
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 34; 2022 > Article
- Original Article Association between coronavirus disease 2019-related workplace interventions and prevalence of depression and anxiety
-
Hyun Woo Park
 , Seung Hyun Park, Young Wook Kim, JunSeok Son, Chan Woo Kim, Hyoung Ouk Park, Jun Ho Lee, Young Hoo Shin, Chang Ho Chae, Eui Yup Chung, Hun Jeong
, Seung Hyun Park, Young Wook Kim, JunSeok Son, Chan Woo Kim, Hyoung Ouk Park, Jun Ho Lee, Young Hoo Shin, Chang Ho Chae, Eui Yup Chung, Hun Jeong -
Annals of Occupational and Environmental Medicine 2022;34:e11.
DOI: https://doi.org/10.35371/aoem.2022.34.e11
Published online: June 3, 2022
Department of Occupational and Environmental Medicine, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon, Korea.
- Correspondence: Seung Hyun Park. Department of Occupational and Environmental Medicine, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, 158 Paryong-ro, Masanhoewon-gu, Changwon 51353, Korea. baramkal476@naver.com
• Received: March 22, 2022 • Revised: April 29, 2022 • Accepted: May 17, 2022
Copyright © 2022 Korean Society of Occupational & Environmental Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background Although coronavirus disease 2019 is causing a variety of psychological problems for workers, there are few longitudinal studies on changes in workers’ mental health by workplace intervention. This study aimed to evaluate the change in the prevalence of depression and anxiety according to the active involvement of the workplace.
-
Methods This study was conducted on 1,978 workers at a workplace who underwent a health screening from January 2019 to August 2020, and classified depression and anxiety disorders using a self-report questionnaire. After the first pandemic, the company stopped health screening, took paid leave and telecommuting, and conducted interventions such as operating its own screening clinic. To see if this workplace intervention affects workers’ mental health, we conducted generalized estimating equations to compare odds ratio (OR).
-
Results In the pre-intervention group, 384 people (16.86%) had depression, and 507 people (22.26%) had anxiety disorder. Based on the OR before intervention, the OR of depression decreased to 0.76 (0.66–0.87) and the OR of anxiety disorder decreased to 0.73 (0.65–0.82).
-
Conclusions As a result of this study, it was confirmed that workplace intervention was related to a decrease in depression and anxiety. This study provides basic data to improve workers’ mental health according to workplace intervention, and further research is needed according to workplace intervention in the future.
BACKGROUND
Coronavirus disease 2019 (COVID-19) continues to have direct and indirect effects on all aspects of modern society,1 which has led to a surge of studies on physical and mental health associated with the pandemic. A study based on 5,683 data sources estimated that the COVID-19-related increase in the global average prevalence of major depressive disorder was 27.6% (range: 25.1–30.3) and that of anxiety disorder was 25.6% (range: 23.2–28.0).2 Since the main transmission routes of COVID-19 are respiratory droplets and close contact, patients with confirmed infection are kept in isolation3,4 and provided treatment in an isolated environment.5 Concerns about infection and preventive measures such as social distancing have been found to have a negative psychological impact on the affected individuals.6,7
Proper management of depression is crucial because, if left untreated, depression can lead to low quality of life, dysfunction in the workplace, and even suicide, resulting in direct and indirect economic costs to society.8 Internet-based cognitive behavioral therapy9,10,11 and guided self-help intervention based on cognitive behavioral therapy12,13 can be applied in cases of persistent subthreshold depression or mild-to-moderate depression. Combined pharmacotherapy and psychosocial treatment is also known to be effective for patients requiring medication.14 In the same vein, relaxation therapy and cognitive behavioral therapy can be used first for mild anxiety as non-pharmacological treatment.15 These psychological interventions not only help improve the mental health of patients by relieving their depression and anxiety but also help prevent impairment of immunity induced by depression and anxiety.16
In previous studies, counseling has been associated with alleviation of depression and anxiety symptoms17; telecommuting, with reducing depression, stress, and fatigue18; and long paid leave, with a decrease in the prevalence of depression in women.19 Since these management practices cannot be implemented at an individual level, systematic and organizational workplace interventions are needed to ensure effective outcomes. This study aimed to investigate the effects of workplace mental health management interventions, telecommuting, and paid leave in the pandemic environment on the risk of depression and anxiety in the employees.
METHODS
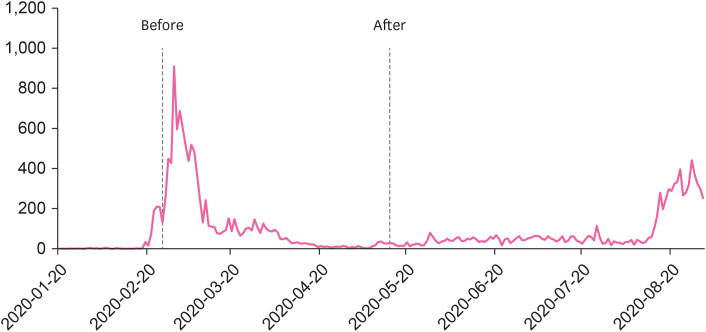
The participants of this retrospective case-control study, using health screening data, were 5,980 workers in Daegu and Gyeongbuk areas who underwent health screening at a university hospital in Changwon from January 2019 to August 2020. After excluding 3,879 workers who did not undergo health screenings for two consecutive years and 123 workers with missing data, a total of 1,978 workers were selected as the final study participants. After the first pandemic that began in Daegu and Gyeongbuk, the examination was stopped and workplace intervention was conducted, and based on this, it was classified into the pre-intervention and post-intervention group. A total of 1,978 workers were examined in 2020, 300 from January 1st to February 25th, 2020, and 1,578 after May 14th to August 31st, 2020 (Fig. 1).
A structured self-report questionnaire was used to collect information about the participants’ age, body mass index (BMI), and medical history as well as lifestyle habits such as exercise history, smoking history, and alcohol consumption history. BMI values of ≥ 25 kg/m2 were classified under obesity in accordance with the World Health Organization’s Asia-Pacific region cut-off for obesity, and individual medical history was checked for hypertension, diabetes, and dyslipidemia. As regards exercise history, the participants were classified into exercise and non-exercise group based on the criteria for moderate-intensity exercise (150 min/week) or high-intensity aerobic exercise (75 min/week) as prescribed in the National Health Insurance Physical Activity Guidelines (ages 18–64 years). For smoking history, the participants were classified into nonsmoker (≤ 5 packs lifetime), former smoker, and current smoker groups according to cumulative pack-year exposure. Drinking habits were classified as high-risk drinking group if the drank more than twice a week and drank 7 glasses (Alchhol content 8 g/cup) a day for men and 5 glasses a day for women, according to the high-risk drinking classification standard set by the National Health and Nutrition Examination Survey.20
The CES-D Scale is a self-report depression scale developed by the U.S. National Institute of Mental Health (NIMH) as a primary screening tool to detect depression in the general population.21 It consists of 20 items (16 negative-statement and 4 positive-statement items), and each item is rated on a 4-point Likert scale, with the total score ranging between 0 and 60 points, whereby a higher total score indicates a higher severity of depression. The severity of depression symptoms is classified into four categories: normal (0–15), mild (16–20), moderate (21–24), and severe (25–60). In this study, 16 points, the cut-off score for mild depression, was applied to divide the participants into the normal group and the depressive symptom group. The reliability and validity of the CES-D were established with the internal consistency value of Cronbach’s α = 0.90.
CUXOS is a self-report anxiety scale designed to assess anxiety severity. This 20-item scale consists of a 6-item psychic anxiety subscale and a 14-item somatic anxiety subscale. Since CUXOS is sensitive to change, it is used for screening or mid-treatment monitoring and evaluation of symptom changes. Each item is rated on a 5-point Likert scale, with the total score ranging between 0 and 80 points, whereby a higher total score indicates a higher severity of anxiety. In Korean version of the CUXOS, the severity of anxiety symptoms was classified into normal (0–25), risk (26–41), high-risk (42–54), and ultrahigh-risk (55–80) groups. In this study, 26 points, the cut-off score for mild anxiety, was applied to divide the participants into the normal group and the anxiety symptom group. The reliability and validity of the Korean version of the CUXOS were established with the internal consistency value of Cronbach’s α = 0.90.22
After the first pandemic of COVID-19, the workplace was closed from February 22 to 24, partially closed from February 29 to March 1, and preemptive paid leave and telecommuting were conducted for a month for workers living in epidemic areas and adjacent areas.
From February 27th to April 10th, we conducted a confirmation test for symptomatic patients at our own screening clinic and consultation with a professional specialist of occupational and environmental medicine if patient wanted, including those with symptoms. We did not conduct follow-up on the workers we consulted. In addition, some people who wanted professional counseling conducted the Internet-guided Cognitive Behavior Therapy after consulting with a psychiatrist, but no additional information could be obtained due to personal information. The medical examination started again from May 14th, and the person who received the medical examination from May 14th to August 31st was set as a post-intervention group.
Descriptive statistical analysis was performed to determine the workplace-specific demographic characteristics and prevalence of depression and anxiety, along with independent t-test and χ2 test, depending on the type of variable. Based on the results, the generalized estimating equations (GEE) was used to determine whether there is workplace-specific difference in the prevalence of depression and anxiety between the test results before and after the COVID-19 pandemic. GEE are useful for estimating causal models for panels and for processing repetitive measurements or time series data, especially when there is no correlation between explanatory and dependent variables or partial correlation is missing. Statistical analysis was performed using STATA for window ver. 16.1(StataCorp., College Station, TX, USA), with the confidence interval (CI) set at 95%, and the significance level at p < 0.05.
The present study protocol was reviewed and approved by the Institutional Review Board of Samsung Changwon Hospital before implementation (approval No. SCMC 2022-02-006) and waived the requirement for informed consent. This was due to the use of anonymized data that were routinely collected as part of a health checkup program.
RESULTS
Table 1 shows the general characteristics of the participants in the pre-intervention group and post-intervention group. The average age of the pre-intervention group was 34.78 ± 7.83 years, consisting of men (n = 1,160; 50.92%) and women (n = 1,118; 49.08%). Anxiety disorders (n = 507; 22.26%), dyslipidemia (n = 247; 15.12%), smoking status (n = 422; 15.67%) showed significant differences in distribution, but depression (n = 384; 16.86%), obesity (n = 728; 31.96%), diabetes (n = 67; 2.94%), risk drinking (n = 783; 34.37%) and physical activity (n = 928; 40.74%) showed no significant difference in distribution.
Table 1
General characteristics of all study participants (n = 1,978)
The average age of the post-intervention group was 33.97 ± 7.29 years, consisting of men (n = 696; 41.48%) and women (n = 982; 58.52%). Anxiety disorders (n = 309; 18.41%), dyslipidemia (n = 231; 16.89%), smoking status (n = 222; 13.23%) showed significant differences in distribution, but depression (n = 247; 14.72%), obesity (n = 580; 34.56%), diabetes (n = 47; 2.80%), risk drinking (n = 610; 36.35%) and physical activity (n = 723; 43.09%) showed no significant difference in distribution (Table 1).
The participants from January 2019 to February 2020 were set as pre-intervention group, and the participants group was set as post-intervention group from May to August 2020 to observe changes in depression and anxiety disorders after intervention. Based on the OR of the pre-intervention group, the OR of the post-intervention group was 0.79 (0.69–0.90) for depression and 0.77 (0.69–0.86) for anxiety disorder, and when the remaining variables were corrected, the values were 0.76 (0.66–0.87) and 0.73 (0.65–0.82) for anxiety disorder were statistically significant (Table 2).
Table 2
OR for depression and anxiety according to company intervention
Adjusted model: adjusted for age, sex, obesity, hypertension, diabetes mellitus, risk drinking, smoking, physical activity.
Pre-intervention: pre-intervention group (for those who underwent health screening from January 2019 to February 2020); Post-intervention: post-intervention group (for those who underwent health screening from March 2020 to August 2020); OR: odds ratio; CI: confidence interval.
In addition, when stratified on gender, the ORs of depression and anxiety disorders in men were 0.70 (0.53–0.91) and 0.79 (0.65–0.95), respectively, and the ORs of depression and anxiety disorders in women were 0.78 (0.66–0.92) and 0.70 (0.60–0.82), respectively (Supplementary Table 1).
DISCUSSION
This study aimed to investigate the effect of active workplace intervention on depression and anxiety after the outbreak of COVID-19 in large-scale local infections for workplace workers. The results showed a significant decrease in depression and anxiety of workers actively intervening in the workplace compared to the previous year before.
Previous studies have demonstrated the effects of pandemics on mental health, such as depression and anxiety. The daily severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection rate and reduced human mobility were associated with an increase in the prevalence of major depressive disorder (regression coefficient [B] 0.9 [95% CI = 0.1–1.8; p = 0.029] for human mobility, 18.1 [95% CI = 7.9–28.3; p = 0.0005] for daily SARS-CoV-2 infection) and anxiety disorder (0.9 [95% CI = 0.1–1.7; p = 0.022] for human mobility, 13.8 [95% CI = 10.7–17.0; p < 0.0001] for daily SARS-CoV-2 infection).2 The increase in the daily infection rate due to the first wave of pandemic, which started in Daegu and Gyeongbuk on February 18, led to reduced mobility to other regions, and the outbreak and consequent limited mobility presumably affected people’s mental health. Further, the number of major depressive disorder patients worldwide increased from 44.8 million to 62.9 million (27.6% increase, 95% CI, 25.1–30.3), and the number of anxiety disorder patients increased from 64.3 million to 90.6 million (25.6% increase, 95% CI, 23.2–30.3).2 In a longitudinal study involving 14,769 Chinese university students, compared with the pre-COVID-19 period (October 2019: depressive symptoms at 1.46%, anxiety symptoms at 1.44%), depression and anxiety symptoms increased by 1,413.01% and 181.94%, respectively, in the wake of the COVID-19 pandemic (April 2020: depressive symptoms at 22.09%, anxiety symptoms at 4.06%).23 According to the global trend, the prevalence of depression and anxiety disorders of workers should increase after COVID-19, but it is believed that the OR of depression and anxiety disorders of workers has decreased due to active intervention in the workplace.
In addition, previous studies also note that active government interventions, such as lockdown during epidemics, have positive effects on mental health, such as depression and anxiety. In a UK-based longitudinal study involving 36,520 adults, conducted from March 23th to August 9th 2020, depression and anxiety symptoms decreased over the 20 weeks following the introduction of lockdown (depressive symptoms: b = –1.93, SE = 0.26, p <0.0001, anxiety symptoms: b = –2.52, SE = 0.28, p < 0.001), most markedly between weeks 2 and 5 of the strict lockdown, but little change was observed in the levels of depression and anxiety between weeks 16 and 20 after the introduction of substantial easing of lockdown.24 Likewise, in Ireland, the prevalence of major depressive disorder and generalized anxiety disorder decreased from 29.8% (95% CI, 17.0–32.6) to 22.8% (95% CI, 20.2–25.3) and from 22.3% (95% CI, 19.7–24.8) to 20.0% (95% CI, 17.6–22.4), respectively, over 6 weeks of lockdown.25 This suggests that active workplace interventions, such as preemptive leave and active implementation of telecommuting for workers living in pandemic-affected areas, are associated with the improvement of mental health.
In other studies that examined mental health interventions, information interventions such as counseling and preemptive testing were found to have effects on depression and anxiety. In particular, psychosocial interventions, such as cognitive behavior therapy (CBT),26 Instant messenger-based individual consultation,27 and internet-based integrated intervention,28 were found to be significantly associated with a reduction in the prevalence of depression and anxiety. CBT is the most evidence-based psychological intervention in treating various mental disorders, such as depression, anxiety disorders, and substance abuse disorder.26 Patients provided with instant messenger-based individual consultation scored significantly lower in the Hospital Anxiety and Depression Scale (HADS) (HADS-D score before intervention, 10.1 ± 2.8; after intervention, 4.4 ± 2.2, p <0.01; HADS-A score before intervention, 12.6 ± 3.6, after intervention, 6.1 ± 2.1, p < 0.01).27 Previous studies also found that each additional 10 days’ paid leave granted to female workers decreased their OR of depression by 29% (OR, 0.71; 95% CI, 0.55–0.92; p = 0.01),19 and that symptoms of depression decreased (−2.0%)18 in case of telecommuting. After the active intervention of the workplace, the depression OR decreased to 0.76 compared to the pre-intervention group, and the anxiety disorder OR also decreased to 0.73. This may be attributed to company’s efforts to provide transparent information and preemptive screening tests in suspected cases, which contributed considerably to preventing and easing symptoms of depression and anxiety among its employees.
As limitations of this study, the following aspects should be considered: the analysis of indicators to determine depression and anxiety disorders was restricted by excessive information loss due to a large number of workers who did not receive health screening for two consecutive years; the fact that the two major variables “depression” and “anxiety” were measured by self-report questionnaires leaves room for confounding factors; it was not possible to accurately identify those who received paid leave and their residential areas due to the issue of personal information; and the so-called health worker effect could not be ruled out because the participants were only regular workers who were eligible for comprehensive health benefits, including screening.
Despite these limitations, this study is significant for the following merits: it is a single-center study, thus ensuring consistency of the inspectors, testing facilities, and testing methodologies; it is the first study in Korea examining the association between workplace intervention and the prevalence of depression and anxiety; it is a longitudinal study with a large sample (n = 1,978); it is an opportune study in the current situation of a new wave of the COVID-19 pandemic persistently spreading across the globe. From March to August 2020, nine confirmed cases occurred in the company, but depression and anxiety could be reduced through active intervention by the company. The findings of this study allow the assumption that in the event of a similar pandemic situation in the future, active workplace interventions can be a helpful strategy for managing depression and anxiety among workers.
CONCLUSIONS
We found a significant reduction in the levels of perceived depression and anxiety in the workplace that implemented active interventions such as paid leave, telecommuting, and operation of a screening center. Given various factors associated with mental health, workplace interventions alone cannot explain the decrease in depression and anxiety. However, this study provides basic data to improve workers' mental health according to workplace intervention, and further research on intervention within one workplace is needed in the future.
Acknowledgements
The authors would like to thank Jae Chul Ha for technical assistance for this study.
Abbreviations
COVID-19
coronavirus disease 2019
OR
odds ratio
BMI
body mass index
CI
confidence interval
CES-D
The Center for Epidemiologic Studies Depression scale
CUXOS
The Clinically Useful Anxiety Outcome Scale
pre-intervention group
the group that underwent health screenings before the first wave of COVID-19
post-intervention group
the group that underwent health screenings before the first wave of COVID-19
GEE
generalized estimating equations
-
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
-
Competing interests: The authors declare that they have no competing interests.
-
Author Contributions:
Conceptualization: Park HW.
Methodology: Park HW, Park SH.
Software: Park HW, Jung H.
Validation: Park SH.
Formal analysis: Park HO, Park HW.
Investigation: Park HW, Jeong H.
Data curation: Park HW, Chae CH.
Visualization: Park SH.
Writing - original draft: Park HW.
Writing - review & editing: Park HW, Park SH, Kim YW, Son J, Kim CW, Lee JH, Shin YH, Park HO, Chae CH, Chung EY.
NOTES
SUPPLEMENTARY MATERIAL
Supplementary Table 1
Odds ratio for depression and anxiety according to gender
- 1. Holmes EA, O’Connor RC, Perry VH, Tracey I, Wessely S, Arseneault L, et al. Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. Lancet Psychiatry 2020;7(6):547–560. 32304649.ArticlePubMedPMC
- 2. Santomauro DF, Herrera AM, Shadid J, Zheng P, Ashbaugh C, Pigott DM, et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021;398(10312):1700–1712. 34634250.PubMedPMC
- 3. Sharifian-Dorche M, Huot P, Osherov M, Wen D, Saveriano A, Giacomini PS, et al. Neurological complications of coronavirus infection; a comparative review and lessons learned during the COVID-19 pandemic. J Neurol Sci 2020;417:117085. 32871412.ArticlePubMedPMC
- 4. Ma L, Song JN, Song YP, Zhao LT, Chen H. Efficacy and safety of Shufeng Jiedu capsule in the treatment of COVID-19: a protocol for systematic review and meta analysis. Medicine (Baltimore) 2020;99(50):e23293. 33327256.PubMedPMC
- 5. Qian Y, Xu H, Diao J, Li Q, Zhan Q, Fang Y. Influence of life intervention on anxiety, depression, and quality of life of COVID-19 patients: a protocol for systematic review and meta-analysis. Medicine (Baltimore) 2021;100(18):e25391. 33950923.PubMedPMC
- 6. Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet 2020;395(10227):912–920. 32112714.ArticlePubMedPMC
- 7. Gruber J, Prinstein MJ, Clark LA, Rottenberg J, Abramowitz JS, Albano AM, et al. Mental health and clinical psychological science in the time of COVID-19: Challenges, opportunities, and a call to action. Am Psychol 2021;76(3):409–426. 32772538.ArticlePubMedPMC
- 8. Lépine JP, Briley M. The increasing burden of depression. Neuropsychiatr Dis Treat 2011;7(Suppl 1):3–7. 21750622.PubMedPMC
- 9. Bowman D, Scogin F, Lyrene B. The efficacy of self-examination therapy and cognitive bibliotherapy in the treatment of mild to moderate depression. Psychother Res 1995;5(2):131–140.Article
- 10. Proudfoot J, Ryden C, Everitt B, Shapiro DA, Goldberg D, Mann A, et al. Clinical efficacy of computerised cognitive-behavioural therapy for anxiety and depression in primary care: randomised controlled trial. Br J Psychiatry 2004;185(1):46–54. 15231555.ArticlePubMed
- 11. Wright JH, Wright AS, Albano AM, Basco MR, Goldsmith LJ, Raffield T, et al. Computer-assisted cognitive therapy for depression: maintaining efficacy while reducing therapist time. Am J Psychiatry 2005;162(6):1158–1164. 15930065.ArticlePubMed
- 12. Lovell K, Bower P, Richards D, Barkham M, Sibbald B, Roberts C, et al. Developing guided self-help for depression using the Medical Research Council complex interventions framework: a description of the modelling phase and results of an exploratory randomised controlled trial. BMC Psychiatry 2008;8(1):91. 19025646.ArticlePubMedPMCPDF
- 13. Williams C, Wilson P, Walker A, Wallace I, Morrison J, Whitfield G, et al. An evaluation of the Effectiveness of Structured Cognitive Behaviour Therapy Self-Help Materials Delivered by a Self-Help Support Worker Within Primary Care. Report Submitted to the Chief Scientific Officer in Scotland (contract number CZH/4/61). Glasgow, Scotland: University of Glasgow; 2007.
- 14. Parikh SV, Quilty LC, Ravitz P, Rosenbluth M, Pavlova B, Grigoriadis S, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 2. Psychological treatments. Can J Psychiatry 2016;61(9):524–539. 27486150.ArticlePubMedPMCPDF
- 15. Culpepper L. Generalized anxiety disorder in primary care: emerging issues in management and treatment. J Clin Psychiatry 2002;63(Suppl 8):35–42. 12044106.PubMed
- 16. Shields GS, Spahr CM, Slavich GM. Psychosocial interventions and immune system function: a systematic review and meta-analysis of randomized clinical trials. JAMA Psychiatry 2020;77(10):1031–1043. 32492090.ArticlePubMedPMC
- 17. Niileksela CR, Ghosh A, Janis RA. Dynamic changes in generalized anxiety and depression during counseling. J Couns Psychol 2021;68(1):112–124. 32364396.ArticlePubMed
- 18. Oakman J, Kinsman N, Stuckey R, Graham M, Weale V. A rapid review of mental and physical health effects of working at home: how do we optimise health? BMC Public Health 2020;20(1):1825. 33256652.ArticlePubMedPMCPDF
- 19. Kim D. Does paid vacation leave protect against depression among working Americans? A national longitudinal fixed effects analysis. Scand J Work Environ Health 2019;45(1):22–32. 30403822.ArticlePubMedPMC
- 20. Hwang S. Estimation of high-risk drinkers and drinking behavior in Korea-focusing on Korean National Health and Nutrition Examination Survey (KNHANES) and Korean Statistical Information Service data. J Environ Health Sci 2020;46(1):65–77.
- 21. Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas 1977;1(3):385–401.
- 22. Jeon SW, Han C, Ko YH, Yoon S, Pae CU, Choi J, et al. A Korean validation study of the clinically useful anxiety outcome scale: comorbidity and differentiation of anxiety and depressive disorders. PLoS One 2017;12(6):e0179247. 28604808.ArticlePubMedPMC
- 23. Wu S, Zhang K, Parks-Stamm EJ, Hu Z, Ji Y, Cui X. Increases in anxiety and depression during COVID-19: a large longitudinal study from China. Front Psychol 2021;12:706601. 34295294.ArticlePubMedPMC
- 24. Fancourt D, Steptoe A, Bu F. Trajectories of anxiety and depressive symptoms during enforced isolation due to COVID-19 in England: a longitudinal observational study. Lancet Psychiatry 2021;8(2):141–149. 33308420.ArticlePubMed
- 25. Waterman S, Hunter EC, Cole CL, Evans LJ, Greenberg N, Rubin GJ, et al. Training peers to treat Ebola centre workers with anxiety and depression in Sierra Leone. Int J Soc Psychiatry 2018;64(2):156–165. 29432085.ArticlePubMedPDF
- 26. David D, Cristea I, Hofmann SG. Why cognitive behavioral therapy is the current gold standard of psychotherapy. Front Psychiatry 2018;9:4. 29434552.ArticlePubMedPMC
- 27. Zhou L, Xie RH, Yang X, Zhang S, Li D, Zhang Y, et al. Feasibility and preliminary results of effectiveness of social media-based intervention on the psychological well-being of suspected COVID-19 cases during quarantine. Can J Psychiatry 2020;65(10):736–738. 32483978.ArticlePubMedPMCPDF
- 28. Schröder J, Berger T, Westermann S, Klein JP, Moritz S. Internet interventions for depression: new developments. Dialogues Clin Neurosci 2016;18(2):203–212. 27489460.ArticlePubMedPMC
REFERENCES
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Effects of resilience training for mothers on maternal resilience and children’s pain in pediatric burn units in a randomized controlled trial
Fahimeh Alsadat Hosseini, Maryam Shaygan, Maryam Shayegan
Scientific Reports.2025;[Epub] CrossRef - Telecommuting-related health outcomes during the COVID-19 pandemic in South Korea: a national population-based cross-sectional study
Seung-Woo Ryoo, Jin-Young Min, Dong-Wook Lee, Baek-Yong Choi, Juho Choi, Ho-Yeon Kim, Kyoung-Bok Min
BMC Public Health.2023;[Epub] CrossRef - Multidimensional typologies of precarious employment and their relationships with mental well-being in Korean wageworkers: A latent class analysis based on the Korean Working Conditions Survey (2020–2021)
Seong-Uk Baek, Jong-Uk Won, Jin-Ha Yoon
Preventive Medicine.2023; 177: 107787. CrossRef
 Cite
CiteAssociation between coronavirus disease 2019-related workplace interventions and prevalence of depression and anxiety
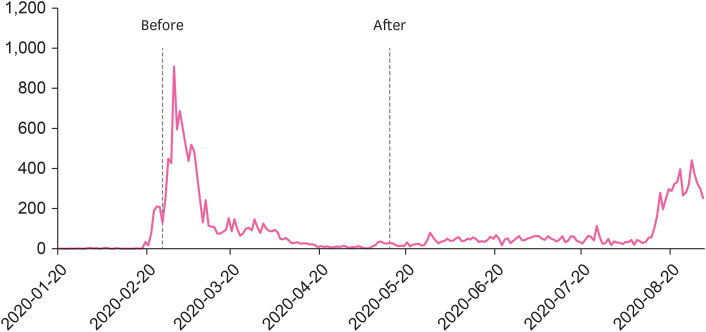
Fig. 1 Daily number of new confirmed cases of coronavirus disease 2019.
Fig. 1
Association between coronavirus disease 2019-related workplace interventions and prevalence of depression and anxiety
| Variables | Mean ± SD or percentage (%) | |||
|---|---|---|---|---|
| Pre-intervention (n = 2,278) | Post-intervention (n = 1,678) | |||
| Age (years) | 34.78 ± 7.83 | 33.97 ± 7.29 | < 0.001 | |
| Depression | 384 (16.86) | 247 (14.72) | 0.070 | |
| Anxiety | 507 (22.26) | 309 (18.41) | 0.003 | |
| Gender | < 0.001 | |||
| Male | 1,160 (50.92) | 696 (41.48) | ||
| Female | 1,118 (49.08) | 982 (58.52) | ||
| BMI over 25 | 728 (31.96) | 580 (34.56) | 0.085 | |
| Hypertension | 120 (5.27) | 56 (3.34) | 0.004 | |
| Diabetes | 67 (2.94) | 47 (2.80) | 0.794 | |
| Dyslipidemia | 247 (15.12) | 231 (16.89) | 0.187 | |
| Risk drinkinga | 783 (34.37) | 610 (36.35) | 0.197 | |
| Smoking status | 0.004 | |||
| Nob | 1,499 (65.80) | 1,188 (70.80) | ||
| Former | 357 (15.67) | 222 (13.23) | ||
| Current | 422 (18.53) | 268 (15.97) | ||
| Physical activity | 928 (40.74) | 723 (43.09) | 0.139 | |
| Variables | Crude OR | Adjusted OR | |||
|---|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | ||||
| Depression | |||||
| Pre-intervention | Ref. | Ref. | |||
| Post-intervention | 0.79 (0.69–0.90) | 0.001 | 0.76 (0.66–0.87) | < 0.001 | |
| Anxiety | |||||
| Pre-intervention | Ref. | Ref. | |||
| Post-intervention | 0.77 (0.69–0.86) | < 0.001 | 0.73 (0.65–0.82) | < 0.001 | |
Table 1 General characteristics of all study participants (n = 1,978)
Data are shown as mean ± standard deviation or number (%).
BMI: body mass index.
aRisk drinking: an average alcohol consumption of ≥ 7 cups (Alchhol content 8 g/cup), ≥ 2 times per week; bSmoking status: No = Lifetime smoking history ≤ 5 packs.
Table 2 OR for depression and anxiety according to company intervention
Adjusted model: adjusted for age, sex, obesity, hypertension, diabetes mellitus, risk drinking, smoking, physical activity.
Pre-intervention: pre-intervention group (for those who underwent health screening from January 2019 to February 2020); Post-intervention: post-intervention group (for those who underwent health screening from March 2020 to August 2020); OR: odds ratio; CI: confidence interval.

