
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 37; 2025 > Article
-
[Special Collection] Psychosocial stress measurement tools
Special Article Workplace Violence (KWVS®13): scale development and validation in the Korean context -
Da-Yee Jeung1
 , Hyoung Ryoul Kim2, Hansoo Song3, Inah Kim4, Jin-Ha Yoon5, Sang-Baek Koh6, Sung-Soo Oh7, Hee-Tae Kang8, Dae-Sung Hyun9, Chunhui Suh10, Sei-Jin Chang6,*
, Hyoung Ryoul Kim2, Hansoo Song3, Inah Kim4, Jin-Ha Yoon5, Sang-Baek Koh6, Sung-Soo Oh7, Hee-Tae Kang8, Dae-Sung Hyun9, Chunhui Suh10, Sei-Jin Chang6,* -
Annals of Occupational and Environmental Medicine 2025;37:e14.
DOI: https://doi.org/10.35371/aoem.2025.37.e14
Published online: May 7, 2025
1Department of Dental Hygiene, Hanyang Women's University, Seoul, Korea
2Department of Occupational and Environmental Medicine, Seoul St. Mary's Hospital, Seoul, Korea
3Department of Occupational and Environmental Medicine, Chosun University Hospital, Gwangju, Korea
4Department of Occupational and Environmental Medicine, Hanyang University College of Medicine, Seoul, Korea
5The Institute for Occupational Health, Yonsei University College of Medicine, Seoul, Korea
6Department of Preventive Medicine, Institute of Occupational and Environmental Medicine, Yonsei University Wonju College of Medicine, Wonju, Korea
7Department of Occupational and Environmental Medicine, Institute of Occupational and Environmental Medicine, Wonju SeveranceChristian Hospital, Yonsei University Wonju College of Medicine, Wonju, Korea
8Department of Occupational and Environmental Medicine, Wonju Severance Christian Hospital, Yonsei University Wonju College of Medicine, Wonju, Korea
9Department of Non-benefits Management, National Health Insurance Service, Wonju, Korea
10Department of Occupational and Environmental Medicine, Institute of Environmental and Occupational Medicine, Inje University Pusan Paik Hospital, Busan, Korea
- *Corresponding author: Sei-Jin Chang Department of Preventive Medicine, Institute of Occupational and Environmental Medicine,Yonsei University Wonju College of Medicine, 20 Ilsan-ro, Wonju 26426, Korea E-mail: chang0343@yonsei.ac.kr
• Received: February 11, 2025 • Revised: April 19, 2025 • Accepted: April 21, 2025
© 2025 Korean Society of Occupational & Environmental Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background Workplace violence refers to any act or threat of physical violence, verbal abuse, harassment, intimidation, bullying, mobbing, or other aggressive and disruptive behaviors that occur at work. This study aims to develop and validate a revision of the Korean Workplace Violence Scale (KWVS®13), based on the first edition of the Korean Workplace Violence Scale (KWVS-24), and to provide practical applications and guidelines for the Korean workplace environment.
-
Methods The revised KWVS®13 was developed by restructuring the 24-item KWVS through a review process involving eight experts. To validate the reliability and validity of KWVS®13, a self-administered survey comprising KWVS®13, burnout, and depression scales was conducted among 359 service industry workers. KWVS®13 was reclassified, and its reliability and validity were assessed. Receiver operating characteristic curve analysis was performed to establish sex-specific cutoff values (normal vs. risk) of the scale.
-
Results KWVS®13 consists of 13 items across four subscales: “psychological and sexual violence from customers” (4 items), “psychological and sexual violence from supervisors or coworkers” (4 items), “physical assault from customers, supervisors, or coworkers” (2 items), and “organizational protective system for workplace violence” (3 items). We found that KWVS®13 shows relatively good validity (content validity ratio for content validity: 0.888; success rate of item convergent and discriminant validity: 100%, and significant correlation coefficient with burnout (r = 0.115–0.83, p < 0.05) and depression (r = 0.098–0.348, p < 0.05) with the exception of Organizational Violence Protection System for Workplace Violence) and reliability (Cronbach’s alpha: 0.827–0.860). The reference values for determining risk groups according to the intensity of exposure to workplace violence are presented separately by sex.
-
Conclusions KWVS®13 is a robust and useful measurement tool to objectively and quantitatively assess the intensity and magnitude of workplace violence. It incorporates important considerations for workplace violence assessment and provides a reliable framework for evaluating workplace violence in various professional settings.
BACKGROUND
Workplace violence refers to any act or threat of physical violence, verbal abuse, harassment, intimidation, bullying, or other aggressive and disruptive behavior that occurs in the workplace.1 It can range from verbal abuse to physical assault and may target all types of employees, customers, or others in a work environment. Workplace violence can affect any occupation and has consequences ranging from psychological problems to physical injuries or even death.2
The prevalence of workplace violence varies greatly by occupation and region. According to a 2022 International Labour Organization–Lloyd’s Register Foundation-Gallup survey, 23% of employees globally have experienced some form of violence or harassment at work.3 The World Health Organization estimates that between 8% and 38% of healthcare workers have experienced physical violence at some point in their careers, and up to 62% of healthcare workers have experienced workplace violence, with verbal abuse being the most common form.4 In South Korea, workplace violence varies by occupation and has a higher prevalence in certain occupational sectors. Lee et al.5 analyzed data from the 2011 Korean Labor Conditions Survey and found that service workers reported a higher incidence of workplace violence than those in other occupations. Hong et al.6 reported that sales workers experienced more sexual harassment in the workplace than white-collar workers do. According to data from the 5th Survey of Korean Workers, 5.6% of workers experienced violence in the workplace, with verbal abuse being the most common form (4.9%). Among service industry workers, the prevalence was 9.0%.7 According to a survey conducted by a non-governmental organization, about 15.3% of South Korean workers have experienced physical and verbal abuse at work, so-called “bullying.”8
Workplace violence has been shown to impact employees’ physical and mental health significantly. Exposure to workplace violence increases the risk of post-traumatic stress disorder (PTSD) symptoms, chronic pain, musculoskeletal disorders, hypertension, and other cardiovascular diseases.9 Moreover, workplace violence contributes to burnout,10 increased absenteeism, decreased productivity, and increased healthcare costs.1 Although workplace violence affects almost all occupations, it is apparent that violence in healthcare settings manifests a significant threat to public health.11 The healthcare and social service industries have the greatest rates of workplace violence injuries.12 Previous studies revealed that victims of workplace violence are more prone to experience demoralization, depression, and loss of self-esteem, as well as symptoms of PTSD such as insomnia, irritability, difficulty concentrating, reliving of trauma, and emotional distress.13-15
Measuring workplace violence is a complex process that requires the assessment of its different forms, causes, and consequences. An effective measurement tool for workplace violence is also needed to assess the incidents or perceptions of workplace violence, evaluating the frequency, nature, and impact of violent behaviors in the workplace, as well as types of violence such as physical violence, verbal abuse, threats, and harassment.16
Over the past 30 years, several measurement tools have been developed to measure workplace violence. Whittington and Wykes17 developed the Violent Incident Form to measure violent events, including their nature and consequences in the health and service sectors. The Workplace Aggression Research Questionnaire by Neuman and Baron18 was designed to assess workplace violence by focusing on physical and verbal aggression directed at employees by superiors, coworkers, or clients. Arnetz and Arnetz19 used the Violence Assessment Questionnaire to measure the frequency of workplace violence incidents (e.g., physical aggression and verbal threats) and their emotional impact on workers. Kelloway et al.20 developed the Workplace Violence Questionnaire to assess physical violence, verbal abuse, bullying, and sexual harassment in the workplace, incorporating both frequency and severity dimensions. The Negative Acts Questionnaire–Revised21 is widely used to assess workplace bullying. It measures exposure to negative behaviors, such as personal bullying, work-related harassment, and physical threats. The Occupational Violence Questionnaire22 was developed to measure violence faced by workers in various occupational sectors, including verbal abuse, threats, and physical violence. In South Korea, only a few tools have been developed to assess workplace violence across different professions (e.g., the Workplace Violence Scale for Clinical Dental Hygienists and the 12-item Perception of Aggression Scale).23,24
The first version of the ‘Korean Workplace Violence Scale (KWVS-24)’ was designed to evaluate the intensity of workplace violence considering the unique characteristics of Korea's organizational culture and service industry. It consisted of 24 items and was formulated through an in-depth literature review, focus group interviews, and a nationwide survey.25,26 However, the questions need to be revised because the work environment and organizational climate have rapidly changed, and some items overlapped. This study aims to revise existing workplace violence measurement tools, to reflect these societal changes. Several studies conducted using KWVS-24, as well as Delphi analysis to develop the revision, have shown that some items are redundant, some items may be included in the comprehensive questions, and others are difficult to apply to specialized occupations (e.g., non-face-to-face workers such as white-collar workers and call center workers). Over time, the authors have gathered diverse feedback regarding improvements to KWVS-24.
The purpose of this study is to develop and validate a revision of KWVS®13, based on the first edition of the Korean Workplace Violence Scale (KWVS-24), and to provide practical applications and guidelines for the Korean workplace environment.
METHODS
We conducted a literature review and expert consultations to refine the initial version and validate its reliability. To develop a draft of the revised KWVS, we identified the items through research team workshops, the Delphi method, and advisory meetings. The eight researchers who participated in the Delphi survey are experts who have been conducting research in the field of psychometry for more than a decade, to develop psychosocial measurement tools. Their majors are occupational medicine, preventive medicine, medical sociology, health psychology, and dental hygiene. KWVS®13 was elaborated through a workshop in which 12 investigators and advisory committee members participated. The group included experts from the labor industry, companies, government, and university institutions. A detailed procedure of this study is shown in Fig. 1.
Using the Delphi method, eight experts evaluated whether each item should be retained, revised, or excluded. Positive responses, including retaining or revising an item, were used to calculate the content validity ratio (CVR) for each item.27 Lawshe27 recommended that items with a CVR of 0.75 or higher, based on evaluations from eight panelists, could be regarded as evidence of satisfactory content validity. The CVR was calculated using Lawshe’s formula. Using this validation process, we developed the revised draft, named KWVS®13.
To validate KWVS®13, we conducted a survey targeting 359 service workers (114 males and 245 females). The survey included demographics (sex, age, and occupation), KWVS®13, and measures for depression (using the Patient Health Questionnaire-9) and burnout (using the emotional exhaustion subscale of the Maslach Burnout Inventory).28,29 Participants were sampled from various service industry sectors, representing various levels of emotional labor, and data were collected using administered face-to-face surveys.
Exploratory factor analysis (EFA) was performed to examine the factor structure of the 13 items. Convergent and discriminant validity were evaluated using a Multitrait-Multimethod Matrix to induce correlation coefficients.30 Criterion validity was addressed using Pearson’s correlation analysis to analyze the relationship between KWVS®13 subscales, with depression and burnout as outcome variables. Cronbach’s alpha was calculated to evaluate the internal consistency (reliability). Finally, receiver operating characteristic (ROC) analysis was conducted to establish sex-specific cutoff values (normal vs. risk) for the scale. A p < 0.05 was considered significant for all statistical analyses. For CVR of content validity, a value of 0.75 or higher was considered meaningful. Data were analyzed using IBM SPSS Statistics version 23.0 (IBM Corp., Armonk, NY, USA).
RESULTS
The first edition of KWVS-24 consisted of four subscales and 24 items, measured using a 4-point Likert scale. In this study, we developed the revised version of KWVS-24 (KWVS®13) through a four-step validation process.
The draft version of KWVS®13, refined through the Delphi method and open workshops, is shown in Fig. 2. The Korean version is available in the Supplementary Data 1. Based on the CVR of the initial version of KWVS-24, 13 items were selected. The CVR calculated using Lawshe’s Content Validity Index for KWVS®13 was 0.88.
To confirm validity and reliability, a self-administered survey (n = 359) was performed. Regarding the sex distribution of participants, 114 were males (31.8%) and 245 were females (68.2%). The average age of respondents was 36.9 years. Notably, participants in their 20s and 30s made up 65% of the total sample, indicating a higher proportion of younger workers. Regarding occupational status, the largest group consisted of healthcare workers (29.4%). This was followed by administrative/public service workers (20.9%), call center agents (20.6%), retail and food service workers (10.3%), and police/firefighters (7.0%).
Factorial validity
EFA from the survey dataset was performed to confirm the construct validity of KWVS®13. As a result of the principal component factor analysis of the 13 items proposed for the draft version of KWVS®13, they were initially grouped into three factors, with a total variance of 67.72. Factor 1 was grouped under “psychological and sexual violence from customers, supervisors, or coworkers.” However, the authors agreed that these items should be measured separately because there could be differences between violence from customers and violence from supervisors or coworkers. Factors 2 and 3 were therefore reclassified into “physical assault from customers, supervisors, or coworkers” and “organizational protective system for workplace violence,” respectively. Finally, the 13-item KWVS®13 was reclassified into four subscales (Table 1).
KWVS®13 consists of 13 items in four subscales: “psychological and sexual violence from customers” (4 items), “psychological and sexual violence from supervisors or coworkers” (4 items), “physical assault from customers, supervisors, or coworkers” (2 items), and “organizational protective system for workplace violence” (3 items). All items were scored on a 4-point (1-2-3-4) Likert scale (some items were reverse-scored on a 4-3-2-1 Likert scale).
Convergent and discriminant validity
A Multitrait-Multimethod Matrix analysis was performed to evaluate convergent and discriminant validity between each item and the pre-conceptualized subscale of KWVS®13. Convergent validity was considered acceptable when the correlation between each item and its corresponding factor was at least 0.40. Discriminant validity was obtained when the correlation between each item and its corresponding subscale was greater than its correlation with unrelated subscales. We calculated the success rates of convergent and discriminant validity using the percentage of successful tests out of the total number of tests.
The results showed that convergent and discriminant validity were acceptable for all four subscales, with correlation coefficients (r) above 0.738 and 0.588, respectively. Additionally, for all the subscales, the success rates for item convergent and discriminant validity were 100% (Table 2).
Correlation analysis was performed between the four subscales and the outcome variables burnout and depression to assess the criterion validity of KWVS®13. The results indicate that all four subscales of KWVS®13 showed significant positive correlations with burnout (r = 0.115–0.83, p < 0.05) and depression (r = 0.098–0.348, p < 0.05), with the exception of the Organizational Violence Protection System for Workplace Violence subscale (Table 3).
Cronbach’s alpha was calculated to evaluate the reliability of KWVS®13. As shown in Table 4, Cronbach’s alpha for the four subscales ranged from 0.827 to 0.860.
For the user guidelines, the reference values for determining risk groups according to the intensity of exposure to workplace violence were presented by sex (Table 5). Sex-specific reference values were proposed based on the results of the ROC analysis of depression collected from the survey. The sex-specific cutoff values were obtained based on the maximum value of the area under the ROC curve. These cutoff points were applied to present the sex-specific reference values for each subscale (Table 5).
DISCUSSION
Workplace violence negatively impacts the productivity of organizations as a result of reduced job satisfaction and poor performance capacity and can negatively impact employees' achievement of their goals by decreasing their effectiveness and efficiency.31,32 It has been documented that when organizations experience extreme violence in the workplace, they are deprived of their competitive advantage because the affected workers may not be in a position to perform as effectively as expected.
Over the past few decades, most workplace violence measures have focused on observing the frequency, types, and responses to violence. Currently, very little research has been conducted on organizational policies addressing workplace violence. Prevention strategies should focus on equipping healthcare workers with skills to mitigate potentially violent situations, with the support of organizational policies against aggression. Recent studies highlight that training in communication and relaxation techniques, along with regular psychological support, can be useful in reducing the psychological problems of workplace violence.33 Currently, no standardized model exists for measuring and evaluating workplace violence. Many conventional scales are complex and multidimensional, often neglecting to account for social and cultural differences in the current situation or context. However, access to mental health support and workplace policies that address workplace violence significantly mitigate the impact of workplace violence on employee health. Researchers should focus on the importance of workplace violence scales in measuring and evaluating workplace violence in various professional, work, environmental, and sociocultural contexts.
However, there has been little interest in improving workplace violence. Strong collaborative efforts, support, and commitment from both employers and employees are required to protect them. These data can be used to develop appropriate measurement tools to identify the causes, facts, and magnitude of workplace violence and to suggest strategies to reduce the risk of workplace violence at the individual and organizational levels.
Some contextual factors are needed to develop measures of workplace violence, including the type, frequency, workplace environment, and cultural diversity, as it can vary widely across occupations (e.g., service vs. healthcare vs. education sectors) and work environment.34 Research suggests that the negative effects of workplace violence, such as acute trauma and emotional exhaustion, can be minimized when effectively managed by organizations through collaborative protection systems. Sufficient organizational support is less likely to increase employees’ mental and psychological problems. Studies have shown that organizations that provide strong support systems for their employees can reduce workplace violence and its harmful effects. Organizational support can also reduce aggression by creating a positive work environment that discourages violent behavior. Supportive practices, such as conflict resolution training, clear anti-violence policies, and strong leadership, can reduce the likelihood of violent incidents.35 These systems ensure a safer and healthier environment, improve employee well-being, and foster a culture of respect and responsibility.36,37 Nonetheless, little attention has been paid to the improvement of workplace violence. Both employers and employees must collaborate, support, and commit to protecting themselves, for example, through the development of an appropriate measurement tool for workplace violence.
In this study, we propose KWVS®13, a measurement tool that captures workplace violence and reflects the unique characteristics of Korean organizational culture. Respondents were asked about the frequency and nature of workplace violence they experienced over the past year. The 1-year recall period was selected as workers exposed to violent behavior can typically remember incidents from the previous year.16 It also aligns with common assessment intervals used in other longitudinal studies of workplace violence.38
The revision seeks to enhance usability by reducing the number of items, redefining the general and comprehensive concepts of workplace violence. We preserved eight and modified three of the 24 items. Thirteen items of the subscale of ‘organizational protective System for workplace violence’ were removed because some items (12, 13, 14, and 15) overlapped with item 11, and some items (17, 18, 19, 20, 21, 22, and 24) were included in the comprehensive question of item 16. The revised process of KWVS®13 is presented in the Supplementary Data 2.
The concept of the workplace violence subscales of KWVS®13 is as follows: “psychological and sexual violence from customers” assesses the level of exposure to and experience of mental and sexual violence from clients. “Psychological and sexual violence from supervisors or coworkers” evaluates the level of exposure to and experience of mental and sexual violence from coworkers or supervisors in the workplace. “Physical assault by customers, supervisors, or coworkers” evaluates the level of exposure or experience of physical violence against customers or in the workplace. Finally, the Organizational Violence Protection System for Workplace Violence assesses the degree to which behavioral guidelines and safeguards are systematically in place in the workplace against various forms of violence from bosses, colleagues, and customers.
KWVS®13 was developed to assess the intensity of workplace violence of all workers over a one-year recall period. Scores are evaluated by summing the responses for each item on a subscale. The higher the score, the higher the exposure to workplace violence. However, it is not recommended that the four subscales be added to evaluate overall workplace violence. To account for sex differences, we suggest different reference values for males and females because the level of exposure and awareness of workplace violence varies by sex.39,40 Sex-specific reference values were based on the results of the ROC analysis of depression scores. These findings are provisional and future studies should refine and validate them further using representative national samples.
In the present study, it was found that KWVS®13 is a standardized measurement tool derived from reliability and validity analysis covering all workers, which can quantitatively evaluate workplace violence intensity. In correlation analyses to confirm the relationship of four subscales to the gold standards such as depression and burnout, “psychological and sexual violence from customers or supervisors/coworkers” were more greatly associated with depression and burnout than “physical violence from customers or supervisors/coworkers.” These differences suggest that psychological and sexual violence is more frequent than physical violence, and that the “organizational protective system for workplace violence” does not have a significant impact on psychosocial unhealth such as depression or burnout, compared with exposure to violence. Nevertheless, the “organizational protective system” is significant in that it can reduce workers’ exposure to workplace violence and its consequences.
KWVS®13 is a measurement tool that can objectively evaluate the intensity of workplace violence experienced from customers, supervisors, and coworkers at a geometric level. KWVS®13 also reflects that the intensity of workplace violence differs by sex and includes reference values for males and females.
Despite these strengths, this study had some limitations. The participants who took part in validating the reliability and validity of the tool were from various service industries. Therefore, the generalizability of these findings to primary industries or the manufacturing sectors cannot be confirmed. Further validation studies targeting various occupations are still required.
CONCLUSIONS
KWVS®13 has proved to be a useful measurement tool for objectively and quantitatively assessing the intensity and magnitude of workplace violence. Its development incorporates key considerations essential to developing an effective tool for measuring workplace violence. We found that KWVS®13 shows relatively good validity and reliability, making it a strong and standardized measurement tool that improves on the original KWVS-24. Further research is needed to confirm its validity and reliability and to elucidate the causal relationships between workplace violence and various health outcomes (physical, mental, and occupational).
Abbreviations
AUC
area under the receiver operating characteristic curve
CVR
content validity ratio
EFA
exploratory factor analysis
KWVS
Korean Workplace Violence Scale
PTSD
post-traumatic stress disorder
ROC
receiver operating characteristic
-
Funding
This study was supported by Occupational Safety and Health Research Institute (2018-OSHRI-790).
-
Competing interests
Hyoung Ryoul Kim, Hansoo Song, Inah Kim, Jin-Ha Yoon, Sang-Baek Koh, Sung-Soo Oh, and Chunhui Suh contributing editors of the Annals of Occupational and Environmental Medicine, were not involved in the editorial evaluation or decision to publish this article. All remaining authors have declared no conflicts of interest.
-
Author contributions
Conceptualization: Chang SJ. Data curation: Hyun DS, Jeung DY. Formal analysis: Kim HR, Song H, Kim I, Yoon JH. Investigation: Kim I, Koh SB. Methodology: Oh SS, Kang HT, Suh C. Validation: Jeung DY, Hyun DS. Writing - original draft: Jeung DY. Writing - review & editing: Chang SJ, Jeung DY.
NOTES
SUPPLEMENTARY MATERIAL
Supplementary Data 1.
Korean Workplace Violence Scale: KWVS®13.
Supplementary Data 2.
Final revision of items from KWVS-24 to KWVS®13.


Table 1.
Results of factor analysis for KWVS®13
Table 2.
Convergent and discriminant validity of four subscales and items of KWVS®13
Table 3.
Correlations between four subscales of KWVS®13, burnout and depression
Table 4.
Cronbach’s alphas for four subscales of KWVS®13
Table 5.
Sex-specific cutoff values and reference values for four subscales of KWVS®13
- 1. Occupational Safety and Health Administration. Workplace Violence in Healthcare: Understanding the Challenge. Washington, DC: Occupational Safety and Health Administration; 2015.
- 2. National Institute for Occupational Safety and Health (NIOSH). About workplace violence. https://www.cdc.gov/niosh/violence/about/index.html. Updated 2024. Accessed January 20, 2025.
- 3. Gallup. Are you addressing psychosocial risks at your workplace? https://gallup.com/workplace/470585/addressing-psychosocial-risks-workplace.aspx. Updated May 22, 2024. Accessed May 15, 2025.
- 4. World Health Organization. Preventing violence against health workers. https://www.who.int/activities/preventing-violence-against-health-workers. Updated 2022. Accessed January 20, 2025.
- 5. Lee HE, Kim HR, Park JS. Work-related risk factors for workplace violence among Korean employees. J Occup Health 2014;56(1):12–20.ArticlePubMedPDF
- 6. Hong K, Lee KM, Jang SN. Violence experience among wage workers in the workplace and related factors in Korea. Health Soc Welf Rev 2019;39(3):506–34.Article
- 7. Kim HR. Associations between workplace violence, mental health, and physical health among Korean workers: the fifth Korean working conditions survey. Workplace Health Saf 2022;70(3):161–72.ArticlePubMedPDF
- 8. The Korea Herald. Battling ‘gapjil’: the quest to tame the tyrants among us. https://m.koreaherald.com/article/3365614. Updated December 22, 2024. Accessed January 20, 2025..
- 9. Kivimaki M, Steptoe A. Effects of stress on the development and progression of cardiovascular disease. Nat Rev Cardiol 2018;15(4):215–29.ArticlePubMedPDF
- 10. Maslach C, Leiter MP. Understanding the burnout experience: recent research and its implications for psychiatry. World Psychiatry 2016;15(2):103–11.ArticlePubMedPMC
- 11. Lim MC, Jeffree MS, Saupin SS, Giloi N, Lukman KA. Workplace violence in healthcare settings: the risk factors, implications and collaborative preventive measures. Ann Med Surg (Lond) 2022;78:103727.ArticlePubMedPMC
- 12. U.S. Bureau of Labour Statistics (USBLS). Workplace violence in healthcare 2018. https://www.bls.gov/iif/factsheets/workplace-violence-healthcare-2018.htm. Updated 2020. Accessed February 14, 2022..
- 13. Stathopoulou HG. Violence and aggression towards health care professionals. Health Sci J 2007;1(2):1–7.
- 14. Zafar W, Siddiqui E, Ejaz K, Shehzad MU, Khan UR, Jamali S, et al. Health care personnel and workplace violence in the emergency departments of a volatile metropolis: results from Karachi, Pakistan. J Emerg Med 2013;45(5):761–72.ArticlePubMedPMC
- 15. Zhao S, Liu H, Ma H, Jiao M, Li Y, Hao Y, et al. Coping with workplace violence in healthcare settings: social support and strategies. Int J Environ Res Public Health 2015;12(11):14429–44.ArticlePubMedPMC
- 16. Magnavita N, Larese Filon F, Giorgi G, Meraglia I, Chirico F. Assessing workplace violence: methodological considerations. Med Lav 2024;115(1):e2024003.ArticlePubMedPMCPDF
- 17. Whittington R, Wykes T. Violence in psychiatric hospitals: are certain staff prone to being assaulted? J Adv Nurs 1994;19(2):219–25.ArticlePubMed
- 18. Neuman JH, Baron RA. Workplace violence and workplace aggression: evidence concerning specific forms, potential causes, and preferred targets. J Manag 1998;24(3):391–419.ArticlePDF
- 19. Arnetz JE, Arnetz BB. Violence towards health care staff and possible effects on the quality of patient care. Soc Sci Med 2001;52(3):417–27.ArticlePubMed
- 20. Kelloway EK, Barling J, Hurrell JJ Jr. Handbook of Workplace Violence. Thousand Oaks, CA: Sage Publication; 2006.Article
- 21. Einarsen S, Hoel H, Notelaers G. Measuring exposure to bullying and harassment at work: validity, factor structure and psychometric properties of the Negative Acts Questionnaire-Revised. Work Stress 2009;23(1):24–44.Article
- 22. Mayhew C, Chappell D. Workplace violence: an overview of patterns of risk and the emotional/stress consequences on targets. Int J Law Psychiatry 2007;30(4-5):327–39.ArticlePubMed
- 23. Won SE, Choi MI, Noh H, Han SY, Mun SJ. Measuring workplace violence for clinical dental hygienists. Int J Dent Hyg 2021;19(3):340–9.ArticlePubMedPDF
- 24. Nam S, Hong S, Kim H, Wong JY, Fong DY. Reliability and validity of the Korean 12-item Perception of Aggression Scale. J Psychiatr Ment Health Nurs 2022;29(3):442–50.ArticlePubMedPDF
- 25. Chang SJ, Kang DM, Kang HT, Kim SY, Kim I, Kim JI. Development of Korean Emotional Labor and Workplace Violence Evaluation Tool. Ulsan, Korea: Occupational Safety and Health Research Institute; 2013.
- 26. Chang SJ, Kang HT, Kim SY, Kim IA, Kim JI, Kim HR, et al. Application Study of Korean Emotional Labor Scale and Korean Workplace Violence Scale. Ulsan, Korea: Occupational Safety and Health Research Institute; 2014.
- 27. Lawshe CH. A quantitative approach to content validity. Pers Psychol 1975;28(4):563–75.
- 28. An JY, Seo ER, Lim KH, Shin JH, Kim JB. Standardization of the Korean version of screening tool for depression (Patient Health Questionnaire-9, PHQ-9). J Korean Soc Biol Ther Psychiatry 2013;19(1):47–56.
- 29. Shin KH. The Maslach Burnout Inventory-General Survey (MBI-GS): an application in South Korea. Korean J Ind Organ Psychol 2003;16(3):1–17.
- 30. Schmitt N, Stults DM. Methodology review: analysis of multitrait-multimethod matrices. Appl Psychol Meas 1986;10(1):1–22.ArticlePDF
- 31. Dillon BL. Workplace violence: impact, causes, and prevention. Work 2012;42(1):15–20.ArticlePubMedPDF
- 32. Hunt ML, Hughey AW. Workplace violence: impact and prevention. KCA J 2010;29(1):39–43.
- 33. Gupta I, Eid SM, Harris CM, Kauffman R, Washburn C, Singh A, et al. Prevalence of workplace violence and effects of de-escalation training among hospitalists: a pilot study. J Community Hosp Intern Med Perspect 2023;13(3):1–5.ArticlePubMedPMC
- 34. Occupational Safety and Health Administration. Guidelines for Preventing Workplace Violence for Healthcare and Social Service Workers. Washington, DC: Occupational Safety and Health Administration; 2016.
- 35. Barling J, Dupre KE, Kelloway EK. Predicting workplace aggression and violence. Annu Rev Psychol 2009;60:671–92.ArticlePubMed
- 36. International Labour Organization. Ending Violence and Harassment in the World of Work. International Labour Conference, 108th Session. Geneva, Switzerland: International Labour Office; 2019.
- 37. Occupational Safety and Health Administration. Workplace violence. https://www.osha.gov/workplace-violence. Accessed January 20, 2024..
- 38. Andersen LPS, Biering K, Conway PM. Negative acts as risk factor for work-related violence and threats from clients towards employees: a follow-up study. Int J Environ Res Public Health 2023;20(4):3358.ArticlePubMedPMC
- 39. Jung S, Lee HJ, Lee MY, Kim ES, Jeon SW, Shin DW, et al. Gender differences in the association between workplace bullying and depression among Korean employees. Brain Sci 2023;13(10):1486.ArticlePubMedPMC
- 40. Nelson S, Ayaz B, Baumann AL, Dozois G. A gender-based review of workplace violence amongst the global health workforce: a scoping review of the literature. PLOS Glob Public Health 2024;4(7):e0003336.ArticlePubMedPMC
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Development of a First-tier Risk Assessment Tool for Occupational Hazards Among Public Officials
Sangjun Choi, Hayoung Lee, Juhyeon Jeong, Seonjin Lim, Soo-Young Lee, Jaehyun Park
Safety and Health at Work.2026; 17(2): 286. CrossRef
 Cite
CiteWorkplace Violence (KWVS®13): scale development and validation in the Korean context
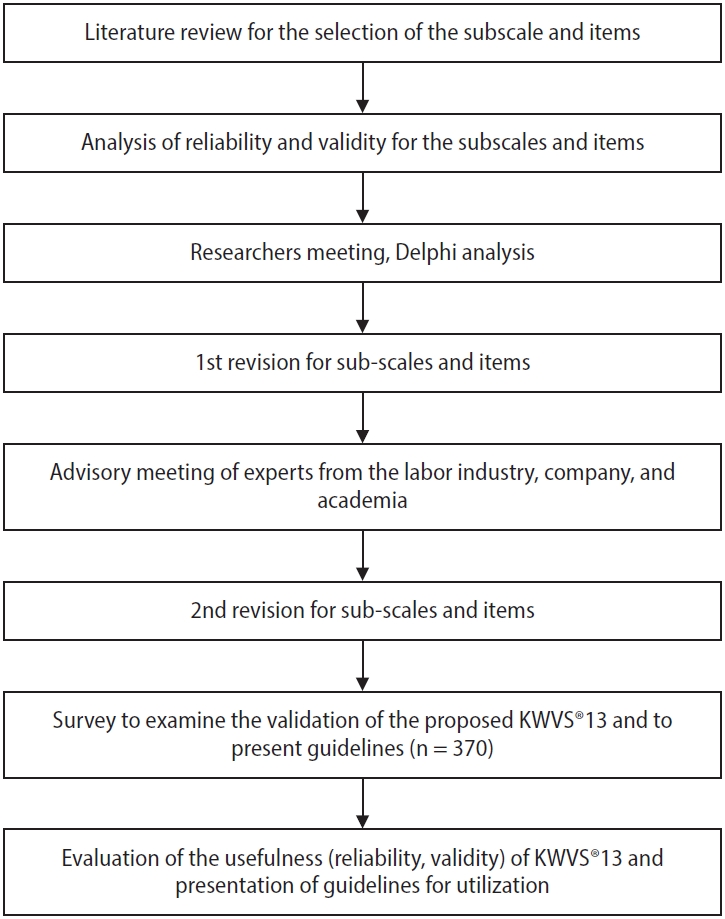

Fig. 1. Flowchart diagram of the study. KWVS: Korean Workplace Violence Scale.
Fig. 2. Subscales and items of KWVS®13. KWVS: Korean Workplace Violence Scale.
Fig. 1.
Fig. 2.
Workplace Violence (KWVS®13): scale development and validation in the Korean context
| Item | Factor |
||
|---|---|---|---|
| 1 | 2 | 3 | |
| KWVS_7 | 0.869 | 0.138 | 0.033 |
| KWVS_8 | 0.828 | 0.193 | 0.109 |
| KWVS_10 | 0.710 | 0.304 | –0.110 |
| KWVS_6 | 0.701 | 0.378 | –0.050 |
| KWVS_5 | 0.696 | 0.258 | 0.084 |
| KWVS_9 | 0.658 | 0.333 | –0.078 |
| KWVS_3 | 0.283 | 0.829 | –0.097 |
| KWVS_1 | 0.176 | 0.776 | –0.048 |
| KWVS_4 | 0.361 | 0.749 | 0.017 |
| KWVS_2 | 0.336 | 0.650 | –0.039 |
| KWVS_12 | –0.012 | –0.129 | 0.916 |
| KWVS_11 | –0.105 | –0.083 | 0.902 |
| KWVS_13 | 0.122 | 0.060 | 0.770 |
| Subscale | No. of items | Correlation coefficient |
Item convergent validity |
Item discriminant validity |
|||
|---|---|---|---|---|---|---|---|
| Convergent validity | Discriminant validity | No. of success | Success rate (%) | No. of success | Success rate (%) | ||
| Psychological and sexual violence from customer | 4 | 0.738–0.877 | 0.038–0.588 | 4/4 | 100 | 16/16 | 100 |
| Psychological and sexual violence from supervisor and coworker | 4 | 0.791–0.875 | 0.028–0.580 | 4/4 | 100 | 16/16 | 100 |
| Physical assault from customer/supervisor/coworker | 2 | 0.923–0.950 | 0.034–0.584 | 2/2 | 100 | 8/8 | 100 |
| Organizational protective system for workplace violence | 3 | 0.785–0.917 | 0.006–0.163 | 3/3 | 100 | 12/12 | 100 |
| Subscale | Burnout | Depression |
|---|---|---|
| Psychological and sexual violence from customer | ||
| Correlation coefficient | 0.283 | 0.280 |
| p-value | <0.001 | <0.001 |
| Psychological and sexual violence from supervisor and coworker | ||
| Correlation coefficient | 0.271 | 0.284 |
| p-value | <0.001 | <0.001 |
| Physical assault from customer/supervisor/coworker | ||
| Correlation coefficient | 0.115 | 0.167 |
| p-value | 0.028 | 0.001 |
| Organizational protective system for workplace violence | ||
| Correlation coefficient | 0.152 | 0.098 |
| p-value | 0.004 | 0.063 |
| Subscale | Cronbach’s alpha | |
|---|---|---|
| KWVS®13 | Psychological and sexual violence from customer | 0.827 |
| Psychological and sexual violence from supervisor and coworker | 0.860 | |
| Physical assault from customer/supervisor/coworker | 0.854 | |
| Organizational protective system for workplace violence | 0.834 | |
| Psychological and sexual violence from customer |
Psychological and sexual violence from supervisor and coworker |
Physical assault from customer/supervisor/ coworker |
Organizational protective system for workplace violence) |
|||||
|---|---|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | Male | Female | |
| Depression | ||||||||
| AUC | 0.719 | 0.624 | 0.781 | 0.630 | 0.705 | 0.569 | 0.522 | 0.602 |
| Sensitivity | 63.6 | 86.8 | 81.8 | 48.1 | 63.6 | 33.8 | 90.9 | 62.5 |
| Specificity | 74.3 | 32.1 | 63.6 | 74.3 | 71.4 | 81.2 | 23.4 | 56.0 |
| Cut-point | 8 | 5 | 5 | 6 | 2 | 2 | 10 | 8 |
| Reference values | Normal: 4–8 | Normal: 4–5 | Normal: 4–5 | Normal: 3–6 | Normal: 2 | Normal: 2 | Normal: 3–10 | Normal: 3–8 |
| Risk: 9–16 | Risk: 6–16 | Risk: 6–16 | Risk: 7–16 | Risk: 3–8 | Risk: 3–8 | Risk: 11–12 | Risk: 9–12 | |
Table 1. Results of factor analysis for KWVS®13
The bold fonts are the factor loading values belonging to each factor. KWVS: Korean Workplace Violence Scale.
Table 2. Convergent and discriminant validity of four subscales and items of KWVS®13
KWVS: Korean Workplace Violence Scale.
Table 3. Correlations between four subscales of KWVS®13, burnout and depression
KWVS: Korean Workplace Violence Scale.
Table 4. Cronbach’s alphas for four subscales of KWVS®13
Table 5. Sex-specific cutoff values and reference values for four subscales of KWVS®13
AUC: area under the receiver operating characteristic curve.

