kim UJ, Choi WJ, Lee J, Kim Y, Kim I.
Data curation: Kim UJ, Han E, Lee S.
Formal analysis: Kim UJ, Lee Y, Han E.
Investigation: Kim UJ, Kim I, Ham S, Choi WJ, Kang SK.
Methodology: Lee W.
Software: Kim UJ, Lee W.
Validation: Kim Y, Ham S, Choi WJ, Lee W.
Visualization: Kim UJ.
Writing - original draft: Kim UJ.
Writing - review & editing: Choi WJ, Lee W, Kang SK, Kim Y, Kim I.
NOTES
SUPPLEMENTARY MATERIALS
Supplementary Table 1
Summary of standards for recognition of cardiovascular and cerebrovascular diseases as occupational diseases (Public Notice by the Ministry of Employment and Labor No. 2020-155)
Supplementary Table 2
Reasons for introducing workload weighting factors for cardiovascular and cerebrovascular diseases
- 1. Korea Legislation Research Institute. Article 2. Definitions, Labor Standards Act. Updated 2021]. Accessed March 21, 2022]. https://elaw.klri.re.kr/kor_service/lawView.do?hseq=56543&lang=ENG .
- 2. Korea Legislation Research Institute. Article 51. Flexible Work Hours System within Three Months, Labor Standards Act. Updated 2021]. Accessed March 21, 2022]. https://elaw.klri.re.kr/kor_service/lawView.do?hseq=56543&lang=ENG .
- 3. Organisation for Economic Co-operation and Development Statistics. Average annual hours actually worked per worker. Updated 2021]. Accessed March 16, 2022]. https://stats.oecd.org/ .
- 4. Eguchi H, Wada K, Smith DR. Recognition, compensation, and prevention of karoshi, or death due to overwork. J Occup Environ Med 2016;58(8):e313–e314. 27500999.ArticlePubMed
- 5. Nishiyama K, Johnson JV. Karoshi--death from overwork: occupational health consequences of Japanese production management. Int J Health Serv 1997;27(4):625–641. 9399110.ArticlePubMedPDF
- 6. Uehata T. Study of Karoshi (the first report): examination of 17 cases in different occupations. Jpn J Ind Health 1978;20:479.
- 7. Li J, Pega F, Ujita Y, Brisson C, Clays E, Descatha A, et al. The effect of exposure to long working hours on ischaemic heart disease: a systematic review and meta-analysis from the WHO/ILO Joint Estimates of the Work-related Burden of Disease and Injury. Environ Int 2020;142:105739. 32505014.ArticlePubMedPMC
- 8. Descatha A, Sembajwe G, Pega F, Ujita Y, Baer M, Boccuni F, et al. The effect of exposure to long working hours on stroke: a systematic review and meta-analysis from the WHO/ILO Joint Estimates of the Work-related Burden of Disease and Injury. Environ Int 2020;142:105746. 32505015.ArticlePubMed
- 9. Ministry of Employment and Labor (MOEL). The Second Five-Year Plan for Industrial Accident Prevention Plan. Sejong, Korea: MOEL; 2004.
- 10. Korea Legislation Research Institute. Article 669. Measures to Prevent Health Problems Caused by Job Stress, Rules on Occupational Safety and Health Standards. Updated 2021]. Accessed April 6, 2022]. https://www.law.go.kr/%EB%B2%95%EB%A0%B9/%EC%82%B0%EC%97%85%EC%95%88%EC%A0%84%EB%B3%B4%EA%B1%B4%EA%B8%B0%EC%A4%80%EC%97%90%EA%B4%80%ED%95%9C%EA%B7%9C%EC%B9%99 .
- 11. Korea Legislation Research Institute. Article 44. Scope of Occupational Disease, etc., Enforcement Decree of the Labor Standards Act. Updated 2019]. Accessed March 21, 2022]. https://elaw.klri.re.kr/kor_service/lawView.do?hseq=51770&lang=ENG .
- 12. Korea Legislation Research Institute. Article 36. Categories of Insurance Benefits and Standards for Their Calculation, Industrial Accident Compensation Insurance Act. Updated 2021]. Accessed March 21, 2022]. https://elaw.klri.re.kr/kor_service/lawView.do?hseq=56558&lang=ENG .
- 13. Korea Legislation Research Institute. Article 34. Standards for Recognition of Occupational Diseases, Enforcement Decree of the Industrial Accident Compensation Insurance Act. Updated 2019]. Accessed March 21, 2022]. https://elaw.klri.re.kr/kor_service/lawView.do?hseq=52116&lang=ENG .
- 14. Korea Legislation Research Institute. Article 39. Occupational Disease or Death Caused by an Occupational Disease, Enforcement Rule of the Industrial Accident Compensation Insurance Act (1995.4.29 revision). Updated 1995]. Accessed June 11, 2022]. https://www.law.go.kr/lsInfoP.do?lsiSeq=11122&ancYd=19950429&ancNo=00097&efYd=19950501&nwJoYnInfo=N&efGubun=Y&chrClsCd=010202&ancYnChk=0#AJAX .
- 15. Korea Legislation Research Institute. Article 39. Occupational Disease or Death Caused by an Occupational Disease, Enforcement Rule of the Industrial Accident Compensation Insurance Act (1996.3.19 revision). Updated 1996]. Accessed June 11, 2022]. https://www.law.go.kr/lsInfoP.do?lsiSeq=611&ancYd=19960319&ancNo=00107&efYd=19960321&nwJoYnInfo=N&efGubun=Y&chrClsCd=010202&ancYnChk=0#0000 .
- 16. Korea Legislation Research Institute. Article 39. Occupational Disease or Death Caused by an Occupational Disease, Enforcement Rule of the Industrial Accident Compensation Insurance Act (1999.10.7 revision). Updated 1999]. Accessed June 11, 2022]. https://www.law.go.kr/lsInfoP.do?lsiSeq=50194&ancYd=19991007&ancNo=00157&efYd=19991007&nwJoYnInfo=N&efGubun=Y&chrClsCd=010202&ancYnChk=0#0000 .
- 17. Korean Enforcement Decree of the Industrial Accident Compensation Insurance Act and Public Notice of What is Necessary to Determine Approval for Cerebro-Cardiovascular Disease and Musculoskeletal Disease as Occupational Diseases (2008.7.1). Updated 2008]. Accessed June 11, 2022]. https://www.law.go.kr/LSW//admRulInfoP.do?admRulSeq=2308 .
- 18. Korean Enforcement Decree of the Industrial Accident Compensation Insurance Act and Public Notice of What Is Necessary to Determine Approval for Cerebro-Cardiovascular Disease and Musculoskeletal Disease as Occupational Diseases (2009.9.25 revision). Updated 2009]. Accessed June 11, 2022]. https://www.law.go.kr/LSW//admRulInfoP.do?admRulSeq=2000000021544 .
- 19. Korean Enforcement Decree of the Industrial Accident Compensation Insurance Act and Public Notice of What Is Necessary to Determine Approval for Cerebro-Cardiovascular Disease and Musculoskeletal Disease as Occupational Diseases (2013.6.28 revision). Updated 2013]. Accessed June 11, 2022]. https://www.law.go.kr/LSW//admRulInfoP.do?admRulSeq=2000000094765 .
- 20. Korean Enforcement Decree of the Industrial Accident Compensation Insurance Act and Public Notice of What Is Necessary to Determine Approval for Cerebro-Cardiovascular Disease and Musculoskeletal Disease as Occupational Diseases (2017.12.29 revision). Updated 2017]. Accessed June 11, 2022]. https://www.law.go.kr/LSW//admRulInfoP.do?admRulSeq=2100000107994 .
- 21. Korean Enforcement Decree of the Industrial Accident Compensation Insurance Act and Public Notice of What Is Necessary to Determine Approval for Cerebro-Cardiovascular Disease and Musculoskeletal Disease as Occupational Diseases (2020.12.29 revision). Updated 2020]. Accessed June 11, 2022]. https://www.law.go.kr/LSW//admRulInfoP.do?admRulSeq=2100000196483 .
- 22. Ministry of Employment and Labor (MOEL). 2020 Industrial Accident Insurance Yearbook. Sejong, Korea: MOEL; 2021.
- 23. Ha EH, Kim SG, Yun CS, Yu SJ, Yi CH, Kim YK, et al. Study on the Approval Criteria of Neuro-Cardiovascular Disease Due to Occupational Cases. Sejong, Korea: Ministry of Employment and Labor; 2005.
- 24. Won JU, Kim SG, Im HJ, Kim HR. A Study on the Overwork Criteria for Cerebro-Cardiovascular Disease. Sejong, Korea: Ministry of Employment and Labor; 2008.
- 25. Korean Statistical Information Service (KOSIS). Numbers of deaths by cause of death/sex/occupation. Updated 2021]. Accessed June 12, 2022]. https://kosis.kr/statHtml/statHtml.do?orgId=101&tblId=DT_1B34E05&vw_cd=MT_ZTITLE&list_id=F_27&scrId=&seqNo=&lang_mode=ko&obj_var_id=&itm_id=&conn_path=MT_ZTITLE&path=%252FstatisticsList%252FstatisticsListIndex.do .
- 26. Korean Statistical Information Service (KOSIS). Numbers of deaths and mortality rates by cause of death/sex/age. Updated 2022]. Accessed June 12, 2022]. https://kosis.kr/statHtml/statHtml.do?orgId=101&tblId=DT_1B34E07&vw_cd=MT_ZTITLE&list_id=F_27&scrId=&seqNo=&lang_mode=ko&obj_var_id=&itm_id=&conn_path=MT_ZTITLE&path=%252FstatisticsList%252FstatisticsListIndex.do .
- 27. Korean Statistical Information Service (KOSIS). Numbers of the employed by sex/age. Updated 2022]. Accessed June 11, 2022]. https://kosis.kr/statHtml/statHtml.do?orgId=101&tblId=DT_1DA7024S&vw_cd=MT_ZTITLE&list_id=B17&scrId=&seqNo=&lang_mode=ko&obj_var_id=&itm_id=&conn_path=MT_ZTITLE&path=%252FstatisticsList%252FstatisticsListIndex.do .
- 28. Korean Statistical Information Service (KOSIS). Resident registered population by administrative district/age (1992~2010). Updated 2022]. Accessed August 24, 2022]. https://kosis.kr/statHtml/statHtml.do?orgId=101&tblId=DT_1B04005&vw_cd=MT_ZTITLE&list_id=A_7&scrId=&seqNo=&lang_mode=ko&obj_var_id=&itm_id=&conn_path=MT_ZTITLE&path=%252FstatisticsList%252FstatisticsListIndex.do .
- 29. Korean Statistical Information Service (KOSIS). Resident registered population by administrative district/age (2011~). Updated 2022]. Accessed August 24, 2022]. https://kosis.kr/statHtml/statHtml.do?orgId=101&tblId=DT_1B04005N&vw_cd=MT_ZTITLE&list_id=A_7&scrId=&seqNo=&lang_mode=ko&obj_var_id=&itm_id=&conn_path=MT_ZTITLE&path=%252FstatisticsList%252FstatisticsListIndex.do .
- 30. Korean Statistical Information Service (KOSIS). Resident registration mid-year population by administrative district/sex/age. Updated 2022]. Accessed June 29, 2022]. https://kosis.kr/statHtml/statHtml.do?orgId=101&tblId=DT_1B040M1&vw_cd=MT_ZTITLE&list_id=A_7&scrId=&seqNo=&lang_mode=ko&obj_var_id=&itm_id=&conn_path=MT_ZTITLE&path=%252FstatisticsList%252FstatisticsListIndex.do .
- 31. Statistics Korea. Population Trend Survey - Statistics Information Report. Daejeon, Korea: Statistics Korea; 2021.
- 32. Statistics Korea. Economically Active Population Survey - Statistics Information Report. Daejeon, Korea: Statistics Korea; 2022.
- 33. Coviello V, Boggess M. Cumulative incidence estimation in the presence of competing risks. Stata J 2004;4(2):103–112.ArticlePDF
- 34. Goel MK, Khanna P, Kishore J. Understanding survival analysis: Kaplan-Meier estimate. Int J Ayurveda Res 2010;1(4):274–278. 21455458.ArticlePubMedPMC
- 35. Lee H. A study on approval criteria of occupational accident in the accident from overwork. Labor Law Forum 2009;2(2):138–174.
- 36. Korean Supreme Court Decision 1991 Nu 10015, Decided April 14, 1992.
- 37. Korean Supreme Court Decision 1992 Nu 16553, Decided February 12, 1993.
- 38. Choi WJ, Kim YG, Kim I, Lee MJ, Lee W, Lee J. The Standards for Recognition of Cerebro-Cardiovascular Diseases and the Determination of Additional Burden Factors. Sejong, Korea: Ministry of Employment and Labor; 2021.
- 39. Song J, Kim SG, Kim YK, Kim I, Sakong J, Ahn YS, et al. A Study on the Standards for Recognition of Occupational Diseases and Improvement of Disaster Investigation. Sejong, Korea: Ministry of Employment and Labor; 2017.
- 40. Kwon YJ, Kim SG, Won JU, Im HJ, Kim I. Research on the criteria for Recognizing Civil Servants’ Diseases Under the Military Pension Act. Seoul, Korea: Ministry of National Defense; 2012.
- 41. Ministry of Employment and Labor (MOEL). 2011 Industrial Accident Insurance Yearbook. Sejong, Korea: MOEL; 2012.
- 42. Ministry of Employment and Labor (MOEL). Survey Report on Labor Conditions by Employment Type. Sejong, Korea: MOEL; 2019.
- 43. Occupational Safety and Health Research Institute (OSHRI). The Results of 1st Korean Working Conditions Survey. Ulsan, Korea: OSHRI; 2006.
- 44. Occupational Safety and Health Research Institute (OSHRI). The Results of 2nd Korean Working Conditions Survey. Ulsan, Korea: OSHRI; 2010.
- 45. Occupational Safety and Health Research Institute (OSHRI). The Results of 4th Korean Working Conditions Survey. Ulsan, Korea: OSHRI; 2014.
- 46. Occupational Safety and Health Research Institute (OSHRI). The Results of 5th Korean Working Conditions Survey. Ulsan, Korea: OSHRI; 2017.
- 47. Park J, Kwon YJ, Kim I. A Study on the Measures to Mitigate the Burden of Proving Industrial Accident Workers Through the Analysis of the Operation Status of the Nursing Care System. Sejong, Korea: Ministry of Employment and Labor; 2012.
- 48. Ministry of Employment and Labor (MOEL). 2012 Industrial Accident Insurance Yearbook. Sejong, Korea: MOEL; 2013.
- 49. Kim K. Case Study of Care Decision for Overworking Death. Ulsan, Korea: Korea Workers Compensation & Welfare Service; 2020.
- 50. Kim I, Kwon D, Kim HR, Yoo S, Youn K, Lee HE, et al. Policy Study to Prevent Overwork Death (Overwork Suicide). Ulsan, Korea: Korea Occupational Safety and Health Agency; 2017.
- 51. Baek J, Lee H, Lee HH, Heo JE, Cho SM, Kim HC. Thirty-six year trends in mortality from diseases of circulatory system in Korea. Korean Circ J 2021;51(4):320–332. 33821581.ArticlePubMedPMCPDF
REFERENCES
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Toward a Psychosocial Risk Management Standard for U.S. Workplaces: A Qualitative Evaluation of International Policies
A. Michael Ierardi, Diana Romero
Occupational Health Science.2026;[Epub] CrossRef - List of occupational diseases among farmers in Korea: a literature review
Hansoo Song, Seok-Ju Yoo, Won-Ju Park, Seunghyeon Cho, Ki Soo Park, Joo Hyun Sung, Sang Jin Park, Seong-yong Yoon, Kyeongsoo Kim, Dong-phil Choi, Hye-min Kim, Bounggyun Ju, Kanwoo Youn
Ann Occup Environ Med.2025; 37: e2. CrossRef - Association of long working hours with visceral adiposity index, anthropometric indices, and weight management behaviors: a study of Korean workers
Seong-Uk Baek, Jin-Ha Yoon
Family Practice.2025;[Epub] CrossRef - Association between long working hours and the development of suicidal ideation among female workers: An 8-year population-based study using the Korean Longitudinal Survey of Women & Family (2012–2020)
Seong-Uk Baek, Yu-Min Lee, Jin-Ha Yoon
Psychiatry Research.2024; 333: 115731. CrossRef - Association between long working hours and diet quality and patterns: A latent profile analysis of a nationally representative sample of Korean workers
Seong-Uk Baek, Jong-Uk Won, Yu-Min Lee, Jin-Ha Yoon
Preventive Medicine.2024; 180: 107890. CrossRef - Is Farming a Risk Occupation for Cardio-cerebrovascular Diseases? A Scoping Review on Cardio-cerebrovascular Disease Risk in Farmers
Hyeonjun Kim, Wongeon Jung, Sunjin Jung, Seunghyeon Cho, Inho Jung, Hansoo Song, Ki-Soo Park, Seong-Yong Yoon, Joo Hyun Sung, Seok-Ju Yoo, Won-Ju Park
Journal of Preventive Medicine and Public Health.2024; 57(6): 521. CrossRef - Injury rates and work-related diseases following workforce reduction among South Korean on-site workers in basic local governments between 2016 and 2018
Dongwhan Suh, Nahyun Kim, Han-Na Jung, Woo Chul Jeong, Hyunjoo Kim
Annals of Occupational and Environmental Medicine.2024; 37: e17. CrossRef - Self-Esteem Trajectories After Occupational Injuries and Diseases and Their Relation to Changes in Subjective Health: Result From the Panel Study of Workers’ Compensation Insurance (PSWCI)
Seong-Uk Baek, Won-Tae Lee, Min-Seok Kim, Myeong-Hun Lim, Jin-Ha Yoon, Jong-Uk Won
Journal of Korean Medical Science.2023;[Epub] CrossRef
 Cite
CiteStandards for recognition and approval rate of occupational cerebro-cardiovascular diseases in Korea

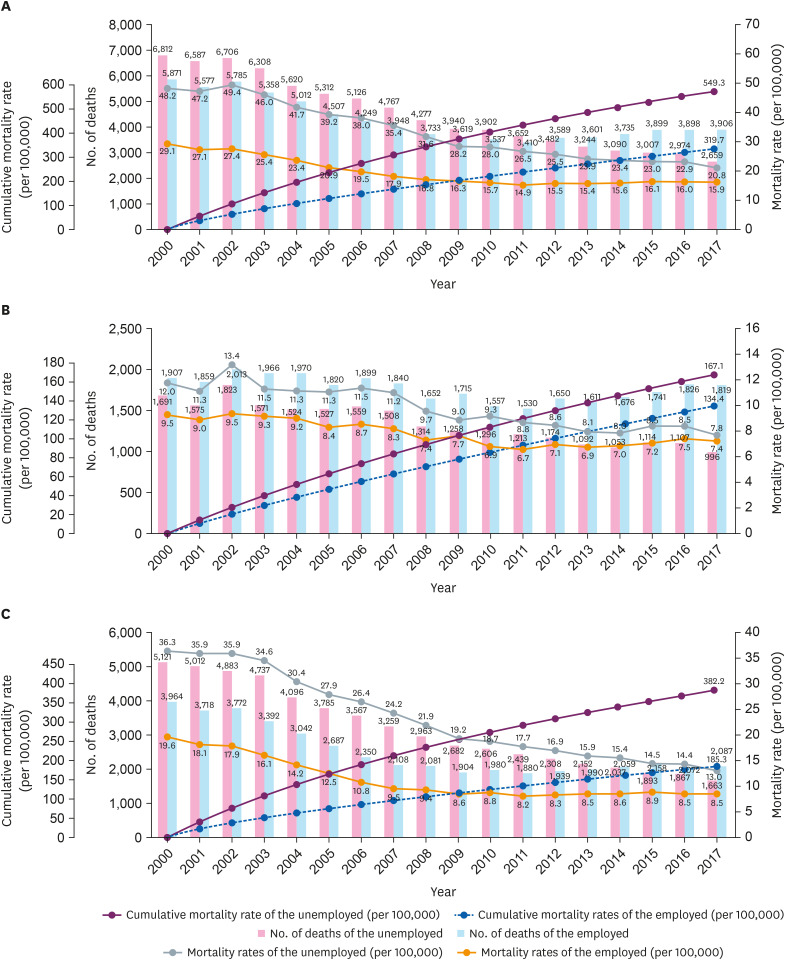
Fig. 1 Numbers of applications and approvals of CCVDs as occupational diseases per year and their approval rate as well as numbers of workers covered by the Industrial Accident Compensation Insurance (2000–2020).aIn July 2008, the standards for recognition of CCVDs were tightened (removing the provision that recognized cerebral hemorrhage as an occupational disease in the course of work) and the Occupational Disease Review Commission system was introduced; bIn July 2013, the standards for recognition of CCVDs were relaxed (working hours added); cIn September 2017, the principle of estimation was applied; and dIn January 2018, the standards for recognition of CCVDs were relaxed (eliminating the duty for health status considerations of short-term overwork workers, subdividing standard time for chronic overwork, and taking into account weighting factors of workload and night shifts).CCVD: cardiovascular and cerebrovascular disease.
Fig. 2 Numbers of deaths, mortality rates, and cumulative mortality rates per year (2000–2017) of the unemployed and employed. (A) Cardiovascular and cerebrovascular diseases, (B) cardiovascular disease, and (C) cerebrovascular disease.
Fig. 1
Fig. 2
Standards for recognition and approval rate of occupational cerebro-cardiovascular diseases in Korea
| Revision date | Legal basis | Changes |
|---|---|---|
| 8.27.1982 | The established rule of the Ministry of Labor, No. 71 | • Enactment of standards for recognition of occupational accidents. |
| • Only stroke and sudden cardiac death that were apparently caused by an occupational injury or by occupational work were to be recognized. | ||
| • Occupational factors had to be a sufficient cause of disease onset to be recognized. | ||
| 10.20.1983 | The established rule of the Ministry of Labor, No. 92 | • Recognition of CCVDs when workers with predispositions or underlying diseases develop central nervous system disorders and circulatory diseases in connection with their work. |
| • Recognition of CCVDs as occupational accidents even when hypertension has developed in relation to work or when an existing disease has been triggered or exacerbated. | ||
| 12.5.1989 | The established rule of the Ministry of Labor, No. 167 | • If intraparenchymal hemorrhage or subarachnoid hemorrhage occurs in the course of work, it is recognized as an occupational disease even if there is an existing disease. |
| 5.6.1993 | The established rule of the Ministry of Labor, No. 234 | • Expansion of the scope of recognition to include intraparenchymal hemorrhage, subarachnoid hemorrhage, cerebral infarction, hypertensive encephalopathy, primary cardiac arrest, angina, and myocardial infarction. |
| 7.21.1994 | The established rule of the Ministry of Labor, No. 247 | • Relaxation of the standards of recognition of CCVDs as occupational accidents when they occur in the course of work unless there is clear medical evidence that they were spontaneous. |
| • Primary cardiac arrest was excluded from the list of recognized diseases (only intraparenchymal hemorrhage, subarachnoid hemorrhage, cerebral infarction, hypertensive encephalopathy, angina, and myocardial infarction were accepted). | ||
| • “Rapid changes in the working environment” and “chronic overwork” were to be considered. | ||
| • Quantitative representation of chronic overwork. | ||
| 5.1.1995 | Enforcement Regulation of the Industrial Accident Compensation Insurance Act, Appendix 1 | • Integration of the standards for recognition as an occupational accident from the established rule of the Ministry of Labor into the Enforcement Regulation of the Industrial Accident Compensation Insurance Act. |
| • Standards for recognition of CCVDs as occupational accidents were divided into standards for recognition of occupational accidents and occupational diseases. | ||
| • Stricter standards such as, “a disease shall be deemed to be an occupational disease if it is medically proven that the cause of a disease or death from the same disease during the performance of the work has not worsened spontaneously” were developed. | ||
| 3.19.1996 | Enforcement Regulation of the Industrial Accident Compensation Insurance Act, Appendix 1 | • Standards relaxed again by the recognition of cerebral hemorrhage as an occupational disease “in the event of the onset or death of cerebral hemorrhage in the course of work, unless clearly demonstrated medically that it worsened spontaneously.” |
| 10.7.1999 | Enforcement Regulation of the Industrial Accident Compensation Insurance Act, Appendix 1 | • Addition of dissecting aortic aneurysm (intraparenchymal hemorrhage, subarachnoid hemorrhage, cerebral infarction, hypertensive encephalopathy, angina, myocardial infarction, and dissecting aortic aneurysm). |
| 7.1.2008 | Public Notice by the Ministry of Labor, No. 2008-43 | • Deletion of the phrase “occur while performing work” from the standards for recognition of intraparenchymal hemorrhage and subarachnoid hemorrhage. |
| • Removal of diseases that were not specifically eventualized because it was detected before severe deterioration of the underlying pathogenesis, such as hypertensive encephalopathy and angina. | ||
| 9.25.2009 | Public Notice by the Ministry of Employment and Labor, No. 2009-38 | • Addition of deadline for reconsideration (5 years). |
| 6.28.2013 | Public Notice by the Ministry of Employment and Labor, No. 2013-32 | • Changes in the degree of work from “the degree to which the work intensity, responsibilities, and work environment within 1 week before the onset of the disease is difficult for the general public to adapt to” to “the degree that it is difficult for even the same kind of workers who perform similar tasks to adapt.” |
| • A statement was added that whether the CCVD falls under the “occupational burden for a short period of time” is to be judged by combining the characteristics of the work and workers. | ||
| • Contents of working hours (average of 60 hours per week for 12 weeks before onset or 64 hours per week for 4 weeks before onset) was added in the section regarding chronic heavy work. | ||
| • Changes in the deadline for reconsideration to 3 years. | ||
| 7.1.2016 | Public Notice by the Ministry of Employment and Labor, No. 2016-25 | • Reconsideration deadline: 3 years → changed to every 3 years. |
| 12.29.2017 | Public Notice by the Ministry of Employment and Labor, No. 2017-117 | • Changes to workers’ health were not to be considered in short-term overwork. |
| • Standard time for chronic overwork expanded to three levels. | ||
| • Specification of the weighting factors of workload such as shift work. | ||
| • Because night work imposes a more physical and mental burden, 30% of daytime working hours is to be added when calculating working hours. | ||
| 12.29.2020 | Public Notice by the Ministry of Employment and Labor, No. 2020-155 | • Revised the basis of the deadline for reconsideration as January 1, 2021. |
Table 1 Revision history of standards for the approval of CCVDs as occupational diseases
CCVD: cardiovascular and cerebrovascular disease.

