
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 38; 2026 > Article
- Original Article Association between relative handgrip strength and glycemic control among male automobile manufacturing workers using vibration tools in South Korea
-
Dong-Jae Seo1
 , Hyun Joong Kim1, Yongjin Kim1, Jaewon Mun1, Jong-Han Leem1,2, Shin-Goo Park1,2, Dong-Wook Lee1,2, Hwan-Cheol Kim1,2,*
, Hyun Joong Kim1, Yongjin Kim1, Jaewon Mun1, Jong-Han Leem1,2, Shin-Goo Park1,2, Dong-Wook Lee1,2, Hwan-Cheol Kim1,2,* -
Annals of Occupational and Environmental Medicine 2026;38:e14.
DOI: https://doi.org/10.35371/aoem.2026.38.e14
Published online: April 8, 2026
1Department of Occupational and Environmental Medicine, Inha University Hospital, Incheon, Korea
2Department of Social and Preventive Medicine, Inha University College of Medicine, Incheon, Korea
- *Corresponding author: Hwan-Cheol Kim Department of Occupational and Environmental Medicine, Inha University Hospital, Inha University College of Medicine, 27 Inhang-ro, Jung-gu, Incheon 22332, Korea E-mail: carpediem@inha.ac.kr
• Received: November 21, 2025 • Revised: March 30, 2026 • Accepted: April 1, 2026
© 2026 Korean Society of Occupational & Environmental Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,179 Views
- 50 Download
Abstract
-
Background Although the association between handgrip strength and glycemic control has been reported, studies conducted exclusively within specific occupational groups remain limited. To explore the association between handgrip strength and metabolic health in industrial settings, this study examined the relationship between relative handgrip strength and glycated hemoglobin (HbA1c) among male automobile manufacturing workers using vibration tools in South Korea.
-
Methods Using 66,212 occupational health examination records collected at Inha University Hospital between January 2024 and April 2025, a total of 3,365 workers with HbA1c and handgrip strength measurements were identified. After excluding duplicates (n = 1,536), female workers (n = 2), and records without Hb and estimated glomerular filtration rate, 1,823 male participants were included in the final analysis. Relative handgrip strength was calculated as the maximum value of bilateral grip strength divided by body mass index. Multiple linear regression analyses were conducted to assess the association between relative handgrip strength and HbA1c, adjusting for age, smoking status, alcohol consumption, current hypertension, current dyslipidemia, current hypoglycemic-agents use, family diabetes history, leisure-time physical activity, and resistance exercise.
-
Results Relative handgrip strength was inversely associated with HbA1c levels (B: –0.060; 95% confidence interval [CI]: −0.081 to −0.039; p < 0.001). The association was strongest among normoglycemic participants (B: −0.185; 95% CI: −0.305 to −0.065; p = 0.003). Effect size was reduced but significantly associated among individuals with prediabetes (B: −0.115; 95% CI: −0.180 to −0.050; p < 0.001) and further attenuated to a borderline significance in individuals with diabetes (B: −0.023; 95% CI: −0.050 to 0.003; p = 0.082). These findings indicate that greater muscle strength relative to body size is related to better glycemic control.
-
Conclusions Handgrip strength was associated with HbA1c levels in industrial workers. This study suggests that handgrip strength may provide complementary information on metabolic health in occupational settings.
BACKGROUND
Diabetes mellitus, alongside hypertension and hyperlipidemia, is a prevalent chronic metabolic syndrome, characterized by impaired regulation of blood glucose levels due to mechanisms including insulin resistance.1,2 It is a well-established risk factor for micro- and macrovascular complications.3 Therefore, diabetes is a leading cause of mortality and morbidity globally.2 In South Korea, the prevalence of diabetes continues to rise annually.4,5
Glycated hemoglobin (HbA1c) is a biomarker that reflects average blood glucose levels over the preceding 3 months and serves as an indicator for the diagnosis and management of diabetes.6 Poor HbA1c control is associated with a higher incidence of cardiovascular complications and increased mortality attributable to these conditions.7 However, HbA1c levels are not determined by glycemia alone.8 Because HbA1c is expressed as the proportion of glycated to total hemoglobin, it is influenced by red blood cell (RBC) lifespan and hemoglobin concentration or variants. Prolonged RBC survival can lead to higher HbA1c values at a given average glucose level, whereas conditions that shorten RBC life span may result in spuriously low HbA1c.9 Additionally, iron or vitamin B12 deficiency and certain anemia can cause discrepancies between HbA1c and actual glycemic status.10,11
Chronic kidney disease is another important non-glycemic determinant of HbA1c.12 In individuals with impaired kidney function, the uremia-related carbamylation of hemoglobin and alterations in RBC survival may distort the relationship between HbA1c and true average glucose levels.13 Thus, reduced estimated glomerular filtration rate (eGFR) and anemia can affect HbA1c independently of serum glucose, and HbA1c may be an imperfect surrogate for chronic glycemia in the presence of advanced kidney disease.
Skeletal muscles are a major reservoir for blood glucose, with insulin playing a critical role in facilitating glucose uptake into muscle tissue.14 An increase in skeletal muscle mass enhances muscle strength; when insulin secretion effectively promotes glucose transport into muscles, glycemic control can be considered favorable. However, a decrease in muscle mass is associated with increased insulin resistance, thereby contributing to diabetes progression.15 Additionally, a decrease in muscle strength has been observed in individuals with diabetes, and evidence suggests that increasing muscle strength through exercise improves glycemic control.16 A bidirectional relationship exists between skeletal muscle loss and diabetes.17
Handgrip strength is a noninvasive measurement that can be performed repeatedly in any setting using a dynamometer, making it a convenient and practical tool. It is an indicator of sarcopenia, increasingly regarded as the “new vital sign,” as it does not require blood samples or other invasive procedures.18 Because handgrip strength tends to increase with body weight, the handgrip strength-to-body mass index (BMI) ratio has been proposed as a more reliable biomarker.19,20
The associations among diabetes control, HbA1c, and handgrip strength in the general population have been explored. Large-scale epidemiological studies, including the UK Biobank21 and Prospective Urban Rural Epidemiology (PURE) study,22 have demonstrated that reduced handgrip strength is independently associated with all-cause and cardiovascular mortality across diverse populations. These findings have reinforced the value of handgrip strength as a simple yet powerful indicator of overall health and longevity, supporting its potential inclusion in public health surveillance systems. However, research conducted exclusively among manufacturing workers remains limited.
In industrial contexts, workers are frequently exposed to vibration tools, repetitive manual labor, and long working hours, which may all affect muscular and metabolic functions.23,24 This study focused on automobile manufacturing workers, whose regular tasks involved the use of vibration tools. Given this shared exposure, the study aimed to determine whether the associations between handgrip strength and glycemic control observed in the general population are consistently present within this occupational group. We incorporated duration of employment as a factor, recognizing that prolonged exposure to occupational hazards may further influence these relationships. By stratifying participants based on employment duration, we sought to explore how work-related factors affect the relationship between handgrip strength and glycemic control.
METHODS
This cross-sectional observational study investigated the association between relative handgrip strength and glycemic control among male automobile manufacturing workers using vibration tools in South Korea. Data were obtained from occupational health examinations at Inha University Hospital between January 2024 and April 2025. We analyzed 66,212 health examination records. Of these, 3,365 records containing complete data for HbA1c and handgrip strength were identified, whereas 62,847 records missing either variable were excluded. After excluding 1,536 duplicate entries, two female workers, and records without Hb and eGFR data, 1,823 male automobile manufacturing workers were included (Fig. 1).
Handgrip strength data were collected only from workers whose regular tasks involved the use of vibration tools. Handgrip strength was measured in a standing position with the elbow and wrist fully extended using a handheld digital dynamometer (T.K.K.5401, Takei Scientific Instruments Co. Ltd., Tokyo, Japan). Relative handgrip strength was calculated by dividing the maximum value from either hand by the BMI.25
Type 2 diabetes was defined according to the American Diabetes Association criteria26 as a fasting plasma glucose level ≥126 mg/dL, HbA1c level ≥6.5%, or hypoglycemic-agents use. Prediabetes was defined as HbA1c levels of 5.7%–6.4% or fasting plasma glucose levels of 100–126 mg/dL, without meeting the criteria for diabetes.
Employment duration was defined as the total number of years worked since joining the factory. Participants were stratified by employment duration into four categories: 0–5, 6–10, 11–20, and >20 years.
The analysis included the following variables: age, hemoglobin, eGFR, smoking status (never, former, current), alcohol consumption (non-drinker, drinker), current hypertension, current hyperlipidemia, current hypoglycemic-agents use, family diabetes history, participation in leisure-time physical activity (LTPA), and engagement in resistance exercise. Serum creatinine was measured, eGFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) creatinine equation. LTPA was categorized as low, moderate, and high according to World Health Organization recommendations; resistance exercise was categorized by weekly frequency (0, 1–2, and ≥3 sessions).
All statistical analyses were conducted using IBM SPSS Statistics for Windows, version 27.0 (IBM Corp., Armonk, NY, USA). Linear regression analyses were performed to evaluate the association between relative handgrip strength and HbA1c levels. Model 1 was adjusted for age only; model 2 was additionally adjusted for hemoglobin, eGFR, smoking status, alcohol consumption, current hypertension, current hyperlipidemia, current hypoglycemic-agents use, family diabetes history, LTPA, and resistance exercise. Subgroup analyses were conducted for participants categorized into the normoglycemic, prediabetes, and diabetes groups to compare associations across different glycemic status groups. Participants were stratified by employment duration to explore potential interactions between employment duration and the association between handgrip strength and HbA1c. Interaction effects between handgrip strength, HbA1c, and employment duration were assessed. Descriptive statistics were presented as means and standard deviations for continuous variables and as percentages for categorical variables. A p-value of <0.05 was considered statistically significant. Ninety-five percent confidence intervals (95% CI) were reported for all estimates. Forest plots of regression coefficients and 95% CIs were generated using R version 4.5.1 (R Foundation for Statistical Computing, Vienna, Austria).
This retrospective analysis of existing occupational health examination records was approved by the Institutional Review Board of Inha University Hospital (IRB No. 2025-10-017). Given the retrospective design and minimal risk to participants, the IRB waived the requirement for obtaining informed consent, and all data were de-identified and analyzed in an anonymized form.
RESULTS
Table 1 presents descriptive statistics of the study population. A total of 1,823 male automobile factory workers were included, with a mean age of 48.54 years (standard deviation [SD]: 7.88) and a mean BMI of 25.17 kg/m² (SD: 3.27). The mean relative handgrip strength was 1.72 (SD: 0.30). Regarding glycemic status, the mean fasting glucose was 106.29 mg/dL (SD: 25.84), mean HbA1c was 5.84% (SD: 0.80), mean Hb was 15.13 g/dL (SD: 1.03), and mean eGFR was 101.35 mL/min/1.73 m2 (SD: 11.61). The mean employment duration was 20.55 years (SD: 11.30), with most participants being long-term employees (46.0% with >20 years of employment). The prevalence of type 2 diabetes mellitus (T2DM) was 15.9%, with 31.4% normoglycemic and 52.7% prediabetic.
Table 2 presents the results of linear regression analyses examining the association between HbA1c and relative handgrip strength in the overall study population (n = 1,823). Each 1% increase in HbA1c level was significantly associated with lower relative handgrip strength. In model 1, the regression coefficient was –0.069 (95% CI: −0.086 to −0.052; p < 0.001). This association remained statistically significant after full adjustment for hemoglobin, eGFR, current hypertension, current hyperlipidemia, hypoglycemic-agents use, family diabetes history, smoking status, alcohol consumption, LTPA, and resistance exercise (model 2: B: −0.060; 95% CI: −0.081 to −0.039; p < 0.001).
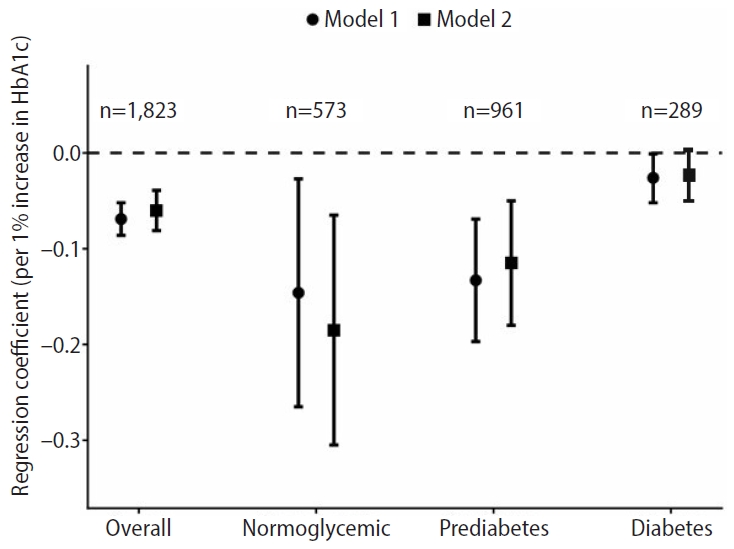
Table 3 presents the results of subgroup analyses stratified by diabetes status. Stronger associations were observed among normoglycemic participants (n = 573), where HbA1c was inversely associated with relative handgrip strength in models 1 (B: −0.146; 95% CI: −0.265 to −0.027; p = 0.016) and 2 (B: −0.185; 95% CI: −0.305 to −0.065; p = 0.003). Among participants with prediabetes (n = 961), a significant inverse association was observed (model 1: B: −0.133; 95% CI: −0.197 to −0.069; p < 0.001; model 2: B: −0.115; 95% CI: −0.180 to −0.050; p < 0.001). Conversely, among participants with diabetes (n = 289), a borderline association was observed (model 1: B: −0.026; 95% CI: −0.052 to −0.001; p = 0.046; model 2: B: −0.023, 95% CI: −0.050 to 0.003, p = 0.082). Associations shown in Tables 2 and 3 are visually summarized in Fig. 2.
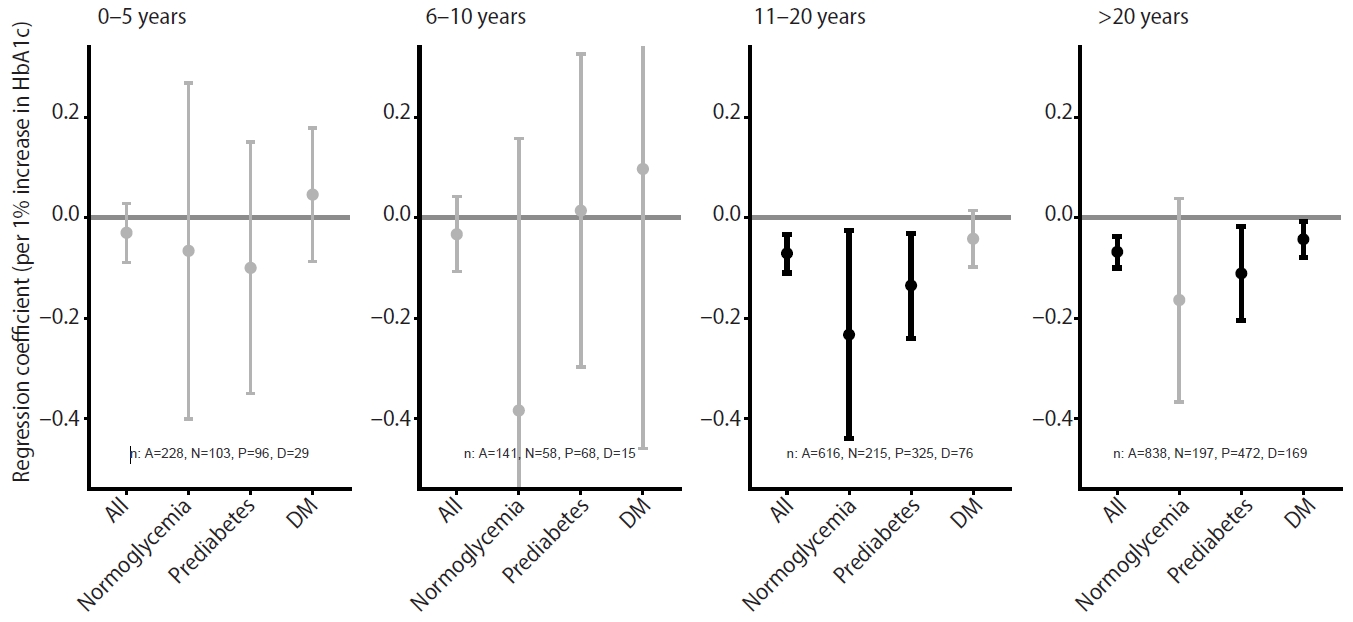
We further conducted stratified analyses by employment duration (Supplementary Table 1), which are visualized in Fig. 3 for the fully adjusted model. Across all categories (0–5 years [n = 228], 6–10 years [n = 141], 11–20 years [n = 616], and >20 years [n = 838]), the regression coefficients for the association between HbA1c and relative handgrip strength were generally negative, although some estimates did not reach statistical significance or showed wider confidence intervals especially in smaller subgroups. The clearest and most consistent inverse associations were observed among long-term employees (11–20 and >20 years). For employees with 11–20 years of employment, the association was significant in models 1 (B: −0.085; 95% CI: −0.117 to −0.053; p < 0.001) and 2 (B: −0.071; 95% CI: −0.110 to −0.033; p < 0.001). Similarly, for employees with >20 years, significant inverse associations were observed in models 1 (B: −0.064; 95% CI: −0.088 to −0.040; p < 0.001) and 2 (B: −0.068; 95% CI: −0.100 to −0.037; p < 0.001). Although several groups with smaller sample sizes showed non-significant or less precise estimates, the overall pattern across duration categories was compatible with an inverse relationship between HbA1c and relative handgrip strength. Within the longer employment, this inverse association was observed across the normoglycemic, prediabetes, and diabetes subgroups, with relatively larger effect sizes generally seen in workers with normoglycemia, consistent with the diabetes-stratified analyses in Table 3.
The interaction between HbA1c and duration of employment was not statistically significant in either the age-adjusted (model 1, p-for-interaction = 0.608) or fully adjusted model (model 2, p-for-interaction = 0.335) (Supplementary Table 2), indicating that the inverse association between HbA1c and relative handgrip strength was consistent and homogeneous across different employment durations.
DISCUSSION
Handgrip strength has evolved from a simple indicator of muscular force and has been increasingly recognized as the “new vital sign” due to its clinical and prognostic relevance.18 Previous studies have demonstrated significant associations between handgrip strength and all-cause mortality, cardiovascular disease, and risk of falls, underscoring its potential as a marker of healthy longevity.27,28 Because it is noninvasive, easy to measure, and highly reproducible, handgrip strength is a practical biomarker for clinical, occupational, and epidemiological settings.18 Building on this practical utility, this study specifically examined the relationship between handgrip strength and HbA1c levels among male automobile manufacturing workers, a group exposed to characteristic occupational factors such as vibration, repetitive manual labor, and long working hours.
In this study, relative handgrip strength demonstrated a significant negative correlation with HbA1c levels after adjustment. The association was the strongest among participants with normoglycemia followed by those with prediabetes, a borderline association was observed among participants with diabetes. Importantly, we did not compare vibration-exposed workers with a non-exposed reference group; instead, we evaluated whether the inverse association between relative handgrip strength and HbA1c, in the general population, was present within a relatively homogeneous group of vibration-exposed automobile manufacturing workers. The inverse association was generally consistent across employment durations, and no meaningful interaction was observed. This indicates that employment duration did not modify the observed inverse association between HbA1c and relative handgrip strength. The attenuated association among individuals with diabetes may reflect a healthy worker effect, as those with advanced disease or substantial muscle weakness are less likely to participate in automobile manufacturing due to early retirement or medical leave. Therefore, the analyzed population may represent relatively healthier individuals with diabetes, potentially underestimating the true relationship between muscle weakness and glycemic control. Additionally, the potential effect of hypoglycemic-agents should be considered. Glucose‑lowering medications can reduce HbA1c levels regardless of current muscle strength; however, better glycemic control may help preserve muscle function. Therefore, the net impact of medication use on the observed association between relative handgrip strength and HbA1c in the diabetes subgroup is complex and was difficult to clarify in this study. Because detailed information on diabetes duration and treatment regimen was unavailable, residual confounding by medication use and disease severity cannot be excluded.
In a previous study conducted among the South Korean general population, individuals with diabetes in the lowest tertile of handgrip strength exhibited poorer glycemic control than those in the highest tertile.29 Similarly, a large-scale, population-based study in the United Kingdom reported that each 1 mmol/mol increase in HbA1c levels was associated with a 4% higher risk of sarcopenia.21 The findings of this study are consistent with these prior results, supporting the view that higher relative handgrip strength is associated with lower HbA1c levels and may be linked to a lower likelihood of diabetes.30 In another study using Korea National Health and Nutrition Examination Survey (KNHANES)31 data, the mean relative handgrip strength among Korean men aged 20–65 years was 1.80, based on nationally representative age-stratified reference values. In this study of male automobile manufacturing workers, the mean relative handgrip strength was 1.72, slightly lower but broadly comparable to the general population values. This similarity suggests that, despite repetitive manual labor, long working hours, and routine use of vibration tools, automobile workers do not exhibit markedly higher grip strength than Korean men; The observed inverse association between HbA1c and relative handgrip strength appears to be consistent with patterns in the general population rather than being uniquely driven by occupational demands. The relationship between muscle strength and glucose metabolism may be bidirectional. Reduced muscle strength may aggravate insulin resistance, while chronic hyperglycemia accelerates muscle protein degradation and mitochondrial dysfunction, leading to progressive muscle weakness.32
Skeletal muscle serves as the primary metabolic organ responsible for approximately 80%–85% of glucose uptake in the body,33 with glucose entering muscle cells through the glucose transporter type 4 (GLUT4) transporter.34 GLUT4 translocation to the cell membrane occurs via two distinct mechanisms: the insulin-dependent and insulin-independent pathways. In the insulin-dependent pathway, GLUT4 is activated through the insulin receptor substrate/phosphoinositide 3-kinase/Akt signaling cascade following insulin stimulation.35 In the insulin-independent pathway, muscle contraction induces GLUT4 translocation to the membrane, facilitating glucose uptake.36
In individuals with T2DM, insulin resistance impairs the insulin-dependent pathway; however, the contraction-mediated pathway remains relatively preserved. Previous experimental research demonstrated that GLUT4 mRNA expression in patients with T2DM increased by approximately 66% after 60 minutes of cycling exercise, whereas the control group showed an increase of approximately 60%,37 corresponding to enhanced glucose disposal. These findings suggest that variations in insulin resistance severity and skeletal muscle GLUT4 content play a crucial role in glucose metabolism among individuals with T2DM.
Decreased muscle strength exacerbates insulin resistance by impairing metabolic regulation, accompanied by mitochondrial dysfunction, increased inflammation, and elevated oxidative stress within muscle tissue.25 In individuals with diabetes, the insulin-dependent pathway for glucose uptake into muscles is likely impaired, possibly leading to a weakened relationship between relative handgrip strength and HbA1c. In contrast, the non-diabetic group, with a functional insulin-independent pathway, exhibited a larger effect and significant relationship between muscle strength and glycemic control. This suggests that the impact of muscle strength on glycemic control may have appeared stronger in individuals without diabetes, where the insulin-dependent pathway remains intact. This finding is consistent with the biological link between muscle function and glucose metabolism within this occupational group.
This study focused on automobile manufacturing workers who regularly operate vibration tools. Vibration exposure can reduce grip strength through sensorineural and musculoskeletal impairment that is not directly related to metabolic status, which may weaken the validity of handgrip strength as a pure biomarker of glycemic control in this population.38 Nevertheless, our findings indicate that lower relative handgrip strength was still associated with higher HbA1c levels among vibration-exposed manual workers, suggesting that the inverse relationship between muscle strength and glycemic status persists even in the presence of vibration exposure in grip strength measurements. Because handgrip strength can be assessed easily without the need for blood sampling, it can be considered as a simple functional indicator that is recorded alongside routine measures such as blood pressure and glucose levels during occupational health examinations and may provide additional information on workers’ status.
Maintaining or enhancing muscle strength may be important for preserving physical function and supporting metabolic health. Regular resistance exercise improves insulin sensitivity and enhances GLUT4 expression in skeletal muscle, thereby supporting better glycemic regulation.39 Future research should elucidate the causal relationship between muscle strength decline and glycemic control in high-risk groups such as night-shift workers.
The strengths of this study include its homogeneous sample composition, which helps reduce variability due to work intensity and exposure factors. In occupational settings, confounding factors such as vibration exposure, long working hours, and job-related physical demands may influence muscle strength and metabolic regulation.17,18 This study, conducted within a single industrial sector, helps minimize such heterogeneity and provides insight into the association between relative handgrip strength and HbA1c in this occupational setting. Additionally, the relatively large sample size of 1,823 participants enhanced the statistical power of the analyses. HbA1c was assessed as part of an occupational health examination for virtually all male workers at the same company, which minimizes the likelihood of substantial selection bias within this cohort. Because automobile manufacturing workers are typically engaged in manual labor and often experience long working hours, clinicians may be uncertain whether reduced handgrip strength simply reflects occupational demands; our findings clarified that lower relative handgrip strength remains associated with poorer glycemic profiles within this occupational context. The study findings align with previous domestic and international research.
This study has some limitations. First, due to its cross-sectional design, causal relationships could not be clearly established and reverse causality could not be ruled out; for example, reduced muscle strength may contribute to poorer glycemic control. Therefore, establishing a longitudinal cohort within occupational populations would provide valuable opportunities to examine whether changes in handgrip strength over time are associated with subsequent alterations in HbA1c levels or the onset of type 2 diabetes. Second, data on dietary intake—a major determinant of HbA1c—were not collected in detail and could not be incorporated into the analyses; important aspects such as overall dietary patterns and meal regularity may have acted as unmeasured confounders. Third, some covariates were collected through self-reported questionnaires, which may have introduced recall or reporting bias. Fourth, because data collection was conducted in an operational industrial setting, some workers may not have adhered to the eight-hour fasting period, potentially affecting the reliability of fasting glucose measurements. Finally, because this study exclusively involved male workers from a single occupational group within South Korea, the observed associations between relative handgrip strength and glycemic control may not be directly applicable to women, other occupational groups, or the broader general population. Additionally, although this study focused on a relatively homogeneous group of male automobile manufacturing workers, detailed information on specific job tasks and vibration exposure intensity was limited, and only few participants were engaged in shift work; therefore, we could not meaningfully examine whether these occupational factors affect the association between relative handgrip strength and HbA1c levels. Hence, caution should be exercised in generalizing these results. Although we additionally adjusted for hemoglobin concentration and eGFR to consider major non-glycemic determinants of HbA1c, other factors that can alter RBC turnover or HbA1c independently of glycemia—including unmeasured anemia subtypes, iron or vitamin B12 deficiency, and certain medications—were not assessed and may have led to residual confounding. Further research involving more diverse cohorts will be required to substantiate and extend these findings. Despite these limitations, the study adds value by supporting the association between handgrip strength and glycemic control within a working population whose occupational factors were relatively controlled.
CONCLUSIONS
This study investigated the relationship between relative handgrip strength and HbA1c levels among male automobile manufacturing workers in South Korea. Higher HbA1c levels were significantly associated with lower relative handgrip strength, suggesting that the same pattern observed in the general population persists within this occupational group. Because handgrip strength is a noninvasive and easily measurable indicator, it can be documented alongside routine clinical measures in occupational health examinations and may provide additional information on workers’ functional and metabolic status. In this context, handgrip strength may provide complementary information on workers’ functional and metabolic status when interpreted together with conventional clinical measures.
Abbreviations
B
regression coefficient
BMI
body mass index
CI
confidence interval
CKD-EPI
Chronic Kidney Disease Epidemiology Collaboration
eGFR
estimated glomerular filtration rate
GLUT4
glucose transporter type 4
HbA1c
glycated hemoglobin
KNHANES
Korea National Health and Nutrition Examination Survey
LTPA
leisure-time physical activity
PURE
Prospective Urban Rural Epidemiology
RBC
red blood cell
SD
standard deviation
T2DM
type 2 diabetes mellitus
-
Competing interests
The authors declare that they have no competing interests.
-
Author contributions
Conceptualization: Seo DJ, Kim HC. Data curation: Kim HC. Methodology/formal analysis/validation: Seo DJ, Kim HC. Project administration: Kim HC. Supervision: Kim HC, Leem JH, Park SG. Writing – original draft: Seo DJ. Writing – review & editing: Kim HJ, Kim Y, Mun J, Kim HC, Leem JH, Park SG, Lee DW.
NOTES
SUPPLEMENTARY MATERIAL
Supplementary Table 1.
Association between HbA1c and relative handgrip strength by employment duration.
Supplementary Table 2.
Interaction between employment duration and HbA1c on handgrip strength.
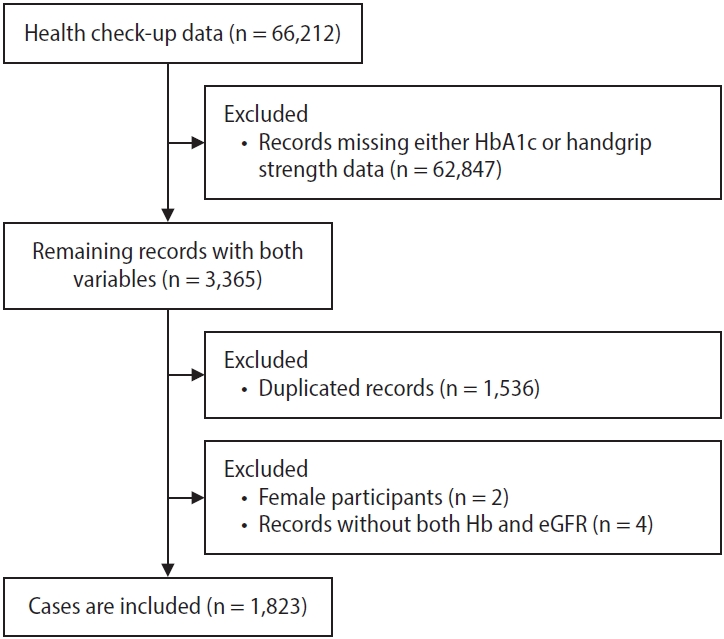
Fig. 2.
Association between glycated hemoglobin (HbA1c) and relative handgrip strength by diabetes status. Model 1: age-adjusted, model 2: fully-adjusted. The circle and square indicate the regression coefficient for Model 1 and Model 2, respectively: dot.
Fig. 3.
Association between glycated hemoglobin (HbA1c) and relative handgrip strength by duration of employment. Fully adjusted; bold indicates p < 0.05. The dot indicates the regression coefficient, and the bar represents the 95% confidence interval for each estimate. DM: diabetes mellitus.
Table 1.
General characteristics of the study population
| Characteristic | Value (n = 1,823) |
|---|---|
| Age (years) | 48.54 ± 7.88 |
| BMI (kg/m2) | 25.17 ± 3.27 |
| Relative grip strength (kg/BMI) | 1.72 ± 0.30 |
| Fasting glucose (mg/dL) | 106.29 ± 25.84 |
| HbA1c (%) | 5.84 ± 0.80 |
| Hb (g/dL) | 15.13 ± 1.03 |
| eGFR (mL/min/1.73 m2) | 101.35 ± 11.61 |
| Employment duration | 20.55 ± 11.30 |
| 0–5 years | 228 (12.5) |
| 6–10 years | 141 (7.7) |
| 11–20 years | 616 (33.8) |
| >20 years | 838 (46.0) |
| Current hypertension | |
| No | 1,431 (78.5) |
| Yes | 392 (21.5) |
| Current dyslipidemia | |
| No | 1,566 (85.9) |
| Yes | 257 (14.1) |
| Current antidiabetic-medication use | |
| No | 1,638 (89.9) |
| Yes | 185 (10.1) |
| Familial diabetes history | |
| No | 1,560 (85.6) |
| Yes | 263 (14.4) |
| Current alcohol use | |
| No | 270 (14.8) |
| Yes | 1,553 (85.2) |
| Diabetic status | |
| Normal | 573 (31.4) |
| Prediabetes | 961 (52.7) |
| T2DM | 289 (15.9) |
| Smoking | |
| Never | 478 (26.2) |
| Former | 618 (33.9) |
| Current | 727 (39.9) |
| Leisure time physical activitya | |
| Low | 608 (33.4) |
| Moderate | 285 (15.6) |
| High | 930 (51.0) |
| Resistance exerciseb | |
| Low | 948 (52.0) |
| Moderate | 471 (25.8) |
| High | 404 (22.2) |
Values are presented as mean±SD or number (%).
BMI: body mass index; HbA1c: glycated hemoglobin; Hb: hemoglobin; eGFR: estimated glomerular filtration rate; T2DM: type 2 diabetes mellitus; SD: standard deviation.
aLeisure-time physical activity was classified according to the World Health Organization physical activity recommendations, combining moderate- and vigorous-intensity activities;
bResistance exercise was classified as follows: low (0 times per week), moderate (1–2 times per week), and high (≥3 times per week).
Table 2.
Association between HbA1c and relative handgrip strength in the study population
| Model 1a | Model 2b | |
|---|---|---|
| Regression coefficientc | −0.069 | −0.060 |
| 95% CI | −0.086 to −0.052 | −0.081 to −0.039 |
| p-value | <0.001 | <0.001 |
HbA1c: glycated hemoglobin; CI: confidence interval.
aModel 1 is adjusted for age;
bModel 2 is adjusted for age, hemoglobin, estimated glomerular filtration rate, current hypertension, current hyperlipidemia, current hypoglycemic–agents use, family diabetes history, smoking, alcohol use, leisure-time physical activity, and resistance exercise;
cRegression coefficients represent the change in relative handgrip strength for each 1% increase in HbA1c.
Table 3.
Association between HbA1c and relative handgrip strength by diabetes status
| Model 1a | Model 2b | |
|---|---|---|
| Normoglycemic (n = 573) | ||
| Regression coefficientc | −0.146 | −0.185 |
| 95% CI | −0.265 to −0.027 | −0.305 to −0.065 |
| p-value | 0.016 | 0.003 |
| Prediabetes (n = 961) | ||
| Regression coefficient | −0.133 | −0.115 |
| 95% CI | −0.197 to −0.069 | −0.180 to −0.050 |
| p-value | <0.001 | <0.001 |
| Diabetes mellitus (n = 289) | ||
| Regression coefficient | −0.026 | −0.023 |
| 95% CI | −0.052 to −0.001 | −0.050 to 0.003 |
| p-value | 0.046 | 0.082 |
HbA1c: glycated hemoglobin; CI: confidence interval.
aModel 1 is adjusted for age;
bModel 2 is adjusted for age, hemoglobin, estimated glomerular filtration rate, current hypertension, current hyperlipidemia, current hypoglycemic–agents use, family diabetes history, smoking, alcohol use, leisure-time physical activity, and resistance exercise;
cRegression coefficients represent the change in relative handgrip strength for each 1% increase in HbA1c.
- 1. Goyal R, Singhal M, Jialal I. Type 2 diabetes. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK513253/. Updated 2023. Accessed November 21, 2025.
- 2. GBD 2021 Diabetes Collaborators. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet 2023;402(10397):203–34.ArticlePubMedPMC
- 3. Wu H, Norton V, Cui K, Zhu B, Bhattacharjee S, Lu YW, et al. Diabetes and its cardiovascular complications: comprehensive network and systematic analyses. Front Cardiovasc Med 2022;9:841928.ArticlePubMedPMC
- 4. Kim JY, Lee J, Moon JH, Park SE, Ko SH, Choi SH, et al. Prevalence, incidence, and metabolic characteristics of young adults with type 2 diabetes mellitus in South Korea (2010-2020). Diabetes Metab J 2025;49(2):172–82.ArticlePubMedPMCPDF
- 5. Park SE, Ko SH, Kim JY, Kim K, Moon JH, Kim NH, et al. Diabetes fact sheets in Korea 2024. Diabetes Metab J 2025;49(1):24–33.ArticlePubMedPMCPDF
- 6. Sherwani SI, Khan HA, Ekhzaimy A, Masood A, Sakharkar MK. Significance of HbA1c test in diagnosis and prognosis of diabetic patients. Biomark Insights 2016;11:95–104.ArticlePubMedPMCPDF
- 7. Dykun I, Kappo N, Kampf J, Babinets O, Janosi RA, Totzeck M, et al. Association of hemoglobin A1c levels with all-cause mortality in patients with coronary artery disease: the Essen Coronary Artery Disease Registry. JACC Adv 2025;4(3):101624.ArticlePubMedPMC
- 8. Eyth E, Zubair M, Naik R. Hemoglobin A1C. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK549816/. Updated 2025. Accessed November 21, 2025.
- 9. Cohen RM, Franco RS, Khera PK, Smith EP, Lindsell CJ, Ciraolo PJ, et al. Red cell life span heterogeneity in hematologically normal people is sufficient to alter HbA1c. Blood 2008;112(10):4284–91.ArticlePubMedPMCPDF
- 10. Sinha N, Mishra TK, Singh T, Gupta N. Effect of iron deficiency anemia on hemoglobin A1c levels. Ann Lab Med 2012;32(1):17–22.ArticlePubMedPMC
- 11. Aydin B, Cansu GB, Ozlu C. Relationship between glycosylated hemoglobin and vitamin B12 deficiency anemia. North Clin Istanb 2022;9(5):459–63.ArticlePubMedPMC
- 12. Bloomgarden Z, Handelsman Y. How does CKD affect HbA1c? J Diabetes 2018;10(4):270.ArticlePubMedPDF
- 13. Tang M, Berg A, Rhee EP, Allegretti AS, Nigwekar S, Karumanchi SA, et al. The impact of carbamylation and anemia on HbA1c's association with renal outcomes in patients with diabetes and chronic kidney disease. Diabetes Care 2023;46(1):130–7.ArticlePubMedPMC
- 14. DeFronzo RA, Tripathy D. Skeletal muscle insulin resistance is the primary defect in type 2 diabetes. Diabetes Care 2009;32(Suppl 2):S157–63.ArticlePubMedPMCPDF
- 15. Leenders M, Verdijk LB, van der Hoeven L, Adam JJ, van Kranenburg J, Nilwik R, et al. Patients with type 2 diabetes show a greater decline in muscle mass, muscle strength, and functional capacity with aging. J Am Med Dir Assoc 2013;14(8):585–92.Article
- 16. Baldi JC, Snowling N. Resistance training improves glycaemic control in obese type 2 diabetic men. Int J Sports Med 2003;24(6):419–23.Article
- 17. Mesinovic J, Zengin A, De Courten B, Ebeling PR, Scott D. Sarcopenia and type 2 diabetes mellitus: a bidirectional relationship. Diabetes Metab Syndr Obes 2019;12:1057–72.ArticlePubMed
- 18. Vaishya R, Misra A, Vaish A, Ursino N, D'Ambrosi R. Hand grip strength as a proposed new vital sign of health: a narrative review of evidences. J Health Popul Nutr 2024;43(1):7.ArticlePubMedPMCPDF
- 19. Choquette S, Bouchard DR, Doyon CY, Senechal M, Brochu M, Dionne IJ. Relative strength as a determinant of mobility in elders 67-84 years of age. a nuage study: nutrition as a determinant of successful aging. J Nutr Health Aging 2010;14(3):190–5.ArticlePubMedPMCPDF
- 20. Jang BN, Nari F, Kim S, Park EC. Association between relative handgrip strength and prediabetes among South Korean adults. PLoS One 2020;15(10):e0240027.ArticlePubMedPMC
- 21. Granic A, Cooper R, Hurst C, Hillman SJ, Dodds RM, Witham MD, et al. Cross-sectional and longitudinal associations between glycaemic measures and grip strength in people without diabetes in the UK Biobank cohort study. Eur Geriatr Med 2025;16(1):67–77.ArticlePubMedPMCPDF
- 22. Leong DP, Teo KK, Rangarajan S, Lopez-Jaramillo P, Avezum A, Orlandini A, et al. Prognostic value of grip strength: findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet 2015;386(9990):266–73.ArticlePubMed
- 23. Son M, Kong JO, Koh SB, Kim J, Harma M. Effects of long working hours and the night shift on severe sleepiness among workers with 12-hour shift systems for 5 to 7 consecutive days in the automobile factories of Korea. J Sleep Res 2008;17(4):385–94.ArticlePubMed
- 24. He X, Xiao B, Wu J, Chen C, Li W, Yan M. Prevalence of work-related musculoskeletal disorders among workers in the automobile manufacturing industry in China: a systematic review and meta-analysis. BMC Public Health 2023;23(1):2042.ArticlePubMedPMCPDF
- 25. Lawman HG, Troiano RP, Perna FM, Wang CY, Fryar CD, Ogden CL. Associations of relative handgrip strength and cardiovascular disease biomarkers in U.S. adults, 2011-2012. Am J Prev Med 2016;50(6):677–83.ArticlePubMedPMC
- 26. ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, et al. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes—2023. Diabetes Care 2023;46(Suppl 1):S19–40.ArticlePubMedPMC
- 27. Lopez-Bueno R, Andersen LL, Koyanagi A, Nunez-Cortes R, Calatayud J, Casana J, et al. Thresholds of handgrip strength for all-cause, cancer, and cardiovascular mortality: a systematic review with dose-response meta-analysis. Ageing Res Rev 2022;82:101778.ArticlePubMed
- 28. Carson RG. Get a grip: individual variations in grip strength are a marker of brain health. Neurobiol Aging 2018;71:189–222.ArticlePubMed
- 29. Choe H, Sung H, Kim GH, Lee O, Moon HY, Kim YS. Associations between grip strength and glycemic control in type 2 diabetes mellitus: an analysis of data from the 2014-2019 Korea National Health and Nutrition Examination Survey. Epidemiol Health 2021;43:e2021080.ArticlePubMedPMC
- 30. Kunutsor SK, Isiozor NM, Khan H, Laukkanen JA. Handgrip strength: a risk indicator for type 2 diabetes: systematic review and meta-analysis of observational cohort studies. Diabetes Metab Res Rev 2021;37(2):e3365.ArticlePubMedPDF
- 31. Kim M, Won CW, Kim M. Muscular grip strength normative values for a Korean population from the Korea National Health and Nutrition Examination Survey, 2014-2015. PLoS One 2018;13(8):e0201275.ArticlePubMedPMC
- 32. Bruce CR, Anderson MJ, Carey AL, Newman DG, Bonen A, Kriketos AD, et al. Muscle oxidative capacity is a better predictor of insulin sensitivity than lipid status. J Clin Endocrinol Metab 2003;88(11):5444–51.ArticlePubMedPDF
- 33. DeFronzo RA. Pathogenesis of type 2 diabetes mellitus. Med Clin North Am 2004;88(4):787–835.ArticlePubMed
- 34. Richter EA, Hargreaves M. Exercise, GLUT4, and skeletal muscle glucose uptake. Physiol Rev 2013;93(3):993–1017.ArticlePubMed
- 35. Mackenzie RW, Elliott BT. Akt/PKB activation and insulin signaling: a novel insulin signaling pathway in the treatment of type 2 diabetes. Diabetes Metab Syndr Obes 2014;7:55–64.ArticlePubMedPMC
- 36. Lauritzen HP. Insulin- and contraction-induced glucose transporter 4 traffic in muscle: insights from a novel imaging approach. Exerc Sport Sci Rev 2013;41(2):77–86.ArticlePubMedPMC
- 37. Hussey SE, McGee SL, Garnham A, McConell GK, Hargreaves M. Exercise increases skeletal muscle GLUT4 gene expression in patients with type 2 diabetes. Diabetes Obes Metab 2012;14(8):768–71.ArticlePubMed
- 38. Dong RG, Wu JZ, Xu XS, Welcome DE, Krajnak K. A review of hand-arm vibration studies conducted by US NIOSH since 2000. Vibration 2021;4(2):482–528.ArticlePubMedPMC
- 39. Holten MK, Zacho M, Gaster M, Juel C, Wojtaszewski JF, Dela F. Strength training increases insulin-mediated glucose uptake, GLUT4 content, and insulin signaling in skeletal muscle in patients with type 2 diabetes. Diabetes 2004;53(2):294–305.ArticlePDF
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteAssociation between relative handgrip strength and glycemic control among male automobile manufacturing workers using vibration tools in South Korea
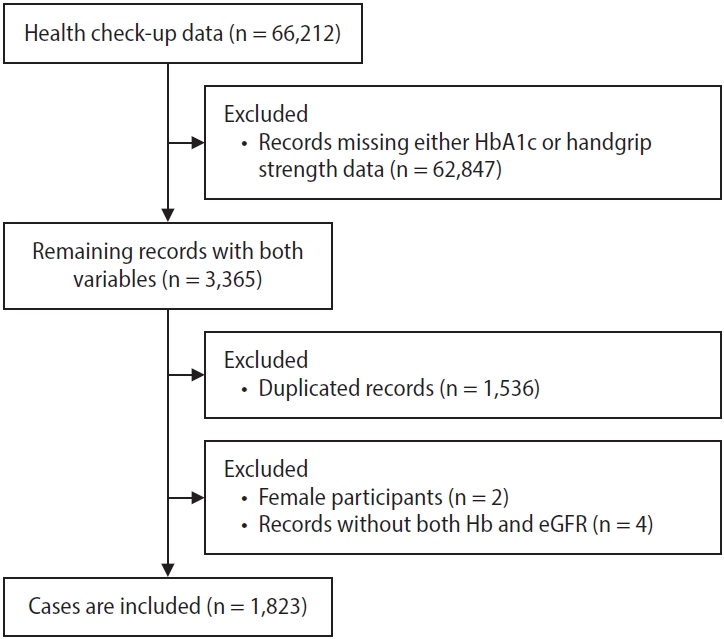
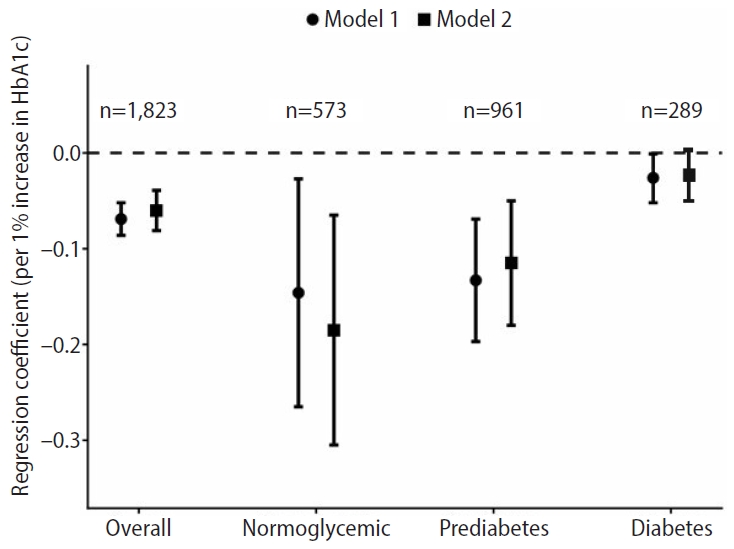
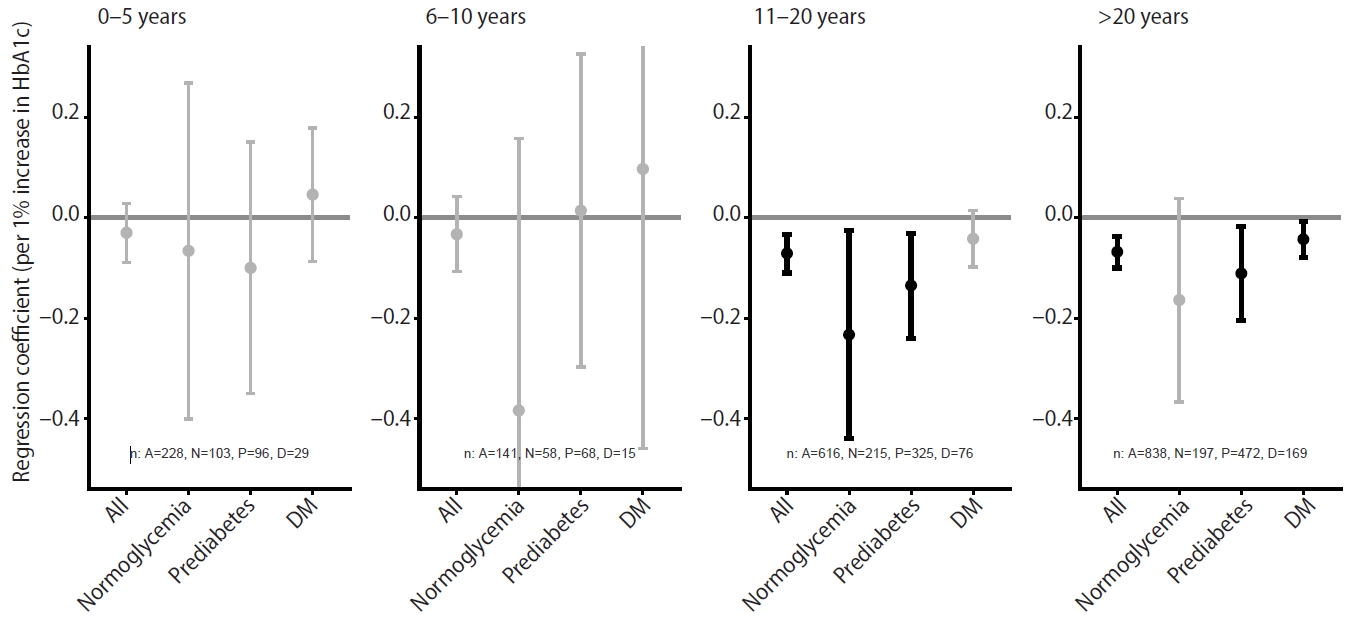
Fig. 1. Flowchart of study participants. HbA1c: glycated hemoglobin.
Fig. 2. Association between glycated hemoglobin (HbA1c) and relative handgrip strength by diabetes status. Model 1: age-adjusted, model 2: fully-adjusted. The circle and square indicate the regression coefficient for Model 1 and Model 2, respectively: dot.
Fig. 3. Association between glycated hemoglobin (HbA1c) and relative handgrip strength by duration of employment. Fully adjusted; bold indicates p < 0.05. The dot indicates the regression coefficient, and the bar represents the 95% confidence interval for each estimate. DM: diabetes mellitus.
Fig. 1.
Fig. 2.
Fig. 3.
Association between relative handgrip strength and glycemic control among male automobile manufacturing workers using vibration tools in South Korea
| Characteristic | Value (n = 1,823) |
|---|---|
| Age (years) | 48.54 ± 7.88 |
| BMI (kg/m2) | 25.17 ± 3.27 |
| Relative grip strength (kg/BMI) | 1.72 ± 0.30 |
| Fasting glucose (mg/dL) | 106.29 ± 25.84 |
| HbA1c (%) | 5.84 ± 0.80 |
| Hb (g/dL) | 15.13 ± 1.03 |
| eGFR (mL/min/1.73 m2) | 101.35 ± 11.61 |
| Employment duration | 20.55 ± 11.30 |
| 0–5 years | 228 (12.5) |
| 6–10 years | 141 (7.7) |
| 11–20 years | 616 (33.8) |
| >20 years | 838 (46.0) |
| Current hypertension | |
| No | 1,431 (78.5) |
| Yes | 392 (21.5) |
| Current dyslipidemia | |
| No | 1,566 (85.9) |
| Yes | 257 (14.1) |
| Current antidiabetic-medication use | |
| No | 1,638 (89.9) |
| Yes | 185 (10.1) |
| Familial diabetes history | |
| No | 1,560 (85.6) |
| Yes | 263 (14.4) |
| Current alcohol use | |
| No | 270 (14.8) |
| Yes | 1,553 (85.2) |
| Diabetic status | |
| Normal | 573 (31.4) |
| Prediabetes | 961 (52.7) |
| T2DM | 289 (15.9) |
| Smoking | |
| Never | 478 (26.2) |
| Former | 618 (33.9) |
| Current | 727 (39.9) |
| Leisure time physical activity |
|
| Low | 608 (33.4) |
| Moderate | 285 (15.6) |
| High | 930 (51.0) |
| Resistance exercise |
|
| Low | 948 (52.0) |
| Moderate | 471 (25.8) |
| High | 404 (22.2) |
| Model 1 |
Model 2 |
|
|---|---|---|
| Regression coefficient |
−0.069 | −0.060 |
| 95% CI | −0.086 to −0.052 | −0.081 to −0.039 |
| p-value | <0.001 | <0.001 |
| Model 1 |
Model 2 |
|
|---|---|---|
| Normoglycemic (n = 573) | ||
| Regression coefficient |
−0.146 | −0.185 |
| 95% CI | −0.265 to −0.027 | −0.305 to −0.065 |
| p-value | 0.016 | 0.003 |
| Prediabetes (n = 961) | ||
| Regression coefficient | −0.133 | −0.115 |
| 95% CI | −0.197 to −0.069 | −0.180 to −0.050 |
| p-value | <0.001 | <0.001 |
| Diabetes mellitus (n = 289) | ||
| Regression coefficient | −0.026 | −0.023 |
| 95% CI | −0.052 to −0.001 | −0.050 to 0.003 |
| p-value | 0.046 | 0.082 |
Table 1. General characteristics of the study population
Values are presented as mean±SD or number (%). BMI: body mass index; HbA1c: glycated hemoglobin; Hb: hemoglobin; eGFR: estimated glomerular filtration rate; T2DM: type 2 diabetes mellitus; SD: standard deviation. Leisure-time physical activity was classified according to the World Health Organization physical activity recommendations, combining moderate- and vigorous-intensity activities; Resistance exercise was classified as follows: low (0 times per week), moderate (1–2 times per week), and high (≥3 times per week).
Table 2. Association between HbA1c and relative handgrip strength in the study population
HbA1c: glycated hemoglobin; CI: confidence interval. Model 1 is adjusted for age; Model 2 is adjusted for age, hemoglobin, estimated glomerular filtration rate, current hypertension, current hyperlipidemia, current hypoglycemic–agents use, family diabetes history, smoking, alcohol use, leisure-time physical activity, and resistance exercise; Regression coefficients represent the change in relative handgrip strength for each 1% increase in HbA1c.
Table 3. Association between HbA1c and relative handgrip strength by diabetes status
HbA1c: glycated hemoglobin; CI: confidence interval. Model 1 is adjusted for age; Model 2 is adjusted for age, hemoglobin, estimated glomerular filtration rate, current hypertension, current hyperlipidemia, current hypoglycemic–agents use, family diabetes history, smoking, alcohol use, leisure-time physical activity, and resistance exercise; Regression coefficients represent the change in relative handgrip strength for each 1% increase in HbA1c.

