
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 33; 2021 > Article
- Original Article A pilot study to assess a risk of a high-risk group of low back pain membership in workers who perform the manual material handling tasks
-
Sungho Lee
 , Seongchan Heo, Jong-Young Lee
, Seongchan Heo, Jong-Young Lee -
Annals of Occupational and Environmental Medicine 2021;33:e34.
DOI: https://doi.org/10.35371/aoem.2021.33.e34
Published online: November 17, 2021
Department of Occupational and Environmental Medicine, Dongguk University Gyeongju Hospital, Gyeongju, Korea.
- Correspondence: Jong-Young Lee. Department of Occupational and Environmental Medicine, Dongguk University Gyeongju Hospital, 87 Dongdae-ro, Gyeongju 38067, Korea. leejy1956@hotmail.com
• Received: September 13, 2021 • Accepted: November 3, 2021
Copyright © 2021 Korean Society of Occupational & Environmental Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background We conducted this experimental study to estimate a risk of a high-risk group of low back pain (LBP) membership in workers who perform the manual material handling (MMH) tasks in an actual workplace setting.
-
Methods The subjects include healthy workers who were engaged in 12 MMH tasks at 6 manufacturing companies. We assessed the dynamic motion of trunk or lumbar spine using an industrial lumbar motion monitor (BioDynamics Laboratory of Ohio State University). The subjects were evaluated for the age, gender, years of working and anthropometric measurements (e.g., height, weight, shoulder height, elbow height, iliac height, leg length, trunk length, trunk circumference, iliac width, iliac depth, xiphoid width and xiphoid depth). Moreover, they were also evaluated for a risk of a high-risk group of LBP membership based on lift frequency, average twisting velocity, maximum moment, maximum sagittal flexion and maximum lateral velocity.
-
Results The subjects who were engaged in a packaging at a detergent manufacturing company are at the greatest risk of LBP (63.76%). This was followed by packaging at a leather product manufacturing company (57.06%), packaging at a non-metallic casting material manufacturing company (57.03%), manual injection at a non-metallic casting material manufacturing company (52.00%), toggling at a leather product manufacturing company (46.09%), non-metallic casting material manufacturing company (42.88%), rolling at a non-metallic mineral product manufacturing company (42.12%), shooting at a non-metallic casting material manufacturing company (40.99%), vacuum processes at a leather product manufacturing company (35.00%), looping at a general industrial machinery manufacturing company (33.93%), setting at a leather product manufacturing company (30.22%) and packaging at a general metal product manufacturing company (22.02%).
-
Conclusions Our approach indicates that there is a risk of a high-risk group of LBP membership in workers who perform the MMH tasks.
BACKGROUND
Low back pain (LBP) is such a common problem as to affect ≥ 25% of total adult workers.1 Its symptoms may be worsened by physical demands of the work.2 Nevertheless, both work- and non-work-related episodes of LBP may also cause work absences. This may lead to problems that workers can perform normal job tasks.3 LBP in a workplace should be considered medically serious; it may cause occupational challenges and disruption because it is self-limiting in nature.4
Workers may be vulnerable to both acute and chronic episodes (> 6 months) of LBP irrespective of whether they are men or women.5 Workers presenting with primary chronic LBP should be meticulously examined, followed by appropriate treatments, employer coordination or occupational rehabilitation.6,7
Workers across all industries and occupations may be vulnerable to LBP, but physical demands of the work raise a risk of developing it.8 From this context, unnatural body positions, a sudden change in the task, fatigue, heavy lifting, outdoor work, hand movements and frequent bending and twisting may serve as risk factors of LBP.9,10,11 Moreover, psychological demands of the work, such as low supervisor support, stressful monotonous work, a rapidly paced work environment, job insecurity, work-family imbalance and exposure to hostile work, may also serve as risk factors of LBP.9,10,11
In 1990, Straker12 defined the manual material handling (MMH) as any activities that are in need of force generated by a person to lift, lower, push, pull, carry or otherwise move, hold or restrain a person, animal or thing. Moreover, the Occupational Safety and Health Administration defined the MMH as the act of moving materials by hand to lift, lower, push, pull and carry them.13 According to a systematic review of the previous studies conducted by Kuiper et al.,14 of various MMH tasks, lifting and lowering are the most frequently involved in diverse occupations and pose a major risk to workers' health status. The MMH tasks are commonly seen in blue collar jobs, such as manufacturing, building and construction, mechanical work, maintenance, repair or technical installations.15 Moreover, they are also seen in healthcare professionals, such as nurses, surgeons, dentists and physiotherapists.16 All the workers mentioned herein are vulnerable to LBP.17 According to a survey conducted by Ferguson et al.18 in MMH workers, a 1-year prevalence of LBP for those whose symptoms last for ≥ 7 days, those requiring medical treatments and those requiring a leave from work was 25%, 14% and 10%, respectively.
Given the above background, we conducted this experimental study to estimate a risk of a high-risk group of LBP membership in workers who perform the MMH tasks in an actual workplace setting.
METHODS
The current study was conducted in healthy workers who were engaged in 12 MMH tasks at 6 manufacturing companies. We included normal healthy men or women who were engaged in MMH tasks at 6 manufacturing companies, the subjects who could be assessed for the dynamic motion and postures of the trunk or lumbar spine and heavy object handling processes and those who could be assessed for the type and details of MMH tasks and anthropometric characteristics. But we excluded the subjects who had an inability to comply with the study protocol.
The current study was conducted in compliance with the relevant ethics guidelines following the approval by the Institutional Review Board (IRB) of Dongguk University Gyeongju Hospital (IRB No.110757-202109-HR-02-02). All procedures described herein were performed in accordance with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The subjects submitted a written informed consent for study participation.
We assessed the dynamic motion of trunk or lumbar spine using an industrial lumbar motion monitor (LMM; BioDynamics Laboratory of Ohio State University, Columbus, OH, USA), as previously described.19,20
The LMM was designed to document 3-dimensional (3D) components of the trunk motion in the work environment. It was modeled after the trunk motion control system of the back. That is, the spine is guided by the spinous and transverse processes that form a T-section in the posterior aspects of each spinal vertebra. T-sections are connected to each other with ligaments and muscles that envelop the facet joints of the spinal segments. The LMM is an exoskeleton of the spine that replicates the motion of these T-sections in the lumbar spine. Thus, T-sections of the LMM are intended to simulate the motion of the facet joints. The LMM is worn on the back of the worker and moves along with the worker. Each edge of the T-section is connected to 3 potentiometers on the base of the LMM via wires. The wires differentially change the voltage readings in the potentiometers as the LMM moves forwards, backwards or to the sides. A cable is also placed through the junction in each T-section and then connected to a fourth potentiometer that changes as the LMM is twisted. Thus, the LMM measures the difference in spine position of the lumbar spine (as a unit) relative to the pelvis.21
The potentiometer signals are interfaced with an analog-to-digital converter and the signals are recorded on a microcomputer. The signals have been calibrated to correlate with trunk angle. The signals are then processed to determine the position, velocity and acceleration of the trunk as a function of time.21
To quantify the magnitude of angle, the angular velocity and acceleration, the duration of exposure to the risk of developing LBP depending on the direction of lumbar motion and the degree of such risk based on a model for estimating it, we analyzed the LMM data. We also analyzed the LMM data relative to the level of risk of developing LBP, thus attempting to determine whether the subjects could perform an excessive motion of the trunk or lumbar spine in an actual workplace setting; these include lifting strength ratio, average twisting velocity, maximum moment, maximum sagittal flexion and maximum lateral velocity.22
A risk of a high-risk group of LBP membership was calculated using a low-back disorder risk assessment model, as previously described by Marras et al.22,23,24
The subjects were evaluated for the age, gender, years of working and anthropometric measurements (e.g., height, weight, shoulder height, elbow height, iliac height [left and right], leg length [upper and lower], trunk length, trunk circumference, iliac width, iliac depth, xiphoid width and xiphoid depth). Moreover, they were also evaluated for a risk of a high-risk group of LBP membership based on lift frequency, average twisting velocity, maximum moment, maximum sagittal flexion and maximum lateral velocity, whose definitions have been described elsewhere.25,26
All data was expressed as mean ± standard deviation or the number of the subjects with percentage, where appropriate.
RESULTS
The current study enrolled a total of 25 subjects (n = 25), comprising 13 men (52.00%) and 12 women (48.00%), whose mean age was 48.80 ± 5.05 years old. Moreover, they were engaged in their work during a mean period of 12.40 ± 4.54 years. Furthermore, their anthropometric measurements were also measured and then averaged; these include height (167.86 ± 6.12 cm), weight (68.34 ± 7.16 kg), shoulder height (134.60 ± 5.50 cm), elbow height (100.95 ± 3.46 cm), Iliac height (left: 88.87 ± 3.48 cm and right: 87.91 ± 4.06 cm), leg length (upper: 37.13 ± 4.24 cm and lower: 47.27 ± 2.98 cm), trunk length (54.66 ± 6.75 cm), trunk circumference (81.71 ± 3.61 cm), iliac width (29.80 ± 2.79 cm), iliac depth (19.10 ± 2.85 cm), xiphoid width (33.34 ± 2.66 cm) and xiphoid depth (21.52 ± 2.02 cm). Baseline characteristics of the subjects are represented in Table 1.
Table 1
Baseline characteristics of the subjects (n = 25)
As shown in Fig. 1A-E, lift frequency was the highest (97.99) in workers who were involved in packaging in the detergent manufacturing industry; average twisting velocity was the highest (52.54) in those who were involved in setting in the leather product manufacturing industry; maximum moment was the highest (98.10) in those who were involved in packaging in the detergent manufacturing industry; maximum sagittal flexion was the highest (71.85) in those who were involved in packaging in the leather product manufacturing industry; and maximum lateral velocity was the highest (52.81) in workers who were involved in packaging in the detergent manufacturing industry.
Fig. 1
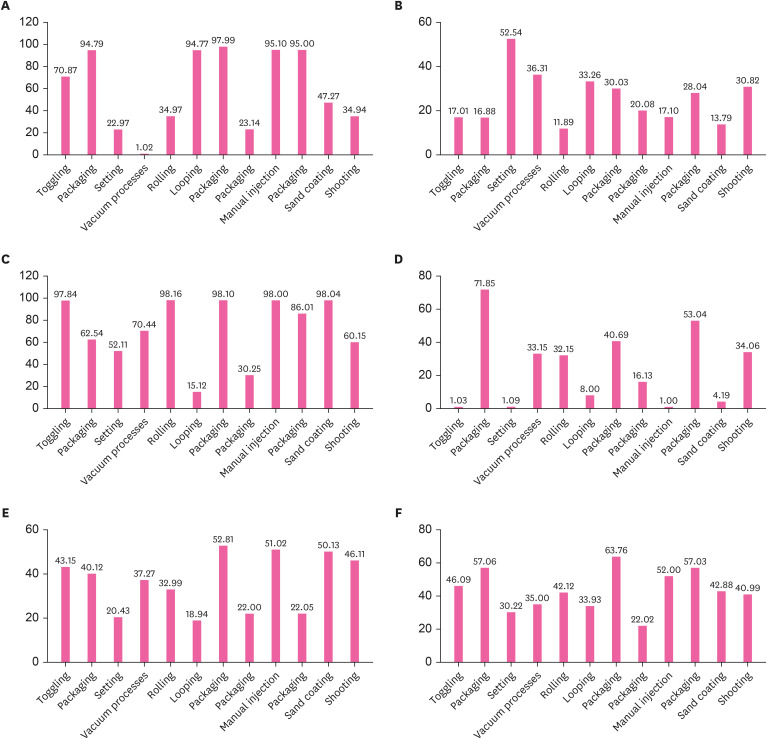
Estimation of a risk of a high-risk group of LBP membership. (A) Lift frequency was the highest (97.99) in workers who were involved in packaging in the detergent manufacturing industry; (B) average twisting velocity was the highest (52.54) in those who were involved in setting in the leather product manufacturing industry; (C) maximum moment was the highest (98.10) in those who were involved in packaging in the detergent manufacturing industry; (D) maximum sagittal flexion was the highest (71.85) in those who were involved in packaging in the leather product manufacturing industry; and (E) maximum lateral velocity was the highest (52.81) in workers who were involved in packaging in the detergent manufacturing industry. (F) The subjects who were engaged in a packaging at a detergent manufacturing company are at the greatest risk of LBP (63.76%).
LBP: low back pain.
As shown in Fig. 1F, the subjects who were engaged in a packaging at a detergent manufacturing company are at the greatest risk of LBP (63.76%). This was followed by packaging at a leather product manufacturing company (57.06%), packaging at a non-metallic casting material manufacturing company (57.03%), manual injection at a non-metallic casting material manufacturing company (52.00%), toggling at a leather product manufacturing company (46.09%), non-metallic casting material manufacturing company (42.88%), rolling at a non-metallic mineral product manufacturing company (42.12%), shooting at a non-metallic casting material manufacturing company (40.99%), vacuum processes at a leather product manufacturing company (35.00%), looping at a general industrial machinery manufacturing company (33.93%), setting at a leather product manufacturing company (30.22%) and packaging at a general metal product manufacturing company (22.02%).
DISCUSSION
With the technological advancements in the modern industry, human life has become convenient.27 It is characterized by frequent use of machines for moving materials, although MMH tasks are still performed by workers.28 This may cause serious problems to workers. The MMH tasks are performed in a limited space, where workers' activity is highly dependent on their physical strength.29 In this regard, the ergonomic MMH tasks are justified. Otherwise, workers may be vulnerable to industrial accident involving damages to their body.30
It is worthwhile to incorporate ergonomic principles into the industrial work environment, which is essential for controlling the occurrence of musculoskeletal injuries (e.g., LBP). Positive effects of ergonomic interventions based on risk assessment tools and techniques have been well described in the literature.31,32 Such interventions include lowering the prevalence and cost of injuries, reducing discomfort and fatigue and improving the productivity. But there are also contradictory reports that ergonomic interventions are not beneficial strategies in the context of work-related musculoskeletal disorders.33,34 It would therefore be mandatory to assess a risk of a high-risk group of LBP membership in workers who perform the MMH tasks.
To date, several tools for risk assessment for LBP have been described in the literature.35,36 They are based on the possible mechanisms underlying the onset of LBP in a workplace setting. Marras et al.36 assesed jobs using both the 1981 and 1991 National Institute for Occupational Safety & Health (NIOSH) lifting indices as compared with psychophysical limits. Moreover, Waters et al.37 assessed the feasibility of these tools, a 3D Static Strength Prediction Program, a program to predict the energy expenditure, and the use of heart rate and oxygen consumption. Furthermore, Lavender et al.38 reported that there would be no need to measure the same dimensions of the risk of LBP following a comparison of tools for assessment of the risk of it. It would therefore be mandatory to validate tools for assessment of the risk of LBP in a workplace setting. This should be accompanied by the optimization of the design of the workplace.
The importance of the feasibility of tools for assessment of the risk of LBP deserves special attention. There is no time to achieve make ergonomic improvements through trial and error in the current competitive market. This is not only because valuable resources are wasted on ineffective tools but also because the onset of LBP cannot be controlled in a timely manner. Consequently, the number of workers presenting with symptoms of LBP as well as the cost of damage would be increased and a loss of competitiveness would be hard to avoid. It is therefore imperative that effective tools for assessment of the risk of LBP in association with the design of a workplace, which will be essential for responding to a question regarding to the degree of the exposure of a workplace to such risk. From this context, an ergonomic model for assessing the risk of LBP has been developed using the LMM data and it has applied to diverse types of the MMH tasks.22,24,39,40 Based on these previous published studies, we estimated a risk of a high-risk group of LBP membership in workers who perform the MMH tasks in an actual workplace setting.
Despite rigorous examination and appropriate management, there may be a variability in an ability to stay at work or return to work in workers with LBP.3,41 Moreover, there is often discrepancy between workers' functional capacity and workability and their return-to-work outcomes.42,43 Presumably, this might be because compound factors are involved in functional and occupational outcomes of workers with LBP; these include pain beliefs, healthcare systems, workplace support and accommodation and socio-demographics.44 It can therefore be inferred that characteristics of a worker, system and a workplace rather than the severity of LBP are determinants of the level of workability.
The onset or worsening of LBP can be prevented by decreasing high physical demands, avoiding unnatural body positions, educating workers for safe MMH tasks and re-engineering workstations and assembly lines.45,46 This was well illustrated in a significant decrease in the occurrence of work-related LBP.46 According to randomized clinical trials, however, some recommendations for the prevention of LBP, such as use of a back belt, were found to be ineffective.47,48 Therefore, workers with LBP should be given reasonable accommodation and support. Then, the relevant regulations and policies should be implemented to prevent long-term work disability, unemployment or unnecessary departures from the workforce.
Our results cannot be generalized not only because we evaluated only a small number of the subjects but also because we failed to serve a control group in predicting a risk of a high-risk group of LBP membership. This deserves further controlled studies to assess the feasibility of our approach. Moreover, limitations of the current study are that we failed to assess the feasibility of an industrial LMM as compared with other assessment tools. For MMH tasks, Lavender et al.38 reported that if properly used, currently-available assessment tools would be helpful for improving effects of ergonomic interventions in lowering or predicting a risk of work-related musculoskeletal disorders, including LBP. Such tools include the 1991 NIOSH lifting equation (NLE; NIOSH, Washington, D.C., USA), the University of Michigan 3D Static Strength Prediction Program (3D SSPP; University of Michigan, Ann Arbor, MI, USA), and the LMM. An appropriate use of such quantitative assessment tools is a more time-sensitive method for efficiently reducing the level of work-related biomechanical stress that may arise from ergonomics interventions.49 Further prospective controlled studies are therefore warranted to propose a model for predicting a risk of a high-risk group of LBD membership in workers who are involved in MMH tasks.
CONCLUSIONS
In conclusion, our approach indicates that there is a risk of a high-risk group of LBP membership in workers who perform the MMH tasks. But further prospective, randomized controlled studies are warranted to validate our approach.
Abbreviations
LBP
low back pain
LMM
lumbar motion monitor
MMH
manual material handling
NIOSH
National Institute for Occupational Safety & Health
3D
3-dimensional
-
Competing interests: The authors declare that they have no competing interests.
-
Author contributions:
NOTES
- 1. Luckhaupt SE, Dahlhamer JM, Gonzales GT, Lu ML, Groenewold M, Sweeney MH, et al. Prevalence, recognition of work-relatedness, and effect on work of low back pain among U.S. workers. Ann Intern Med 2019;171(4):301–304. 31083729.ArticlePubMedPMCPDF
- 2. Nygaard PP, Skovlund SV, Sundstrup E, Andersen LL. Is low-back pain a limiting factor for senior workers with high physical work demands? A cross-sectional study. BMC Musculoskelet Disord 2020;21(1):622. 32958013.ArticlePubMedPMCPDF
- 3. Wynne-Jones G, Cowen J, Jordan JL, Uthman O, Main CJ, Glozier N, et al. Absence from work and return to work in people with back pain: a systematic review and meta-analysis. Occup Environ Med 2014;71(6):448–456. 24186944.ArticlePubMedPMC
- 4. Kerr MS, Frank JW, Shannon HS, Norman RW, Wells RP, Neumann WP, et al. Biomechanical and psychosocial risk factors for low back pain at work. Am J Public Health 2001;91(7):1069–1075. 11441733.ArticlePubMedPMC
- 5. Stevans JM, Delitto A, Khoja SS, Patterson CG, Smith CN, Schneider MJ, et al. Risk factors associated with transition from acute to chronic low back pain in US patients seeking primary care. JAMA Netw Open 2021;4(2):e2037371. 33591367.ArticlePubMedPMC
- 6. Paquette S. Return to work with chronic low back pain: using an evidence-based approach along with the occupational therapy framework. Work 2008;31(1):63–71. 18820421.ArticlePubMedPDF
- 7. Johanning E. Evaluation and management of occupational low back disorders. Am J Ind Med 2000;37(1):94–111. 10573599.ArticlePubMed
- 8. Kim JY, Shin JS, Lim MS, Choi HG, Kim SK, Kang HT, et al. Relationship between simultaneous exposure to ergonomic risk factors and work-related lower back pain: a cross-sectional study based on the fourth Korean working conditions survey. Ann Occup Environ Med 2018;30(1):58. 30202532.ArticlePubMedPMCPDF
- 9. Dick RB, Lowe BD, Lu ML, Krieg EF. Trends in work-related musculoskeletal disorders from the 2002 to 2014 general social survey, quality of work life supplement. J Occup Environ Med 2020;62(8):595–610. 32404838.ArticlePubMedPMC
- 10. Steffens D, Ferreira ML, Latimer J, Ferreira PH, Koes BW, Blyth F, et al. What triggers an episode of acute low back pain? A case-crossover study. Arthritis Care Res (Hoboken) 2015;67(3):403–410. 25665074.ArticlePubMed
- 11. Yang H, Haldeman S, Lu ML, Baker D. Low back pain prevalence and related workplace psychosocial risk factors: a study using data from the 2010 National Health Interview Survey. J Manipulative Physiol Ther 2016;39(7):459–472. 27568831.ArticlePubMedPMC
- 12. Straker LM. An overview of manual handling injury statistics in Western Australia. Int J Ind Ergon 1999;24(4):357–364.Article
- 13. Albers J, Estill C, MacDonald L. Identification of ergonomics interventions used to reduce musculoskeletal loading for building installation tasks. Appl Ergon 2005;36(4):427–439. 15892937.ArticlePubMed
- 14. Kuiper JI, Burdorf A, Verbeek JH, Frings-Dresen MH, van der Beek AJ, Viikari-Juntura ER. Epidemiologic evidence on manual materials handling as a risk factor for back disorders: a systematic review. Int J Ind Ergon 1999;24(4):389–404.Article
- 15. Schneider SP. Musculoskeletal injuries in construction: a review of the literature. Appl Occup Environ Hyg 2001;16(11):1056–1064. 11757902.ArticlePubMed
- 16. Warming S, Precht DH, Suadicani P, Ebbehøj NE. Musculoskeletal complaints among nurses related to patient handling tasks and psychosocial factors--based on logbook registrations. Appl Ergon 2009;40(4):569–576. 18789431.ArticlePubMed
- 17. Graham L, Gray H. Recently qualified physiotherapists' perceptions of work-related musculoskeletal disorders. Int J Ther Rehabil 2005;12(7):299–307.Article
- 18. Ferguson SA, Merryweather A, Thiese MS, Hegmann KT, Lu ML, Kapellusch JM, et al. Prevalence of low back pain, seeking medical care, and lost time due to low back pain among manual material handling workers in the United States. BMC Musculoskelet Disord 2019;20(1):243. 31118009.ArticlePubMedPMCPDF
- 19. Ferguson SA, Marras WS. Revised protocol for the kinematic assessment of impairment. Spine J 2004;4(2):163–169. 15016393.ArticlePubMed
- 20. Ferguson SA, Marras WS, Burr DL, Woods S, Mendel E, Gupta P. Quantification of a meaningful change in low back functional impairment. Spine 2009;34(19):2060–2065. 19730214.ArticlePubMed
- 21. Marras WS, Fathallah FA, Miller RJ, Davis SW, Mirka GA. Accuracy of a three-dimensional lumbar motion monitor for recording dynamic trunk motion characteristics. Int J Ind Ergon 1992;9(1):75–87.Article
- 22. Marras WS, Lavender SA, Leurgans SE, Rajulu SL, Allread WG, Fathallah FA, et al. The role of dynamic three-dimensional trunk motion in occupationally-related low back disorders. The effects of workplace factors, trunk position, and trunk motion characteristics on risk of injury. Spine 1993;18(5):617–628. 8484154.ArticlePubMed
- 23. Marras WS, Allread WG, Burr DL, Fathallah FA. Prospective validation of a low-back disorder risk model and assessment of ergonomic interventions associated with manual materials handling tasks. Ergonomics 2000;43(11):1866–1886. 11105977.ArticlePubMed
- 24. Marras WS, Lavender SA, Leurgans SE, Fathallah FA, Ferguson SA, Allread WG, et al. Biomechanical risk factors for occupationally related low back disorders. Ergonomics 1995;38(2):377–410. 7895740.ArticlePubMed
- 25. Marras WS, Parakkat J, Chany AM, Yang G, Burr D, Lavender SA. Spine loading as a function of lift frequency, exposure duration, and work experience. Clin Biomech (Bristol, Avon) 2006;21(4):345–352.ArticlePubMed
- 26. Iqbal R, De A, Mishra W, Maulik S, Chandra AM. Study on lumbar kinematics and the risk of low back disorder in female university students by using shoes of different heel heights. Work 2012;41(Suppl 1):2521–2526. 22317099.ArticlePubMedPDF
- 27. Chau KY, Lam MH, Cheung ML, Tso EK, Flint SW, Broom DR, et al. Smart technology for healthcare: exploring the antecedents of adoption intention of healthcare wearable technology. Health Psychol Rev 2019;7(1):8099.ArticlePubMedPMCPDF
- 28. Dempsey PG, Burdorf A, Webster BS. The influence of personal variables on work-related low-back disorders and implications for future research. J Occup Environ Med 1997;39(8):748–759. 9273879.ArticlePubMed
- 29. de Cássia Pereira Fernandes R, Pataro SM, de Carvalho RB, Burdorf A. The concurrence of musculoskeletal pain and associated work-related factors: a cross sectional study. BMC Public Health 2016;16(1):628. 27449935.PubMedPMC
- 30. Saha A, Nag A, Nag PK. Occupational injury proneness in Indian women: a survey in fish processing industries. J Occup Med Toxicol 2006;1(1):23. 16968532.ArticlePubMedPMC
- 31. Garg A, Owen B. Reducing back stress to nursing personnel: an ergonomic intervention in a nursing home. Ergonomics 1992;35(11):1353–1375. 1425566.ArticlePubMed
- 32. Aarås A. The impact of ergonomic intervention on individual health and corporate prosperity in a telecommunications environment. Ergonomics 1994;37(10):1679–1696. 7957020.ArticlePubMed
- 33. Bigos SJ, Battié MC, Spengler DM, Fisher LD, Fordyce WE, Hansson TH, et al. A prospective study of work perceptions and psychosocial factors affecting the report of back injury. Spine 1991;16(1):1–6. 1825891.ArticlePubMed
- 34. Hadler NM. Back pain in the workplace. What you lift or how you lift matters far less than whether you lift or when. Spine 1997;22(9):935–940. 9152441.ArticlePubMed
- 35. Waters TR, Putz-Anderson V, Garg A, Fine LJ. Revised NIOSH equation for the design and evaluation of manual lifting tasks. Ergonomics 1993;36(7):749–776. 8339717.ArticlePubMed
- 36. Marras WS, Fine LJ, Ferguson SA, Waters TR. The effectiveness of commonly used lifting assessment methods to identify industrial jobs associated with elevated risk of low-back disorders. Ergonomics 1999;42(1):229–245. 9973881.ArticlePubMed
- 37. Waters TR, Putz-Anderson V, Baron S. Methods for assessing the physical demands of manual lifting: a review and case study from warehousing. Am Ind Hyg Assoc J 1998;59(12):871–881. 9866167.ArticlePubMed
- 38. Lavender SA, Oleske DM, Nicholson L, Andersson GB, Hahn J. Comparison of five methods used to determine low back disorder risk in a manufacturing environment. Spine 1999;24(14):1441–1448. 10423789.ArticlePubMed
- 39. Portell M, Sene-Mir AM, Anguera MT, Jonsson GK, Losada JL. Support system for the assessment and intervention during the manual material handling training at the workplace: contributions from the systematic observation. Front Psychol 2019;10:1247. 31231277.ArticlePubMedPMC
- 40. Marras WS, Kim JY. Anthropometry of industrial populations. Ergonomics 1993;36(4):371–378.Article
- 41. Haldorsen EM, Indahl A, Ursin H. Patients with low back pain not returning to work. A 12-month follow-up study. Spine 1998;23(11):1202–1207. 9636972.ArticlePubMed
- 42. Gross DP, Battié MC. Functional capacity evaluation performance does not predict sustained return to work in claimants with chronic back pain. J Occup Rehabil 2005;15(3):285–294. 16119221.ArticlePubMedPDF
- 43. Gross DP, Asante AK, Miciak M, Battié MC, Carroll LJ, Sun A, et al. Are performance-based functional assessments superior to semistructured interviews for enhancing return-to-work outcomes? Arch Phys Med Rehabil 2014;95(5):807–815.e1. 24502839.ArticlePubMed
- 44. Kristman VL, Shaw WS, Boot CR, Delclos GL, Sullivan MJ, Ehrhart MG, et al. Researching complex and multi-level workplace factors affecting disability and prolonged sickness absence. J Occup Rehabil 2016;26(4):399–416. 27550629.ArticlePubMedPMCPDF
- 45. Schaafsma FG, Anema JR, van der Beek AJ. Back pain: Prevention and management in the workplace. Best Pract Res Clin Rheumatol 2015;29(3):483–494. 26612243.ArticlePubMed
- 46. da Silva T, Mills K, Brown BT, Pocovi N, de Campos T, Maher C, et al. Recurrence of low back pain is common: a prospective inception cohort study. J Physiother 2019;65(3):159–165. 31208917.ArticlePubMed
- 47. Sowah D, Boyko R, Antle D, Miller L, Zakhary M, Straube S. Occupational interventions for the prevention of back pain: Overview of systematic reviews. J Safety Res 2018;66:39–59. 30121110.ArticlePubMed
- 48. Verbeek JH, Martimo KP, Karppinen J, Kuijer PP, Viikari-Juntura E, Takala EP. Manual material handling advice and assistive devices for preventing and treating back pain in workers. Cochrane Database Syst Rev 2011;(6):CD005958. 21678349.ArticlePubMed
- 49. Marklin RW, Wilzbacher JR. Four assessment tools of ergonomics interventions: case study at an electric utility's warehouse system. Am Ind Hyg Assoc J 1999;60(6):777–784. 10635543.ArticlePubMed
REFERENCES
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Effect of training on knowledge, behaviors, and low back pain among marble workers: non-randomized experimental study
Gülcihan Aybike Dilek Kart, Ayse Meydanlioglu
Frontiers in Public Health.2026;[Epub] CrossRef - Assessment of work-related musculoskeletal lower back pain for dentists in Kuwait
Khaled Alkhaledi
Journal of Engineering Research.2025; 13(4): 3563. CrossRef - ERGONOMİK RİSK DEĞERLENDİRME YÖNTEMLERİYLE TESPİT EDİLMİŞ FİZİKSEL İŞ YÜKÜ İLE ENERJİ TÜKETİMİNİN DEĞERLENDİRİLMESİ
Emin Kahya, Ceyda Özgen, Nasiba Jorayeva
Eskişehir Osmangazi Üniversitesi Mühendislik ve Mimarlık Fakültesi Dergisi.2024; 32(2): 1315. CrossRef - Investigation general and specific methods of assessing ergonomic risk factors related to musculoskeletal disorders - a systematic review
Bahram Kouhnavard, Mojtaba Khosravi Danesh, Adel Mazloumi, Mansour Shamsipour
Occupational Health Journal.2024; 20(2): 253. CrossRef - Research misconduct using a ghostwriter in a paper-writing company
Kyunghee Jung-Choi
Annals of Occupational and Environmental Medicine.2023;[Epub] CrossRef - Manual Handling as Contributor of Low Back Pain for Workers: A Case Study at PT Sumber Mandiri Jaya, Kabupaten Merauke
Boyke Elyas Michael Sambeko, Nugroho Susanto, Azir Alfanan
The Indonesian Journal of Occupational Safety and Health.2023; 13(1): 29. CrossRef
 Cite
CiteA pilot study to assess a risk of a high-risk group of low back pain membership in workers who perform the manual material handling tasks
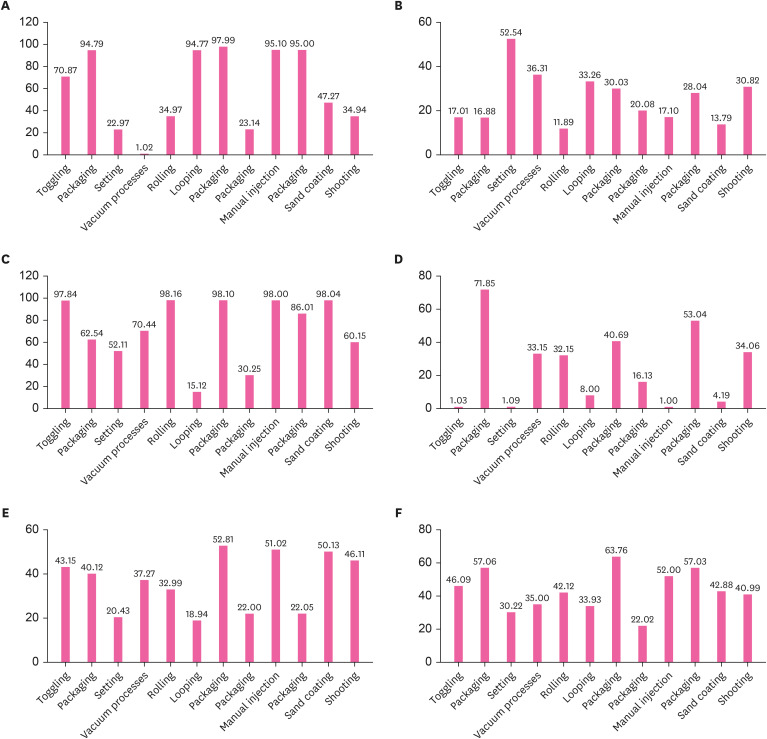
Fig. 1 Estimation of a risk of a high-risk group of LBP membership. (A) Lift frequency was the highest (97.99) in workers who were involved in packaging in the detergent manufacturing industry; (B) average twisting velocity was the highest (52.54) in those who were involved in setting in the leather product manufacturing industry; (C) maximum moment was the highest (98.10) in those who were involved in packaging in the detergent manufacturing industry; (D) maximum sagittal flexion was the highest (71.85) in those who were involved in packaging in the leather product manufacturing industry; and (E) maximum lateral velocity was the highest (52.81) in workers who were involved in packaging in the detergent manufacturing industry. (F) The subjects who were engaged in a packaging at a detergent manufacturing company are at the greatest risk of LBP (63.76%).LBP: low back pain.
Fig. 1
A pilot study to assess a risk of a high-risk group of low back pain membership in workers who perform the manual material handling tasks
| Variables | Values | ||
|---|---|---|---|
| Age (years old) | 48.80 ± 5.05 | ||
| Gender | |||
| Men | 13 (52.00) | ||
| Women | 12 (48.00) | ||
| Type of MMH tasks | |||
| Leather product manufacturing | |||
| Toggling | 1 (4.00) | ||
| Packaging | 1 (4.00) | ||
| Setting | 1 (4.00) | ||
| Vacuum processes | 1 (4.00) | ||
| Non-metallic mineral product manufacturing | |||
| Rolling | 4 (16.00) | ||
| General industrial machinery manufacturing | |||
| Looping | 5 (20.00) | ||
| Detergent manufacturing | |||
| Packaging | 4 (16.00) | ||
| General metal product manufacturing | |||
| Packaging | 4 (16.00) | ||
| Non-metallic casting material manufacturing | |||
| Manual injection | 1 (4.00) | ||
| Packaging | 1 (4.00) | ||
| Sand coating | 1 (4.00) | ||
| Shooting | 1 (4.00) | ||
| Years of working | 12.40 ± 4.54 | ||
| Anthropometric measurements | |||
| Height (cm) | 167.86 ± 6.12 | ||
| Weight (kg) | 68.34 ± 7.16 | ||
| Shoulder height (cm) | 134.60 ± 5.50 | ||
| Elbow height (cm) | 100.95 ± 3.46 | ||
| Iliac height (cm) | |||
| Left | 88.87 ± 3.48 | ||
| Right | 87.91 ± 4.06 | ||
| Leg length (cm) | |||
| Upper | 37.13 ± 4.24 | ||
| Lower | 47.27 ± 2.98 | ||
| Trunk length (cm) | 54.66 ± 6.75 | ||
| Trunk circumference (cm) | 81.71 ± 3.61 | ||
| Iliac width (cm) | 29.80 ± 2.79 | ||
| Iliac depth (cm) | 19.10 ± 2.85 | ||
| Xiphoid width (cm) | 33.34 ± 2.66 | ||
| Xiphoid depth (cm) | 21.52 ± 2.02 | ||
Table 1 Baseline characteristics of the subjects (n = 25)
Values are mean ± standard deviation or the number of the subjects with percentage, where appropriate.
MMH: manual material handling.

