
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 30; 2018 > Article
- Research Article Mental disorders among workers in the healthcare industry: 2014 national health insurance data
- Min-Seok Kim1, Taeshik Kim1, Dongwook Lee1, Ji-hoo Yook1, Yun-Chul Hong1, Seung-Yup Lee2, Jin-Ha Yoon3, Mo-Yeol Kang4
-
Annals of Occupational and Environmental Medicine 2018;30:31.
DOI: https://doi.org/10.1186/s40557-018-0244-x
Published online: May 3, 2018
1Department of Preventive Medicine, Seoul National University College of Medicine, 103 Daehak-ro, Jongno-gu, Seoul 03080 Republic of Korea
2Department of Psychiatry, Uijeongbu St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 271 Cheonbo-ro, Uijeongbu, Gyeonggi-do Republic of Korea
3Department of Preventive Medicine, Yonsei University College of Medicine, 50-1 Yonsei-ro, Seodaemun-gu, Seoul 03722 Republic of Korea
4Department of Occupational and Environmental Medicine, College of Medicine, The Catholic University of Medicine Korea, 222, Banpo-daero, Seocho-gu, Seoul 06591 Republic of Korea
• Received: February 13, 2018 • Accepted: April 25, 2018
© The Author(s). 2018
Open AccessThis article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Abstract
-
Background Numerous studies have shown that healthcare professionals are exposed to psychological distress. However, since most of these studies assessed psychological distress using self-reporting questionnaires, the magnitude of the problem is largely unknown. We evaluated the risks of mood disorders, anxiety disorders, sleep disorders, and any psychiatric disorders in workers in healthcare industry using Korea National Health Insurance (NHI) claims data from 2014, which are based on actual diagnoses instead of self-evaluation.
-
Methods We used Korea 2014 NHI claims data and classified employees as workers in the healthcare industry, based on companies in the NHI database that were registered with hospitals, clinics, public healthcare, and other medical services. To estimate the standardized prevalence of the selected mental health disorders, we calculated the prevalence of diseases in each age group and sex using the age distribution of the Korea population. To compare the risk of selected mental disorders among workers in the healthcare industry with those in other industries, we considered age, sex, and income quartile characteristics and conducted propensity scored matching.
-
Results In the matching study, workers in healthcare industry had higher odds ratios for mood disorders (1.13, 95% CI: 1.11–1.15), anxiety disorders (1.15, 95% CI: 1.13–1.17), sleep disorders (2.21, 95% CI: 2.18–2.24), and any psychiatric disorders (1.44, 95% CI: 1.43–1.46) than the reference group did. Among workers in healthcare industry, females had higher prevalence of psychiatric disorders than males, but the odds ratios for psychiatric disorders, compared to the reference group, were higher in male workers in healthcare industry than in females.
-
Conclusions The prevalence of mood disorders, anxiety disorders, sleep disorders, and all psychiatric disorders for workers in the healthcare industry was higher than that of other Korean workers. The strikingly high prevalence of sleep disorders could be related to the frequent night-shifts in these professions. The high prevalence of mental health problems among workers in healthcare industry is alarming and requires prompt action to protect the health of the “protectors.”
Background
In modern society, mental illness is an increasingly common problem. The World Health Organization (WHO) estimated the total number of people with depression exceeded 300 million in 2015, and a similar number of people are experiencing anxiety disorders [1]. Depression is the leading cause of global Years Lost due to Disability (YLD), and anxiety disorders were the sixth highest cause in 2015 [2]. These psychiatric disorders are associated with long-term sick leave from the workplace and loss of productivity [3–5].
Mental illness is a major concern in healthcare industries. The mental health of healthcare professionals is especially important, because their mental health is associated with medical errors [6, 7] or decreased performance [8], and these could eventually negatively impact patients’ health. Furthermore, mental health problems experienced by healthcare workers contribute to the high turnover rate [9, 10], which affects the costs of medical institutions through training costs and decreased productivity [11–13]. Combined, these effects put the health of patients at risk.
A number of studies have shown that doctors, nurses, and other healthcare professionals are exposed to psychological distress, such as role conflict, emotional labor, being concerned about medical errors and litigation, as well as experiencing verbal or physical abuse by patients and caregivers or bullying by colleagues [14–17]. In addition, healthcare professionals have a much greater chance of being exposed to long working hours, night work, or shift work. Therefore, they frequently experience sleep problem [18–20]. These work-related stress factors could lead to burnout, and even depression, anxiety disorders, sleep disorders, or other psychiatric disorders [5, 21–27].
However, most of the aforementioned studies have assessed the psychological distress using self-reporting questionnaires. This approach involves limitations, since self-reporting questionnaires do not necessarily accurately reflect the mental health of the participants. Moreover, psychological distress may not always cause a mental disorder due to inter-individual differences in regard to resilience, social support, etc. In fact, a prior study reported that there was a mismatch between high distress levels and clinical depressive disorders or anxiety disorders [28].
Taking these points into account, we aimed to explore the prevalence of mental health disorders in workers in healthcare industry using the actual diagnoses derived from the nationwide Korean National Health Insurance claims data for 2014.
Methods
We used the Korean National Health Insurance (NHI) claims data from January 1 to December 31, 2014 to investigate patients with mental health disorders. The NHI database contains various types of information about healthcare facilities and patients, including the date of visit, total number of patients, diagnoses for claims, prescriptions, admission and discharge, and medical services. Under the health insurance policies, all healthcare facilities in Korea are required to submit the data for medical services they provide to patients to the National Health Insurances Services (NHIS). As the NHIS is prohibited from providing personal identification information to the researchers, information that identifies patients is not included in the data.
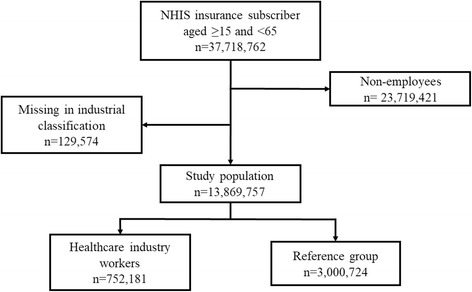
Participants in this study comprised Korean nationals registered as insured employees in the NHIS between the ages of 15 and 64 as of January 1, 2014. Sex, age, insurance fee (20-class), industry classification, and psychiatric disorders (F00-F99, G47) were extracted from the database subject to this analysis. We classified employees as workers in the healthcare industry based on the NHI data for companies registered with hospitals, clinics, public healthcare, and other medical services. We requested the NHI claims data for patients’ age, sex, primary and secondary diagnosis of disease, date of diagnosis, insurance fee, and industry classification of companies. The insurance fees were calculated by the NHIS according to earned income of employees, or estimated income and property of local subscribers. Industry classification was registered based on the company’s report. After the exclusion of non-employees (n = 23,719,421) and participants who were missing an industry classification (n = 129,574), a total of 13,869,757 participants were included in our study (Fig. 1).
Diagnoses were coded according to the sixth revision of the Korean Standard Classification of Diseases, which is based on tenth revision of the Internal Classification of Diseases. We selected three mental disorders: mood disorders (F30–39), anxiety disorders (F41 and F41.0-F41.9), sleep disorders (F51, F51.0-F51.2, F51.8, F51.9, G47, G47.0, G47.1, G47.2, G47.8, and G47.9), as well as any psychiatric disorders (any of F00-F99 and sleep disorders). We excluded sleepwalking, night terrors, nightmares, sleep apnea, narcolepsy, and cataplexy from sleep disorders, because there is a lack of evidence that those conditions are related to job stress. Any patient who was diagnosed with a primary or secondary mood disorder, anxiety disorder, or sleep disorder during the 1-year period was considered as a case for each disease diagnosed. Patients who had been diagnosed with the same disease multiple times were counted once.
To estimate the age-standardized prevalence of selected mental health disorders in the total sample of employees and in the workers in healthcare industry, we calculated the prevalence of the disorders according to age group and sex. Korean population structure data from the 2013 resident population and household status, reported by the Ministry of the Interior and Safety of Korea and presented by Statistics Korea [29], were used for the standard population.
To compare the risk of selected mental health disorders among workers in the healthcare industry and employees in other industries, we selected the reference group from the entire group of insured employees, excluding those working in the healthcare industry, because there were significant differences in characteristics. To achieve balance, we considered age, sex, and income quartile characteristics and conducted greedy matching based on the propensity score. The propensity score is a balancing score of the distribution of measured covariates and can be used to reduce selection bias in observational studies [30]. After 1:4 matching, a final total of 3,008,724 participants were selected as the reference group.
Prevalence of the selected mental health disorders was calculated for the entire sample of insured employees. Odds ratios for the mental health disorders among the insured healthcare employees were calculated as well. To calculate odds ratios, conditional logistic regression was performed due to the matching strategy used. We used SAS version 9.4 for Windows to perform all statistical analyses, and defined statistical significance as p-value < 0.05.
Results
Among all insured employees, females demonstrated a higher percentage of mood disorders (2%), anxiety disorders (2.26%), sleep disorders (2.1%), and any psychiatric disorders (6.53%) compared to males. The most common disorder was anxiety disorder in both sexes. Among workers in healthcare industry, females had a higher percentage of psychiatric disorders than males, except for sleep disorders. Compared with all insured employees, sleep disorders were the most common problem, and the overall frequency of psychiatric disorders was higher in workers in the healthcare industry (Table 1).
Table 1
Prevalence of psychiatric disorders among National Health Insurance service insured employees in Korea (2014)
aMood disorders include diagnosis code of F30~F39 by Korean Standard Classification of Diseases
bAnxiety disorders include diagnosis code of F41 and F41.0~F41.9
cSleep disorders include diagnosis code of F51, F51.0~F51.2, F51.8, F51.9, G47, G47.0, G47.1, G47.2, G47.8, and G47.9
dAny psychiatric disorders include diagnosis code of any of F00~F99 and sleep disorders
Age-standardized 12-month prevalence estimates of selected disorders among all employees were as follows: mood disorders: 1.69% (95% CI: 1.69–1.70), anxiety disorders: 1.93% (95% CI: 1.92–1.93), sleep disorders: 1.76% (95% CI: 1.75–1.77), and any psychiatric disorders: 5.59% (95% CI: 5.59–5.60).
For workers in healthcare industry, prevalence estimates were higher than those for employees in all industries: mood disorders: 1.93% (95% CI: 1.83–2.03), anxiety disorders: 2.18% (95% CI: 2.08–2.07), sleep disorders: 3.47% (95% CI: 3.39–3.54), and any psychiatric disorders: 7.58% (95% CI: 7.43–7.74). The prevalence of all selected mental disorders among females was higher than that of males in both groups (Table 2).
Table 2
Age-standardized prevalence estimate of psychiatric disorders among National Health Insurance service insured employees in Korea (2014)
aMood disorders include diagnosis code of F30~F39 by Korean Standard Classification of Diseases
bAnxiety disorders include diagnosis code of F41 and F41.0~F41.9
cSleep disorders include diagnosis code of F51, F51.0~F51.2, F51.8, F51.9, G47, G47.0, G47.1, G47.2, G47.8, and G47.9
dAny psychiatric disorders include diagnosis code of any of F00~F99 and sleep disorders
After propensity score matching, workers in healthcare industry and those in the reference group were not significantly different with regard to age, income level, and sex (Table 3). The mean age was 37.0 ± 10.5 for healthcare industry workers and 37.1 ± 10.5 for the reference group. The proportion of male workers was 26.18% in both groups. Matching reduced standardized differences for age, sex, and income level.
Table 3
Characteristics of employees before and after propensity score matching among study population
The odds ratios for workers in healthcare industry were higher for mood disorders, anxiety disorders, sleep disorders, and any psychiatric disorders compared to the reference group (Table 4). Risk of sleep disorders was highest in both sexes; odds ratios were 2.21 (95% CI: 2.18–2.24) for the full healthcare sample, and 2.78 (95% CI: 2.69–2.85) for males and 2.05 (95% CI: 2.01–2.09) for females, respectively. For mood disorders, odds ratios were 1.24 (95% CI: 1.19–1.29) for males and 1.10 (95% CI: 1.08–1.12) for females, and for anxiety disorders, 1.19 (95% CI: 1.14–1.23) for males and 1.14 (95% CI: 1.12–1.17) for females, respectively. For any psychiatric disorders, odds ratios were 1.62 (95% CI: 1.59–1.66) for males and 1.39 (95% CI: 1.38–1.41) for females. The odds ratios for mental health disorders were generally higher for male healthcare industry workers than those for female workers, compared with the reference group.
Table 4
Odds ratios of selected psychiatric disorders among workers in healthcare industry versus reference group
aMood disorders includes diagnosis code of F30~F39 by Korean Standard Classification of Diseases
bAnxiety disorders includes diagnosis code of F41 and F41.0~F41.9
cSleep disorders includes diagnosis code of F51, F51.0~F51.2, F51.8, F51.9, G47, G47.0, G47.1, G47.2, G47.8, and G47.9
dAny psychiatric disorders includes diagnosis code of any of F00~F99 and sleep disorders
eNo other covariates included in conditional logistic model
Discussion
This study shows that the prevalence of mood disorders, anxiety disorders, sleep disorders and all psychiatric disorders among workers in healthcare industry was higher than those for workers in other industries. In our study, the reference group was selected from all other industrial workers through propensity score matching method taking age, sex, and income into consideration to investigate the characteristics of workers in the healthcare industry.
In fact, the estimated prevalence of depressive symptoms, anxiety symptoms, and sleep problems in workers in healthcare industry varies among studies and nations. For depressive symptoms, prevalence was estimated as 10% to 28% [8, 31–34], and for anxiety symptoms, prevalence was estimated as 14% to 25% [34–36]. According to the fourth survey of mental disorders, a nationwide sample study of Korean adults (n = 5102) conducted in 2016, the 12-month prevalence of all types of mental disorders listed in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) in Korea was 11.9%. Specifically, the prevalence of mental disorders was as follows: in males, 1.3% for mood disorders, 3.8% for anxiety disorders, and 12.2% for any psychiatric disorders; and in females, 2.5% for mood disorders, 7.5% for anxiety disorders, and 11.5% for any psychiatric disorders [37]. With the exception of mood disorders, the prevalence estimates of disorders in our study were generally lower than those from the fourth survey of mental disorders in Korea. Some of these differences may be due to the difference in study participants. The survey included both workers and non-workers who visited hospitals, while our study only included employees. When we investigated the prevalence of psychiatric disorders among all health insurance subscribers, the prevalence was higher than that in the survey population (data not shown). This implies that there is a strong selection bias—particularly healthy worker effect—for relatively good mental health in employed populations.
Some types of hazardous psychological factors have been reported in the healthcare sector. Possible factors explaining the effects of working in the healthcare sector on mental health disorders include time pressure, low levels of support from supervisors and co-workers, heavy workload, sleep deprivation due to night-shift work, uncertainty regarding decisions, and low autonomy. These workplace stressors negatively affect workers’ mental health [15, 23, 32, 38].
According to previous studies, about 30–40% of healthcare workers suffer from burnout [39–41]. Burnout is an outcome of chronic stress, a state of exhaustion combined with doubts about the value of one’s own work and competence [42]. Burnout has previously been reported to be positively correlated with depression [43]. In a job demand-control model, mismatches between workload and job control increase workers’ stress, which could cause a state of anxiety and aggravate exhaustion [44].
Healthcare workers are also often exposed to conflicts or violent situations [34]. Workers who have experienced physical or emotional violence may feel depressed or anxious. In healthcare facilities, workers must keep working in the place where such an event occurred, and this may contribute to workers being reminded of events and re-experiencing anxiety associated with potential threat [45].
Healthcare workers are under pressure to face patients with empathy instead of expressing negative emotion. Thus, healthcare workers should suppress their negative emotion appropriately. This type of work is called emotional labor. Severe emotional labor is also a job stressor related to burnout and mental disorders [46]. A nationwide study reported that suppressing emotion and engaging with complaining customers were related to depression and anxiety [47].
Sleep disorders were more than twice as high in healthcare workers compared to workers in other industries. A number of previous studies concluded that sleep disorders are common for healthcare workers, due to shift and night work, a well-known risk factor of shift work-related sleep disorders [48], which are more frequent in healthcare compared to other industries. With regard to sleep disorders, somnambulism, night terrors, nightmares, sleep apnea, and narcolepsy were excluded based on a specific diagnostic code. There is a possibility, however, that these disorders were still included in the event that they were categorized as a sleep disorder instead of a specific diagnosis.
This study has several limitations. First, as a cross-sectional study, inferences regarding causation are limited and several biases could have affected the results. Healthcare workers suffering from a mental disorder may have quitted their jobs because they need to utilize emotional intelligence to perform their duties. However, we cannot calculate the magnitude of this healthy worker effect. In general, workers in healthcare facilities have higher knowledge of health and physical accessibility to medical services. In psychiatric disorders, despite of higher accessibility, such knowledge may lead them to be more sensitive to the risk of ‘stigmatization’ by their colleagues or supervisors [49, 50]. The bias caused by differences in accessibility could be verified through comparing outcomes with control-diseases such as rheumatic disease and thyroid disease, but we could not confirm it because such diseases are not included in our data.
Second, the NHI claims data were not designed to be used in studies, so there are limitations with the data. For example, the healthcare industry includes several occupations such as medical doctors, nurses, laboratory technicians, and facility maintenance workers. There could be differences in occupational stress factors and estimated prevalence of mental disorders among these workers. However, there is lack of job information in the NHI claims data. According to the Korea Health Industry Statistics System, the percentages of medical personnel employed in hospitals in Korea comprise about 19% medical doctors, 44% nurses, and 37% other workers [51].
Third, medical records not covered by NHI were excluded from the subject of this study. Most people in the general population worry about possible disadvantages in the workplace caused by psychiatric diagnoses, which, in turn, leads to some patients electing not to apply for national health insurance for treatment to avoid a history of such treatment entering into the public record. Consequently, such cases, not included in the NHI data, were not included in this study. Moreover, since the NHI database does not contain family histories of psychiatric disorders, we could not consider the effect of family history.
Lastly, in terms of clinical aspects, we simply defined mental disorder cases as those for the people who had been diagnosed with mental disorder more than one time, and this could not differentiate the severity of disease. Moreover, diagnoses could have been made by physicians with little expertise in psychiatric evaluation. Further research including dosage and duration of medication, hospitalization, and defining cases with more a sophisticated method is needed.
The strength of our study is the large sample size based on one full year of NHI data related to psychiatric disorders with respect to the entire Korean population of insured employees. To the best of our knowledge, there have not yet been studies on a similar topic with such a massive number of participants.
In addition, most previous studies were based on self-reporting questionnaires; thus, it was hard to assure that prevalence of psychiatric disorders was actually higher among workers in the healthcare industry. This study, however, is distinguished from prior studies in that it is based on actual diagnoses by medical doctors, which are claimed subsequently to the NHIS.
Conclusions
We found the prevalence of mood disorders, anxiety disorders, sleep disorders, and all psychiatric disorders among workers in the healthcare industry was higher compared to workers in other industries in Korea. Therefore, particular attention should be paid to the mental health of workers in healthcare industry. For institutional or governmental mental illness prevention programs, further research is needed on the risk factors and stressors of the actual occupation of healthcare industry workers.
This study was funded by the Occupational Safety and Health Research Institute, Korean Occupational Safety and Health Agency.
The National Health Insurance claims data were provided by the National Health Insurance Services (NHIS), which were fully encoded and used randomized personal identification numbers to make it impossible to identify individuals.
- 1.
- 2.
- 3. Hensing G, Spak F. Psychiatric disorders as a factor in sick-leave due to other diagnoses. A general population-based study. Br J Psychiatry 1998;172:250–256. 10.1192/bjp.172.3.250. 9614475.ArticlePubMed
- 4. Nystuen P, Hagen KB, Herrin J. Mental health problems as a cause of long-term sick leave in the Norwegian workforce. Scand J Soc Med 2001;29:175–182.ArticlePDF
- 5. Michie S, Williams S. Reducing work related psychological ill health and sickness absence: a systematic literature review. Occup Environ Med 2003;60:3–9. 10.1136/oem.60.1.3. 12499449.ArticlePubMedPMC
- 6. Suzuki K, Ohida T, Kaneita Y, Yokoyama E, Miyake T, Harano S, et al. Mental health status, shift work, and occupational accidents among hospital nurses in Japan. J Occup Health 2004;46:448–454. 10.1539/joh.46.448. 15613767.ArticlePubMedPDF
- 7. Shanafelt TD, Balch CM, Bechamps G, Russell T, Dyrbye L, Satele D, et al. Burnout and medical errors among American surgeons. Ann Surg 2010;251:995–1000. 10.1097/SLA.0b013e3181bfdab3. 19934755.ArticlePubMed
- 8. Schwenk TL, Gorenflo DW, Leja LM. A survey on the impact of being depressed on the professional status and mental health care of physicians. The Journal of clinical psychiatry 2008;69:617–620. 10.4088/JCP.v69n0414. 18426258.ArticlePubMed
- 9. Lee Y, Kim K. Experiences of nurse turnover. J Korean Acad Nurs 2008;38:248–257. 10.4040/jkan.2008.38.2.248.Article
- 10. Leiter MP, Maslach C. Nurse turnover: the mediating role of burnout. J Nurs Manag 2009;17:331–339. 10.1111/j.1365-2834.2009.01004.x. 19426369.ArticlePubMed
- 11. Duffield CM, Roche MA, Homer C, Buchan J, Dimitrelis S. A comparative review of nurse turnover rates and costs across countries. J Adv Nurs 2014;70(12):2703. 10.1111/jan.12483. 25052582.ArticlePubMedPDF
- 12. O’Brien-Pallas L, Griffin P, Shamian J, Buchan J, Duffield C, Hughes F, et al. The impact of nurse turnover on patient, nurse, and system outcomes: a pilot study and focus for a multicenter international study. Policy, Politics, & Nursing Practice 2006;7:169–179. 10.1177/1527154406291936.ArticlePubMedPDF
- 13. Misra-Hebert AD, Kay R, Stoller JK. A review of physician turnover: rates, causes, and consequences. Am J Med Qual 2004;19:56–66. 10.1177/106286060401900203. 15115276.ArticlePubMedPDF
- 14. Deckard G, Meterko M, Field D. Physician burnout: an examination of personal, professional, and organizational relationships. Med Care 1994;32(7):745–754. 10.1097/00005650-199407000-00007. 8028408.ArticlePubMed
- 15. Felton JS. Burnout as a clinical entity—its importance in health care workers. Occup Med 1998;48:237–250. 10.1093/occmed/48.4.237.Article
- 16. Firth-Cozens J, Greenhalgh J. Doctors’ perceptions of the links between stress and lowered clinical care. Soc Sci Med 1997;44:1017–1022. 10.1016/S0277-9536(96)00227-4. 9089922.ArticlePubMed
- 17. Ruotsalainen J, Serra C, Marine A, Verbeek J. Systematic review of interventions for reducing occupational stress in health care workers. Scand J Work Environ Health 2008;34:169–178. 10.5271/sjweh.1240. 18728906.ArticlePubMed
- 18.
- 19. Owens JA. Sleep loss and fatigue in healthcare professionals. The Journal of perinatal & neonatal nursing 2007;21:92–100. 10.1097/01.JPN.0000270624.64584.9d. 17505227.ArticlePubMed
- 20. Virtanen M, Ferrie JE, Gimeno D, Vahtera J, Elovainio M, Singh-Manoux A, et al. Long working hours and sleep disturbances: the Whitehall II prospective cohort study. Sleep 2009;32:737–745. 10.1093/sleep/32.6.737. 19544749.ArticlePubMedPMC
- 21. Wall TD, Bolden RI, Borrill CS, Carter AJ, Golya DA, Hardy GE, et al. Minor psychiatric disorder in NHS trust staff: occupational and gender differences. Br J Psychiatry 1997;171:519–523. 10.1192/bjp.171.6.519. 9519089.ArticlePubMed
- 22. McNeely E. The consequences of job stress for nurses’ health: time for a check-up. Nurs Outlook 2005;53:291–299. 10.1016/j.outlook.2005.10.001. 16360700.ArticlePubMed
- 23. Embriaco N, Papazian L, Kentish-Barnes N, Pochard F, Azoulay E. Burnout syndrome among critical care healthcare workers. Curr Opin Crit Care 2007;13:482–488. 10.1097/MCC.0b013e3282efd28a. 17762223.ArticlePubMed
- 24. Hegney DG, Craigie M, Hemsworth D, Osseiran-Moisson R, Aoun S, Francis K, et al. Compassion satisfaction, compassion fatigue, anxiety, depression and stress in registered nurses in Australia: study 1 results. J Nurs Manag 2014;22:506–518. 10.1111/jonm.12160. 24175955.ArticlePubMedPDF
- 25. Kim K, Lee S, Choi YH. Relationship between occupational stress and depressive mood among interns and residents in a tertiary hospital, Seoul, Korea. Clinical and Experimental Emergency Medicine 2015;2:117–122. 10.15441/ceem.15.002. 27752582.ArticlePubMedPMCPDF
- 26. Tomioka K, Morita N, Saeki K, Okamoto N, Kurumatani N. Working hours, occupational stress and depression among physicians. Occup Med 2011;61:163–170. 10.1093/occmed/kqr004.Article
- 27. Ahola K, Honkonen T, Isometsä E, Kalimo R, Nykyri E, Aromaa A, et al. The relationship between job-related burnout and depressive disorders—results from the Finnish health 2000 study. J Affect Disord 2005;88:55–62. 10.1016/j.jad.2005.06.004. 16038984.ArticlePubMed
- 28. Stansfeld SA, Marmot MG. Social class and minor psychiatric disorder in British civil servants: a validated screening survey using the general health questionnaire. Psychol Med 1992;22:739. 10.1017/S0033291700038186. 1410098.ArticlePubMed
- 29. http://kosis.kr.
- 30. Austin PC, Grootendorst P, Anderson GM. A comparison of the ability of different propensity score models to balance measured variables between treated and untreated subjects: a Monte Carlo study. Stat Med 2007;26:734–753. 10.1002/sim.2580. 16708349.ArticlePubMed
- 31. Sohn J-W, Kim B-G, Kim S-H, Han C. Mental health of healthcare workers who experience Needlestick and sharps injuries. J Occup Health 2006;48:474–479. 10.1539/joh.48.474. 17179640.ArticlePubMedPDF
- 32. Gao Y-Q, Pan B-C, Sun W, Wu H, Wang J-N, Wang L. Depressive symptoms among Chinese nurses: prevalence and the associated factors. J Adv Nurs 2012;68:1166–1175. 10.1111/j.1365-2648.2011.05832.x. 21950775.ArticlePubMed
- 33. Wang J-N, Sun W, Chi T-S, Wu H, Wang L. Prevalence and associated factors of depressive symptoms among Chinese doctors: a cross-sectional survey. Int Arch Occup Environ Health 2010;83:905–911. 10.1007/s00420-010-0508-4. 20112108.ArticlePubMedPDF
- 34.
- 35. Mealer ML, Shelton A, Berg B, Rothbaum B, Moss M. Increased prevalence of post-traumatic stress disorder symptoms in critical care nurses. Am J Respir Crit Care Med 2007;175:693–697. 10.1164/rccm.200606-735OC. 17185650.ArticlePubMedPDF
- 36. Mealer M, Burnham EL, Goode CJ, Rothbaum B, Moss M. The prevalence and impact of post traumatic stress disorder and burnout syndrome in nurses. Depression and Anxiety 2009;26:1118–1126. 10.1002/da.20631. 19918928.ArticlePubMedPMC
- 37.
- 38. Leiter MP, Harvie PL. Burnout among mental health workers: a review and a research agenda. Int J Soc Psychiatry 1996;42:90–101. 10.1177/002076409604200203. 8811393.ArticlePubMedPDF
- 39. Gómez-Urquiza JL, De la Fuente-Solana EI, Albendín-García L, Vargas-Pecino C, Ortega-Campos EM, Cañadas-De la Fuente GA. Prevalence of Burnout Syndrome in Emergency Nurses: A Meta-Analysis. Crit Care Nurse 2017;37:e1–e9. 10.4037/ccn2017508. 28966203.Article
- 40. Soler JK, Yaman H, Esteva M, Dobbs F, Asenova RS, Katic M, et al. Burnout in European family doctors: the EGPRN study. Fam Pract 2008;25:245–265. 10.1093/fampra/cmn038. 18622012.ArticlePubMed
- 41. Blanchard P, Truchot D, Albiges-Sauvin L, Dewas S, Pointreau Y, Rodrigues M, et al. Prevalence and causes of burnout amongst oncology residents: a comprehensive nationwide cross-sectional study. Eur J Cancer 2010;46(15):2708. 10.1016/j.ejca.2010.05.014. 20627537.ArticlePubMed
- 42. Maslach C, Jackson SE. Leiter MP Maslach burnout inventory manual. 1996, Palo alto. California: Consulting Psychological Press, Inc.
- 43. Ahola K, Honkonen T, Kivimäki M, Virtanen M, Isometsä E, Aromaa A, et al. Contribution of burnout to the association between job strain and depression: the health 2000 study. J Occup Environ Med 2006;48:1023–1030. 10.1097/01.jom.0000237437.84513.92. 17033502.ArticlePubMed
- 44.
- 45. Cooper CL, Swanson N. Workplace violence in the health sector. 2002, State of the art Geneva: Organización Internacional de Trabajo, Organización Mundial de la Salud, Consejo Internacional de Enfermeras Internacional de Servicios Públicos.
- 46. Jeung D-Y, Lee H-O, Chung WG, Yoon J-H, Koh SB, Back C-Y, et al. Association of Emotional Labor, self-efficacy, and type a personality with burnout in Korean dental hygienists. J Korean Med Sci 2017;32:1423. 10.3346/jkms.2017.32.9.1423. 28776336.ArticlePubMedPMCPDF
- 47. Yoon J-H, Kang M-Y, Jeung D, Chang S-J. Suppressing emotion and engaging with complaining customers at work related to experience of depression and anxiety symptoms: a nationwide cross-sectional study. Ind Health. 2017;55:265–74. 10.2486/indhealth.2016-0069. 28216516.ArticlePubMedPMC
- 48. Wright KP, Bogan RK, Wyatt JK. Shift work and the assessment and management of shift work disorder (SWD). Sleep Med Rev 2013;17:41–54. 10.1016/j.smrv.2012.02.002. 22560640.ArticlePubMed
- 49. Jorm AF, Korten AE, Jacomb PA, Christensen H, Henderson S. Attitudes towards people with a mental disorder: a survey of the Australian public and health professionals. Australian & New Zealand Journal of Psychiatry 1999;33:77–83. 10.1046/j.1440-1614.1999.00513.x. 10197888.ArticlePubMedPDF
- 50. Björkman T, Angelman T, Jönsson M. Attitudes towards people with mental illness: a cross-sectional study among nursing staff in psychiatric and somatic care. Scand J Caring Sci 2008;22:170–177. 10.1111/j.1471-6712.2007.00509.x. 18489686.ArticlePubMed
- 51. Korea Health Industry Development Institute. Healthcare workforce - Number of medical personnel in hospital [Internet]. 2016.
REFERENCES
Notes
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Internal Communication and Dissemination Strategies During Magnet Implementation in German Hospitals: A Qualitative Study
Joan Kleine, Carolin Gurisch, Julia Köppen, Reinhard Busse, Lisa Smeds Alenius, Paolo C. Colet
Journal of Nursing Management.2026;[Epub] CrossRef - Mapping research trajectories of platform working and employee well-being: a bibliometric cartography
Shefali Sharma, Amit Mittal, Seema Seema
Kybernetes.2026; : 1. CrossRef - Does leading through algorithmic management impact the workers’ well-being: a systematic literature review and research agenda
Shefali Sharma, Amit Mittal, Seema Seema
Leadership & Organization Development Journal.2026; 47(2): 218. CrossRef - Craving under pressure: the interplay between hedonic hunger, mental health, and ultra-processed food consumption in shift-workers
Elif Akin, Hatice Merve Bayram, Arda Ozturkcan
Frontiers in Public Health.2026;[Epub] CrossRef - Determinants of anxiety and depression and their association with coping strategies in health professionals in war and conflict-afflicted areas
Maisa Nabulsi, Muna Ahmead, Nuha El Sharif
Frontiers in Psychiatry.2026;[Epub] CrossRef - Effectiveness of Mindfulness-Based Stress Reduction Program on Job Satisfaction and Psychological Distress of Care Workers for Older Adults
Nurgül Karakurt, Meltem Oral
Workplace Health & Safety.2026; 74(7): 352. CrossRef - Tabakabhängigkeit im Gesundheitswesen
Miriam Riedl, Martina Strasser, Alkomiet Hasan, Theresa Halms
InFo Neurologie + Psychiatrie.2026; 28(6): 46. CrossRef - Engaging leadership and nurses’ mental health in German acute care hospitals: the mediating role of job resources
Joan Kleine, Dorothea Kohnen, Alessandro Campione, Reinhard Busse
BMC Nursing.2026;[Epub] CrossRef - Generalized anxiety disorder and major depressive disorder among healthcare professionals in Mbarara city, southwestern Uganda: the relationship with professional quality of life and resilience
Joan Abaatyo, Alain Favina, Margaret Twine, Dan Lutasingwa, Rosemary Ricciardelli, Godfrey Zari Rukundo
BMC Public Health.2025;[Epub] CrossRef - The Impact of Self-Compassion on Enhancing the Professional Quality of Life for Healthcare Workers
Eulji Jung, Young-Eun Jung
Journal of Korean Medical Science.2025;[Epub] CrossRef - Factors associated with depression and anxiety among mental healthcare practitioners
Cheval Murugas, Carla Kotzé
Journal of the Colleges of Medicine of South Africa.2025;[Epub] CrossRef - A Reliability Generalization Meta-Analysis of Scores on the Professional Quality of Life (ProQOL) Scale Across Sample Characteristics
A. Stephen Lenz, Carla Smith, Amber Meegan
Measurement and Evaluation in Counseling and Development.2024; 57(4): 403. CrossRef - Assessment of the importance of sleep quality and the effects of deprivation on Sudanese healthcare professionals amidst conflict in Sudan
Mohammed Hammad Jaber Amin, Musab Awadalla Mohamed Elhassan Elmahi, Gasm Alseed Abdelmonim Gasm Alseed Fadlalmoula, Jaber Hammad Jaber Amin, Noon Hatim Khalid Alrabee, Mohammed Haydar Awad, Zuhal Yahya Mohamed Omer, Nuha Tayseer Ibrahim Abu Dayyeh, Nada A
Sleep Science and Practice.2024;[Epub] CrossRef - Prevalence and predictors of depression and anxiety among workers at two points of entry in Botswana during the COVID-19 pandemic
Keatlaretse Siamisang, Naledi Mokgethi, Leungo Audrey Nthibo, Matshwenyego Boitshwarelo, Onalethata Lesetedi
The Pan African Medical Journal.2024;[Epub] CrossRef - Laying the foundations for implementing Magnet principles in hospitals in Europe: A qualitative analysis
Ingrid Svensson, Jackie Bridges, Jaimie Ellis, Noeleen Brady, Simon Dello, Jonathan Hooft, Joan Kleine, Dorothea Kohnen, Elaine Lehane, Rikard Lindqvist, Claudia B. Maier, Vera J.C. Mc Carthy, Ingeborg Strømseng Sjetne, Lars E. Eriksson, Lisa Smeds Aleniu
International Journal of Nursing Studies.2024; 154: 104754. CrossRef - Transformational nurse leadership attributes in German hospitals pursuing organization-wide change via Magnet® or Pathway® principles: results from a qualitative study
Joan Kleine, Julia Köppen, Carolin Gurisch, Claudia B. Maier
BMC Health Services Research.2024;[Epub] CrossRef - The effect of work-family conflict on employee well-being among physicians: the mediating role of job satisfaction and work engagement
Xin Yang, Xiangou Kong, Meixi Qian, Xiaolin Zhang, Lingxi Li, Shang Gao, Liangwen Ning, Xihe Yu
BMC Psychology.2024;[Epub] CrossRef - Mental Health of Healthcare Workers during COVID-19 Pandemic: Systematic Review and Meta-analysis
Bashar I. Alzghoul
The Open Public Health Journal.2024;[Epub] CrossRef - Evaluation of the mental health status of intensive care unit healthcare workers at the beginning of COVID-19 pandemic
Ceren Meriç Özgündüz, Murat Bıçakçıoğlu, Ayse Sahin Tutak, Arman Özgündüz
Frontiers in Public Health.2024;[Epub] CrossRef - Supporting employees with mental illness and reducing mental illness-related stigma in the workplace: an expert survey
Bridget Hogg, Ana Moreno-Alcázar, Mónika Ditta Tóth, Ilinca Serbanescu, Birgit Aust, Caleb Leduc, Charlotte Paterson, Fotini Tsantilla, Kahar Abdulla, Arlinda Cerga-Pashoja, Johanna Cresswell-Smith, Naim Fanaj, Andia Meksi, Doireann Ni Dhalaigh, Hanna Rei
European Archives of Psychiatry and Clinical Neuroscience.2023; 273(3): 739. CrossRef - Depression and quality of life among Afghan healthcare workers: A cross-sectional survey study
Abdul Qadim Mohammadi, Ahmad Neyazi, Vanya Rangelova, Bijaya Kumar Padhi, Goodness Ogeyi Odey, Molly Unoh Ogbodum, Mark D. Griffiths
BMC Psychology.2023;[Epub] CrossRef - Mental health of health professionals and their perspectives on mental health services in a conflict-affected setting: a qualitative study in health centres in the Gaza Strip during the COVID-19 pandemic
Teisi Tamming, Yuko Otake, Safa'a Aburahma, Mengxin Tan, Anas Shishtawi, Yahya El-Daour, Khalil Hamad, Akihiro Seita
BMJ Open.2023; 13(8): e066552. CrossRef - Psychedelic Use Among Psychiatric Medication Prescribers: Effects on Well-Being, Depression, Anxiety, and Associations with Patterns of Use, Reported Harms, and Transformative Mental States
Zachary Herrmann, Adam W. Levin, Steven P. Cole, Sarah Slabaugh, Brian Barnett, Andrew Penn, Rakesh Jain, Charles Raison, Bhavya Rajanna, Saundra Jain
Psychedelic Medicine.2023; 1(3): 139. CrossRef - COVID-19 and Women’s Mental Health during a Pandemic – A Scoping Review
Nileswar Das, Preethy Kathiresan, Pooja Shakya, Siddharth Sarkar
Indian Journal of Social Psychiatry.2023; 39(1): 4. CrossRef - Urgensi Kepesertaan BPJS Kesehatan Sebagai Syarat Peralihan Hak Atas Tanah Berdasarkan Instruksi Presiden Nomor 1 Tahun 2022 Tentang Optimalisasi Pelaksanaan Program Jaminan Kesehatan Nasional
Nur Dwi Safitri, Fauziyah Fauziyah
Indonesian Journal of Law and Justice.2023; 1(2): 10. CrossRef - Job burnout on subjective wellbeing among clinicians in China: the mediating role of mental health
Yingjie Fu, Derong Huang, Shuo Zhang, Jian Wang
Frontiers in Psychology.2023;[Epub] CrossRef - Evaluation of Mental Health Status of the Pregnant Women Working in
Hospitals During Covid-19 Era: A Cross-Sectional Study
Mahboubeh Eslamzadeh, Bita Najjari, Maryam Emadzadeh, Zhaleh Feyzi, Farzaneh Modaresi, Sara Mirzaeian, Fatemeh Behdani, Aazam Sadat Heydari Yazdi
Current Women s Health Reviews.2023;[Epub] CrossRef - Factors Affecting the Psychological Health of Dental Care Professionals During Pandemic: A Systematic Review
Muhammad Faiz Mohd Hanim, Nursharhani Shariff, Intan Elliayana Mohammed, Mohd Yusmiaidil Putera Mohd Yusof, Budi Aslinie Md Sabri, Norashikin Yusof
Malaysian Journal of Medicine and Health Sciences.2023; 19(s18): 83. CrossRef - A Model of Depression in University Faculty, Staff, and Health Care Workers Using an Automated Mental Health Screening Tool
Sharon Tucker, Bern Melnyk, Lanie Corona, Carlos Corona, Haley Roberts
Journal of Occupational & Environmental Medicine.2022; 64(7): 607. CrossRef - Emotional distress symptoms and their determinants: screening of non-clinical hospital staff in an Egyptian University hospital
Noha M. Ibrahim, Dina A. Gamal-Elden, Mohsen A. Gadallah, Sahar K. Kandil
BMC Psychiatry.2022;[Epub] CrossRef - Influencing Factors of High PTSD Among Medical Staff During COVID-19: Evidences From Both Meta-analysis and Subgroup Analysis
Guojia Qi, Ping Yuan, Miao Qi, Xiuli Hu, Shangpeng Shi, Xiuquan Shi
Safety and Health at Work.2022; 13(3): 269. CrossRef - Sleep Quality among Healthcare Professionals in a Tertiary Care Hospital
Abinaya Ravi, Sivapriya KRS, Neethu George, Rock Britto, Anirudh Parthiban, Nagarajan Anukruthi
National Journal of Community Medicine.2022; 13(4): 213. CrossRef - Study of Complexity Systems in Public Health for Evaluating the Correlation between Mental Health and Age-Related Demographic Characteristics: A General Health Study
Fereshte Haghi, Shadi Goli, Rana Rezaei, Fatemeh Akhormi, Fatemeh Eskandari, Zeinab Nasr Isfahani, Mohsen Ahmadi
Journal of Healthcare Engineering.2022; 2022: 1. CrossRef - High Levels of Self-Reported Depressive Symptoms Among Physical Therapists and Physical Therapist Students Are Associated With Musculoskeletal Pain: A Cross-Sectional Study
Tomer Yona, Asaf Weisman, Uri Gottlieb, Youssef Masharawi
Physical Therapy.2022;[Epub] CrossRef - A workplace organisational intervention to improve hospital nurses’ and physicians’ mental health: study protocol for the Magnet4Europe wait list cluster randomised controlled trial
Walter Sermeus, Linda H Aiken, Jane Ball, Jackie Bridges, Luk Bruyneel, Reinhard Busse, Hans De Witte, Simon Dello, Jonathan Drennan, Lars E Eriksson, Peter Griffiths, Dorothea Kohnen, Julia Köppen, Rikard Lindqvist, Claudia Bettina Maier, Matthew D McHug
BMJ Open.2022; 12(7): e059159. CrossRef - Insomnia and Related Factors During the Delta Wave of the COVID-19 Pandemic in the Kingdom of Bahrain: A Cross-Sectional Study
Fatema Habbash, Afif Ben Salah, Amer Almarabheh, Haitham Jahrami
Nature and Science of Sleep.2022; Volume 14: 1963. CrossRef - Impact of Personality Traits and Socio-Demographic Factors on Depression among Doctors and Nurses
Thapasya Maya
ABC Journal of Advanced Research.2022; 11(1): 1. CrossRef - Sleep of Healthcare Workers During the COVID-19 Pandemic and the Role of Atypical Work Schedules: A Scoping Review
Niamh Power, Michel Perreault, Manuela Ferrari, Philippe Boudreau, Diane B. Boivin
Journal of Biological Rhythms.2022; 37(4): 358. CrossRef - The “Healthcare Workers’ Wellbeing [Benessere Operatori]” Project: A Longitudinal Evaluation of Psychological Responses of Italian Healthcare Workers during the COVID-19 Pandemic
Gaia Perego, Federica Cugnata, Chiara Brombin, Francesca Milano, Emanuele Preti, Rossella Di Pierro, Chiara De Panfilis, Fabio Madeddu, Valentina Elisabetta Di Mattei
Journal of Clinical Medicine.2022; 11(9): 2317. CrossRef - Anxiety, Depression and Burnout Levels of Turkish Healthcare Workers at the End of the First Period of COVID-19 Pandemic in Turkey
Burak Uz, Esra Savaşan, Dila Soğancı
Clinical Psychopharmacology and Neuroscience.2022; 20(1): 97. CrossRef - Working Conditions and Long-Term Sickness Absence Due to Mental Disorders
Noora Heinonen, Tea Lallukka, Jouni Lahti, Olli Pietiläinen, Hilla Nordquist, Minna Mänty, Anu Katainen, Anne Kouvonen
Journal of Occupational & Environmental Medicine.2022; 64(2): 105. CrossRef - Mental Health Outcomes and Mental Hygiene in the COVID-19 Era: A Cross-Sectional Study Among Healthcare Workers from a Regional Hospital in Ghana
Reginald Arthur-Mensah, Genevieve Paintsiwaa Paintsil, Agnes Agudu Delali, Abigail Agartha Kyei
Psychology Research and Behavior Management.2022; Volume 15: 21. CrossRef - Delusional Infestation in Healthcare Professionals: Outcomes from a Multi-Centre Case Series
John Frewen, Peter Lepping, Jonathan M. R. Goulding, Stephen Walker, Anthony Bewley
Skin Health and Disease.2022;[Epub] CrossRef - Challenges facing essential workers: a cross-sectional survey of the subjective mental health and well-being of New Zealand healthcare and ‘other’ essential workers during the COVID-19 lockdown
Caroline Bell, Jonathan Williman, Ben Beaglehole, James Stanley, Matthew Jenkins, Philip Gendall, Charlene Rapsey, Susanna Every-Palmer
BMJ Open.2021; 11(7): e048107. CrossRef - Gender differences in mental health problems of healthcare workers during the coronavirus disease 2019 outbreak
Shuai Liu, Lulu Yang, Chenxi Zhang, Yan Xu, Lidan Cai, Simeng Ma, Ying Wang, Zhongxiang Cai, Hui Du, Ruiting Li, Lijun Kang, Huirong Zheng, Zhongchun Liu, Bin Zhang
Journal of Psychiatric Research.2021; 137: 393. CrossRef - A closer look at the high burden of psychiatric disorders among healthcare workers in Egypt during the COVID-19 pandemic
Amr Ehab El-Qushayri, Abdullah Dahy, Abdullah Reda, Mariam Abdelmageed Mahmoud, Sarah Abdel Mageed, Ahmed Mostafa Ahmed Kamel, Sherief Ghozy
Epidemiology and Health.2021; 43: e2021045. CrossRef - Mental Health Outcomes Amongst Health Care Workers During COVID 19 Pandemic in Saudi Arabia
Maha Al Ammari, Khizra Sultana, Abin Thomas, Lolowa Al Swaidan, Nouf Al Harthi
Frontiers in Psychiatry.2021;[Epub] CrossRef - Burnout and Presenteeism among Healthcare Workers in Nigeria: Implications for Patient Care, Occupational Health and Workforce Productivity
Arinze D.G. Nwosu, Edmund Ossai, Okechukwu Onwuasoigwe, Maureen Ezeigweneme, Jude Okpamen
Journal of Public Health Research.2021;[Epub] CrossRef - An Open Trial of the Effectiveness, Program Usage, and User Experience of Internet-based Cognitive Behavioural Therapy for Mixed Anxiety and Depression for Healthcare Workers on Disability Leave
Andrew Miki, Mark A. Lau, Hoora Moradian
Journal of Occupational & Environmental Medicine.2021; 63(10): 865. CrossRef - Anxiety, depression, trauma-related, and sleep disorders among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis
Maxime Marvaldi, Jasmina Mallet, Caroline Dubertret, Marie Rose Moro, Sélim Benjamin Guessoum
Neuroscience & Biobehavioral Reviews.2021; 126: 252. CrossRef - Moral Injury and Light Triad Traits: Anxiety and Depression in Health-Care Personnel During the Coronavirus-2019 Pandemic in Honduras
Elizabeth A. Rodríguez, Maitée Agüero-Flores, Miguel Landa-Blanco, David Agurcia, Cindy Santos-Midence
Hispanic Health Care International.2021; 19(4): 230. CrossRef - Mental Disorders Among Health Care Workers at the Early Phase of COVID-19 Pandemic in Kenya; Findings of an Online Descriptive Survey
Edith Kamaru Kwobah, Ann Mwangi, Kirtika Patel, Thomas Mwogi, Robert Kiptoo, Lukoye Atwoli
Frontiers in Psychiatry.2021;[Epub] CrossRef - Association of Sickness Absence With Severe Psychiatric Outcomes in a Brazilian Health Workforce
Claudia Szlejf, Aline Kumow, Rafael Dadão, Etienne Duim, Vanessa Moraes Assalim
Journal of Occupational & Environmental Medicine.2020; 62(10): e543. CrossRef Obstetrics Healthcare Providers’ Mental Health and Quality of Life During COVID-19 Pandemic: Multicenter Study from Eight Cities in Iran
Homeira Vafaei, Shohreh Roozmeh, Kamran Hessami, Maryam Kasraeian, Nasrin Asadi, Azam Faraji, Khadije Bazrafshan, Najmieh Saadati, Soudabeh Kazemi Aski, Elahe Zarean, Mahboobeh Golshahi, Mansoureh Haghiri, Nazanin Abdi, Reza Tabrizi, Bahram Heshmati, Elha
Psychology Research and Behavior Management.2020; Volume 13: 563. CrossRef- Ethical dilemmas faced by health care workers during COVID-19 pandemic: Issues, implications and suggestions
Vikas Menon, Susanta Kumar Padhy
Asian Journal of Psychiatry.2020; 51: 102116. CrossRef - Surgical Locker room Environment: Understanding the Hazards (SLEUTH) study
Rowan David, Bridget Heijkoop, Arman A. Kahokehr
ANZ Journal of Surgery.2020; 90(10): 1943. CrossRef - Anxiety and hopelessness levels in COVID-19 pandemic: A comparative study of healthcare professionals and other community sample in Turkey
Yunus Hacimusalar, Aybeniz Civan Kahve, Alisan Burak Yasar, Mehmet Sinan Aydin
Journal of Psychiatric Research.2020; 129: 181. CrossRef - The relationship between occupational stress, psychological distress symptoms, and social support among Jordanian healthcare professionals
Wafa'a F. Ta'an, Tariq N. Al‐Dwaikat, Khulod Dardas, Ahmad H. Rayan
Nursing Forum.2020; 55(4): 763. CrossRef - Psychological interventions to foster resilience in healthcare professionals
Angela M Kunzler, Isabella Helmreich, Andrea Chmitorz, Jochem König, Harald Binder, Michèle Wessa, Klaus Lieb
Cochrane Database of Systematic Reviews.2020;[Epub] CrossRef - DANGER! Crisis Health Workers at Risk
Mason Harrell, Saranya A. Selvaraj, Mia Edgar
International Journal of Environmental Research and Public Health.2020; 17(15): 5270. CrossRef - Burnout, Mental Health, and Quality of Life Among Employees of a Malaysian Hospital: A Cross-sectional Study
Luke Sy-Cherng Woon, Chea Ping Tiong
Annals of Work Exposures and Health.2020; 64(9): 1007. CrossRef - Job Satisfaction and Psychiatric Morbidity among Resident Doctors in Selected Teaching Hospitals in Southern Nigeria: A web-based Survey
Segun Bello, Rotimi Felix Afolabi, David Ayobami Adewole
Journal of Occupational Health and Epidemiology.2019; 8(4): 199. CrossRef - Health anxiety in medical employees: A multicentre study
Qingsong Chen, Yuqun Zhang, Dongyun Zhuang, Xueqin Mao, Guolin Mi, Dijuan Wang, Xiangdong Du, Zhenghui Yi, Xinhua Shen, Yuxiu Sui, Huajie Li, Yin Cao, Zufu Zhu, Zhenghua Hou, Qibin Li, Yonggui Yuan
Journal of International Medical Research.2019; 47(10): 4854. CrossRef - Sleep problems of healthcare workers in tertiary hospital and influencing factors identified through a multilevel analysis: a cross-sectional study in China
Huan Liu, Jingjing Liu, Mingxi Chen, Xiao Tan, Tong Zheng, Zheng Kang, Lijun Gao, Mingli Jiao, Ning Ning, Libo Liang, Qunhong Wu, Yanhua Hao
BMJ Open.2019; 9(12): e032239. CrossRef - Exploring the Knowledge, Attitudes, and Behavioural Responses of Healthcare Students towards Mental Illnesses—A Qualitative Study
Taylor Riffel, Shu-Ping Chen
International Journal of Environmental Research and Public Health.2019; 17(1): 25. CrossRef
 Cite
CiteMental disorders among workers in the healthcare industry: 2014 national health insurance data
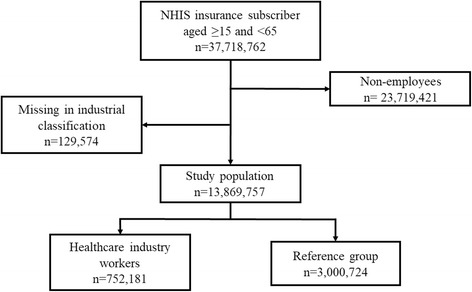
Fig. 1 Flow chart of the study population
Fig. 1
Mental disorders among workers in the healthcare industry: 2014 national health insurance data
| Prevalence cases | All insured employees | Workers in healthcare industry | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Both (n = 13,869,767) | % | Male (n = 8,535,138) | % | Female (n = 5,334,629) | % | Both (n = 752,181) | % | Male (n = 196,957) | % | Female (n = 555,224) | % | |
| Mood disordersa | 217,752 | 1.57 | 111,269 | 1.30 | 106,483 | 2.00 | 13,709 | 1.82 | 3089 | 1.57 | 10,620 | 1.91 |
| Anxiety disordersb | 250,895 | 1.81 | 130,570 | 1.50 | 120,325 | 2.26 | 15,570 | 2.07 | 3528 | 1.79 | 12,042 | 2.17 |
| Sleep disordersc | 228,119 | 1.64 | 116,208 | 1.36 | 111,911 | 2.10 | 24,965 | 3.32 | 6861 | 3.48 | 18,104 | 3.26 |
| Any psychiatric disordersd | 728,767 | 5.25 | 380,223 | 4.45 | 348,544 | 6.53 | 55,139 | 7.33 | 13,512 | 6.86 | 41,627 | 7.50 |
| Age-standardized prevalence estimate (%) | All insured employees | Workers in healthcare industry | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Both | 95% CI | Male | 95% CI | Female | 95% CI | Both | 95% CI | Male | 95% CI | Female | 95% CI | |
| Mood disordersa | 1.69 | 1.68–1.70 | 1.30 | 1.29–1.31 | 2.08 | 2.07–2.10 | 1.93 | 1.83–2.03 | 1.63 | 1.45–1.81 | 2.24 | 2.17–2.31 |
| Anxiety disordersb | 1.93 | 1.92–1.93 | 1.49 | 1.48–1.50 | 2.37 | 2.36–2.39 | 2.18 | 3.39–3.54 | 1.83 | 1.66–1.99 | 2.53 | 2.46–2.60 |
| Sleep disordersc | 1.76 | 1.75–1.77 | 1.33 | 1.32–1.34 | 2.20 | 2.18–2.21 | 3.47 | 2.08–2.27 | 3.33 | 3.21–3.45 | 3.62 | 3.53–3.71 |
| Any psychiatric disordersd | 5.59 | 5.57–5.60 | 4.38 | 4.36–4.40 | 6.83 | 6.80–6.85 | 7.58 | 7.43–7.74 | 6.77 | 6.50–7.04 | 8.43 | 8.30–8.56 |
| Variables | All insured employees | Workers in healthcare industry | Reference group | Standardized differencea | ||||
|---|---|---|---|---|---|---|---|---|
| (n = 13,869,767) | % | (n = 752,181) | % | (n = 3,008,724) | % | pre-match | post-match | |
| Age | − 0.328 | 0.000 | ||||||
| < 20 | 100,403 | 0.72 | 2578 | 0.34 | 10,312 | 0.34 | ||
| 20–29 | 2,424,686 | 17.48 | 218,899 | 29.10 | 875,596 | 29.10 | ||
| 30–39 | 4,151,253 | 29.93 | 239,610 | 31.86 | 958,440 | 31.86 | ||
| 40–49 | 3,942,566 | 28.43 | 180,096 | 23.94 | 720,384 | 23.94 | ||
| 50–59 | 2,721,879 | 19.62 | 93,849 | 12.48 | 375,396 | 12.48 | ||
| ≥60 | 528,980 | 3.81 | 17,149 | 2.28 | 68,596 | 2.28 | ||
| Mean | 40.4 ± 10.8 | 37.0 ± 10.5 | 37.1 ± 10.5 | |||||
| Income level | −0.056 | 0.000 | ||||||
| Q1 | 3,471,369 | 25.03 | 163,190 | 21.70 | 652,760 | 21.70 | ||
| Q2 | 3,440,340 | 24.80 | 247,161 | 32.86 | 988,644 | 32.86 | ||
| Q3 | 3,483,627 | 25.12 | 186,525 | 24.80 | 746,100 | 24.80 | ||
| Q4 | 3,474,431 | 25.05 | 155,305 | 20.65 | 621,220 | 20.65 | ||
| Sex | −0.056 | 0.000 | ||||||
| Male | 8,535,138 | 61.54 | 196,957 | 26.18 | 787,828 | 26.18 | ||
| Female | 5,334,629 | 38.46 | 555,224 | 73.82 | 2,220,896 | 73.82 | ||
| Mood disordersa | Anxiety disordersb | Sleep disordersc | Any psychiatric disordersd | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of cases (%) | ORe | 95%CI | Number of cases (%) | ORe | 95%CI | Number of cases (%) | ORe | 95%CI | Number of cases (%) | ORe | 95%CI | |
| Both | ||||||||||||
| Workers in healthcare industry | 13,709 (1.82) | 1.13 | 1.11 - 1.15 | 15,570 (2.07) | 1.15 | 1.13 - 1.17 | 24,965 (3.32) | 2.21 | 2.18 - 2.24 | 55,139 (7.33) | 1.44 | 1.43 - 1.46 |
| Reference group | 48,769 (1.62) | 1 | 54,266 (1.80) | 1 | 46,197 (1.54) | 1 | 156,902 (5.21) | 1 | ||||
| Male | ||||||||||||
| Workers in healthcare industry | 3,089 (1.57) | 1.24 | 1.19 - 1.29 | 3,528 (1.79) | 1.19 | 1.14 - 1.23 | 6,861 (3.48) | 2.78 | 2.69 - 2.86 | 13,512 (6.86) | 1.62 | 1.59 - 1.66 |
| Reference group | 10,037 (1.27) | 1 | 11,952 (1.52) | 1 | 10,172 (1.29) | 1 | 34,362 (4.36) | 1 | ||||
| Female | ||||||||||||
| Workers in healthcare industry | 10,620 (1.91) | 1.10 | 1.08 - 1.12 | 12,042 (2.17) | 1.14 | 1.12 - 1.17 | 18,104 (3.26) | 2.05 | 2.01 - 2.09 | 41,627 (7.50) | 1.39 | 1.38 - 1.41 |
| Reference group | 38,732 (1.74) | 1 | 42,314 (1.91) | 1 | 36,025 (1.62) | 1 | 122,540 (5.52) | 1 | ||||
Table 1 Prevalence of psychiatric disorders among National Health Insurance service insured employees in Korea (2014)
aMood disorders include diagnosis code of F30~F39 by Korean Standard Classification of Diseases
bAnxiety disorders include diagnosis code of F41 and F41.0~F41.9
cSleep disorders include diagnosis code of F51, F51.0~F51.2, F51.8, F51.9, G47, G47.0, G47.1, G47.2, G47.8, and G47.9
dAny psychiatric disorders include diagnosis code of any of F00~F99 and sleep disorders
Table 2 Age-standardized prevalence estimate of psychiatric disorders among National Health Insurance service insured employees in Korea (2014)
aMood disorders include diagnosis code of F30~F39 by Korean Standard Classification of Diseases
bAnxiety disorders include diagnosis code of F41 and F41.0~F41.9
cSleep disorders include diagnosis code of F51, F51.0~F51.2, F51.8, F51.9, G47, G47.0, G47.1, G47.2, G47.8, and G47.9
dAny psychiatric disorders include diagnosis code of any of F00~F99 and sleep disorders
Table 3 Characteristics of employees before and after propensity score matching among study population
aStandardized differences in age was calculated by categorical variables of age group
Table 4 Odds ratios of selected psychiatric disorders among workers in healthcare industry versus reference group
aMood disorders includes diagnosis code of F30~F39 by Korean Standard Classification of Diseases
bAnxiety disorders includes diagnosis code of F41 and F41.0~F41.9
cSleep disorders includes diagnosis code of F51, F51.0~F51.2, F51.8, F51.9, G47, G47.0, G47.1, G47.2, G47.8, and G47.9
dAny psychiatric disorders includes diagnosis code of any of F00~F99 and sleep disorders
eNo other covariates included in conditional logistic model

