Correlation between shift work and non-alcoholic fatty liver disease among male workers in the steel manufacturing company of Korea: a cross-sectional study
Article information

Abstract
Background
Circadian rhythm disturbance caused by shift work has adverse effects on the metabolic homeostasis of the liver. Disruption of the metabolic homeostasis of the liver causes fat accumulation in the liver. The aim of this study was to investigate the correlation between shift work and non-alcoholic fatty liver disease (NAFLD) among male workers in the steel manufacturing industry of Korea.
Methods
Based on medical examination data collected in June 2020, 2,511 male subjects from one steel manufacturing company in Korea were selected in total. NAFLD was evaluated using abdominal ultrasound, which was performed by two experienced radiologists. The multinomial logistic regression analysis was performed by adjusting for age, physical activity, smoking history, alcohol consumption, body mass index, waist circumference, blood pressure, blood glucose, lipidemia, liver function test, employment duration, and hepatotoxic materials exposure status.
Results
Compared to daytime workers, the odds ratio (OR) of moderate-severe NAFLD in shift workers was 1.449 (95% confidence interval [CI], 1.028–2.043). Compared to daytime workers, the ORs of moderate-severe NAFLD were significantly higher for the group that engaged in total shift work for more than 20 years (OR, 2.285; 95% CI, 1.051–4.970), the group that was not allowed to sleep during night shift work (OR, 1.463; 95% CI, 1.030–2.078), and the group that consumed food during night shift work (OR, 1.580; 95% CI, 1.093–2.284).
Conclusions
There was a correlation between shift work and moderate-severe NAFLD in male steel manufacturing workers. There will be a need for more research related to the correlation of shift work with steatohepatitis and cirrhosis in the future.
BACKGROUND
Non-alcoholic fatty liver disease (NALFD) is a condition in which excessive triglyceride is accumulated in the liver without liver disease due to secondary causes such as significant drinking, drug use, viral hepatitis, etc.1 Multiple meta-analyses23 have shown that the pooled overall prevalence of NALFD is approximately 25.2 to 29.8% worldwide, with an increasing trend from 21.9% in 1991 to 37.3% in 2019.3 The prevalence of NALFD in Korea is 32.87% (31.12%–34.67%).4 The prevalence of NAFLD in Korea has also increased, in line with the global trend, from 24.9% in 1998 to 31.0% in the period from 2008–2014.5 NAFLD can be related to mortality by progression to liver disease6 or liver-related complications such as liver cirrhosis7 and hepatocellular carcinoma.8 Therefore, it is important to prevent NAFLD before it develops into an irreversible disease.
In many countries, about 15 to 25 percent of the workforce consists of shift workers.9 Multiple studies have confirmed that circadian rhythm disturbance caused by shift work has various adverse effects on the body, such as in terms of blood pressure,10 diabetes,11 dyslipidemia,12 and cardiovascular disease.13 Studies have also shown that circadian rhythm disturbance may affect the metabolic homeostasis of the liver and cause fat accumulation, thus resulting in NAFLD.14 In this context, Zhang et al.15 published a study in China showing that current night shift workers among male steelworkers had elevated odds ratio (OR) of NAFLD (OR, 1.23; 95% confidence interval [CI], 1.02–1.48) compared to those who never worked night shifts, as confirmed through abdominal ultrasound. Meanwhile, a study by Choi et al.16 in Korea showed that the OR of abnormal liver enzyme (alanine aminotransferase) level in female shift workers was higher at 1.31 (95% CI, 1.00–1.71) compared to that in to daytime workers, although they did not conduct an analysis of the correlation between shift work and NAFLD. Ultimately, there have been limited large-scale studies in Korea analyzing the correlation between NAFLD and shift work using abdominal ultrasound, even though abdominal ultrasound is recommended as a primary screening tool for NAFLD.17
Therefore, the objective of this study was to investigate the correlation between shift work and NALFD based on the results of health examinations and abdominal ultrasounds of male workers in a steel manufacturing company in Korea. In addition, factors that might affect this correlation, such as total duration of shift work, whether or not sleeping was allowed during their night shift work, and whether or not food was consumed during their night shift work, were also identified.
METHODS
Subjects
This study utilized medical screening data obtained from workers in a steel manufacturing company in Korea. In total, 6,392 workers (daytime worker 3,011, shift worker 3,381) aged 19 years or more who underwent the mandatory medical examination and comprehensive medical screening from June 29, 2020 to August 14, 2020 were recruited. Prior to analysis, 46 subjects with missing values were excluded. Next, 110 women workers were excluded because there were no women involved in shift work in the company. Since the comprehensive medical screening was conducted alternately every two years, dividing the examinees by two leads to 3,401 subjects on whom abdominal ultrasound was performed. Based on the standards of the Korean Association for the Study of the Liver (KASL)’s NAFLD treatment guidelines,17 140 subjects with a history of hepatitis or liver disease and positive hepatitis antigens on blood test were excluded, as were 462 subjects of men with an average weekly alcohol intake of 210 g or more. Lastly, 288 subjects were excluded for having changed departments within one year, which was done in an attempt to minimize the effect of work conversion between shift work and daytime work to NAFLD during the one year prior to the examination. In total, 2,511 men workers (995 daytime workers and 1,516 shift workers) were ultimately selected as the final subjects for this study (Fig. 1).
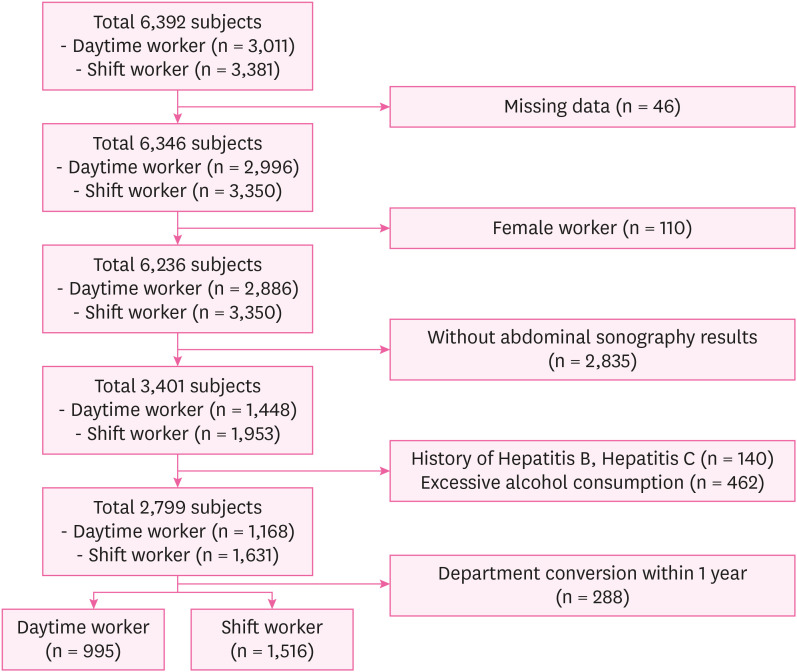
A flow of the study design.
General characteristics
The age, waist circumference, body mass index (BMI), physical activity, smoking history, alcohol consumption, blood pressure, blood glucose, lipidemia, and liver function test results of the study subjects were included as variables. Physical activity was classified into three groups—“Health promotion”, “Recommended exercise”, and “Risk”—according to the criteria of the World Health Organization's Physical Activity Recommendation Guidelines18 by examining weekly aerobic activity information obtained through a health examination questionnaire. Smoking history was classified into groups of “Non-smokers”, “Ex-smokers”, and “Current smokers.” Waist circumference was classified as “Normal” (< 90 cm) or “Abdominal obesity” (≥ 90 cm).19 BMI was classified into four groups, “Normal” (< 23 kg/m2), “Pre-obese” (23-24.9 kg/m2), “Obese class 1” (25-29.9 kg/m2), and “Obese class 2” (≥ 30 kg/m2).20
Blood pressure, blood glucose, lipidemia, and liver function test results were set as variables. Each variable was classified as described in the following based on the criteria for diagnosing disease in Korea, past medical history, physical examination, and blood test results. According to the Korean Society of Hypertension 2018 guidelines,21 subjects who had a systolic blood pressure of 140 mmHg or higher, had a diastolic blood pressure of 90 mmHg or higher, or were taking hypertension drugs at the time of examination were defined as “Abnormal blood pressure”; the remaining subjects were defined as “Normal.” According to the Korean Diabetes Association 2021 guidelines,22 subjects with a fasting blood sugar of 126 mg/dL or higher or who were taking diabetes drugs at the time of examination were defined as “Abnormal blood glucose”; the remaining subjects were defined as “Normal.” According to the blood test standards of the dyslipidemia guidelines,23 subjects who had at least one of the following were defined as “Dyslipidemia”: total cholesterol of 240 mg/dL or higher, triglyceride of 200 mg/dL or higher, high-density cholesterol of less than 40 mg/dL, low-density cholesterol of 160 mg/dL or higher, or taking dyslipidemia drugs at the time of examination. According to the criteria for health examination results of Korea,24 subjects who had at least one of the following were defined as “Abnormal liver enzyme”: aspartate aminotransferase > 40, alanine aminotransferase > 35, or γ-glutamyl transpeptidase > 63.
Weekly alcohol consumption
Since alcohol consumption is one of the diagnostic criteria for NAFLD,17 the alcohol consumption of each study subject was calculated weekly. Weekly alcohol consumption was calculated by examining the average number of alcohol drinks per week and the average alcohol intake per time according to the type of alcohol obtained through the questionnaire. It was calculated using the following equation25:
In terms of alcohol consumption, the subjects were classified into “Non-drinker” (0 g/week), “Moderate drinker” (1–111 g/week), and “Heavy drinker” (≥ 112 g/week).26
Occupational history and shift work-related variables
Duration of employment (month), current shift work status, and materials causing Toxic Associated Steatohepatitis (TASH) were set as variables related to occupational history. In terms of the status of current shift work, the subjects were classified into daytime workers and shift workers according to each worker’s work schedule. A worker was defined as a shift worker if they performed a monthly average of more than four 8-hour work shifts that included hours from 12 a.m. to 5 a.m. for six months, or if they on average worked more than 60 hours per month between 10 p.m. and 6 a.m. for six months.27 The remaining workers were defined as daytime workers. The type of shift work was a four-crew-three-shift system. The shift workers’ work schedule included shifts of 07:00–15:00 for the morning shift, 15:00–23:00 for the afternoon shift, and 23:00–07:00 for the night shift. Meanwhile, the daytime worker’s work schedule was 09:00–17:00.
It was next checked whether each subject worked with TASH-causing materials,28 such as organic solvents, lead, and mercury, to which workers might be exposed during work. Subjects were classified into two groups: 1) a group that handled TASH-causing materials and 2) a group that did not handle such materials.
Variables related to shift work were investigated in terms of the total duration of shift work, whether sleep was allowed during night shift work, and whether food was consumed during night shift work. Each variable was surveyed through a pre-written questionnaire that is used in the Notional Shift Work Special Health Examination.29 The total duration of shift work was classified into three groups: less than 10 years, 10–19 years, and 20 years or more. Whether sleep was allowed during night shift work was classified into two groups based on the response to the following question: “Is sleeping time allowed during night shift work?” The group that answered “Yes” was defined as “Allowed” whereas the other group that answered “No” was defined as “Not allowed.” Whether or not food was consumed during night shift work was classified into two groups: “Yes” and “No.”
Diagnostic criteria of NAFLD
NAFLD was evaluated using abdominal ultrasound (ARIETTA 750, FUJIFILM). Abdominal ultrasound was performed by two experienced radiologists. The examiners read the results without knowing the subject's variable exposure level or any information about the purpose of the investigation. The diagnosis of fatty liver was based on the following features30: increased echoes in hepatic parenchyma (stronger than the kidney and spleen), loss of portal vessels wall echo, and non-visualization of diaphragm. Abdominal ultrasound readings were classified into four grades. If there were no signs of abnormality, a reading was defined as “Normal.” If there was a slight and diffuse increase of liver echogenicity with normal visualization of the diaphragm and of the portal vein wall, it was defined as “Light grade.” If there was a moderate increase of liver echogenicity with slightly impaired appearance of the portal vein wall and the diaphragm, it was defined as “Moderate grade.” If there was a marked increase of liver echogenicity with poor or no visualization of portal vein wall, diaphragm, and posterior part of the right liver lobe, it was defined as “Severe grade.” Severe grade was classified along with the moderate grade group because there were 35 severe grade cases in total, thus showing a small distribution (1.39% of the total distribution) among the total distribution. Ultimately, the grade of NAFLD was classified into three groups: Normal, Light NAFLD, and Moderate-Severe NAFLD.
Statistical analysis
The Student’s t-test and the χ2 test were conducted to examine the general characteristics of the study subjects according to their current status of shift work. The χ2 test was conducted to examine shift work-related variables of study subjects according to the grade of NAFLD. Continuous variables were expressed as mean and standard deviation. Categorical variables were expressed as numbers and proportion. The multinomial logistic regression analysis was conducted to verify the effect of shift work and shift work-related variables on NAFLD compared to daytime work. All statistical analyses were performed with SPSS version 25.0 (IBM, Corp., Armonk, NY, USA) program, and p-values of less than 0.05 were considered to be statistically significant.
Ethic statement
The Institutional Review Board (IRB) of Soonchunhyang University Cheonan Hospital approved this study (IRB No. 2022-04-016). The requirement of informed consent was waived due to its retrospective nature.
RESULTS
General characteristics and shift work-related variables
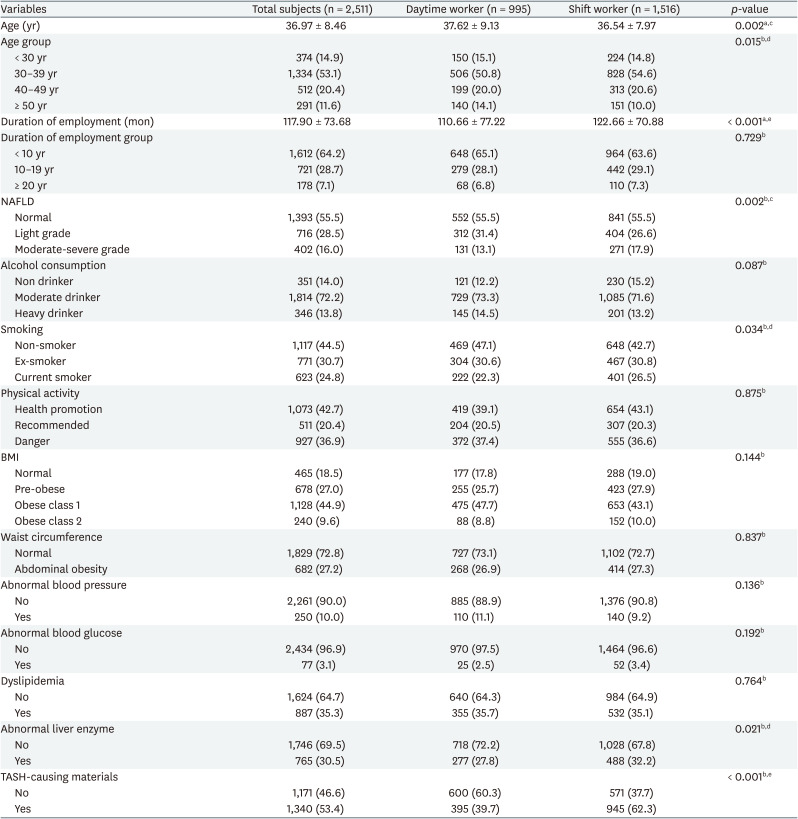
Information regarding the general characteristics, occupational characteristics, abnormal exam finding, and TASH-causing materials among the study subjects is presented in Table 1. In total, 2,511 subjects were included in the final analysis. Among the subjects, there were 995 daytime workers and 1,516 shift workers. Regarding mean age, shift workers were significantly younger than daytime workers. For mean employment duration, shift workers showed significantly longer employment duration. The proportion of NAFLD, age group, smoking, abnormal liver enzyme, and TASH-causing materials were all significantly different between daytime workers and shift workers.
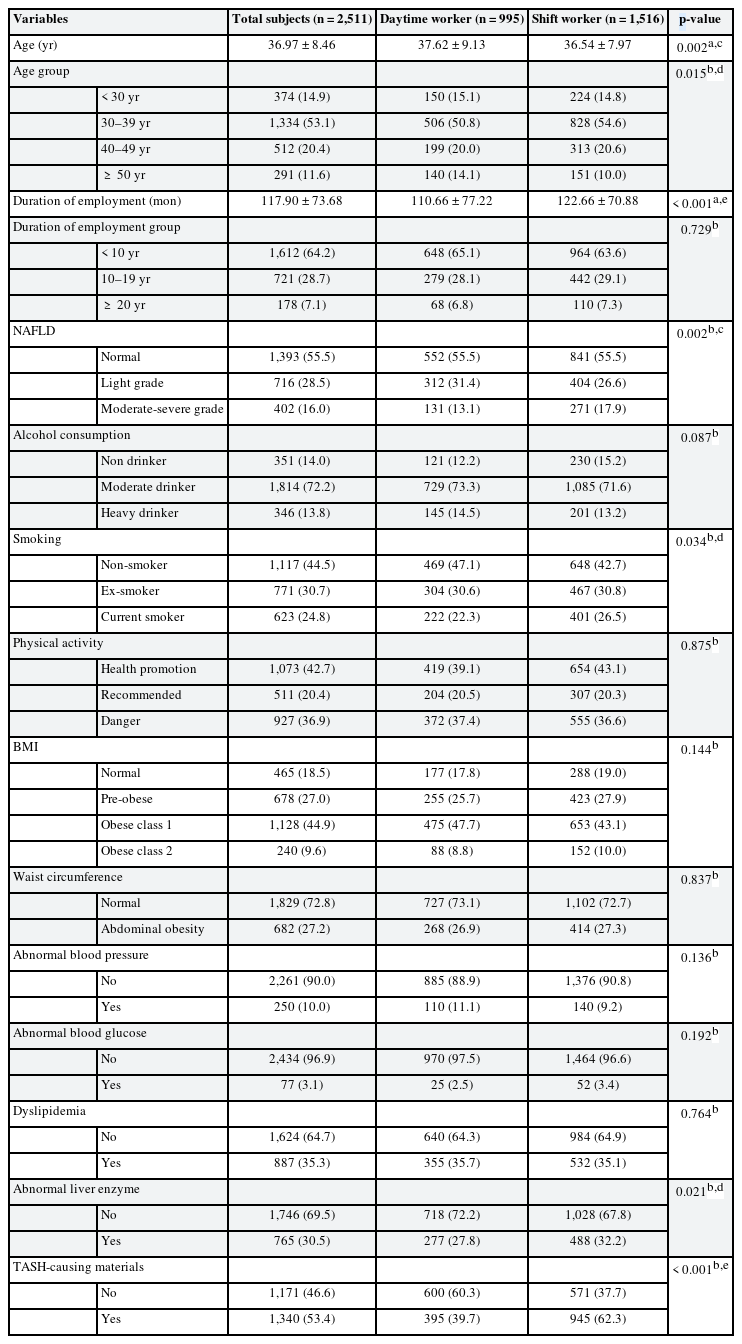
General characteristics of study subjects
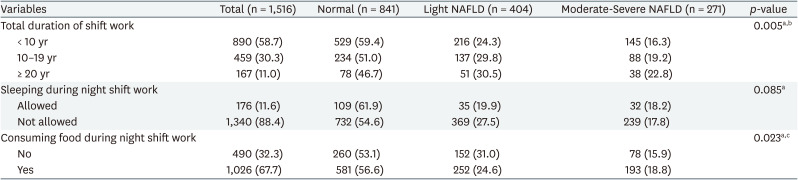
The shift work-related variables of the study subjects are presented in Table 2. The proportion of NAFLD severity was found to be significantly different according to total duration of shift work. The proportion of NAFLD severity was also significantly different between the food consuming group and non-food consuming group during night shift work.
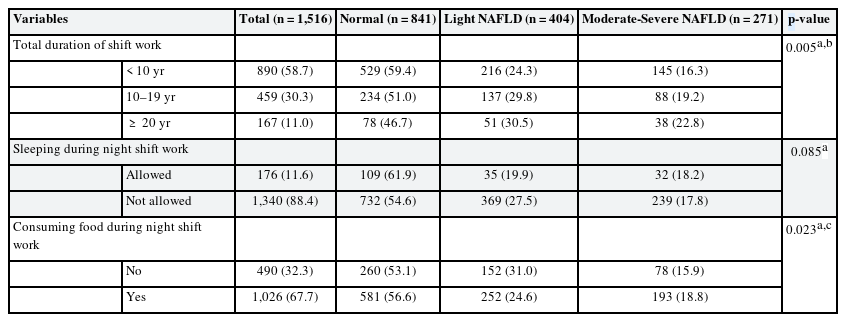
Shift work-related variables of study subjects
OR of NAFLD according to shift work
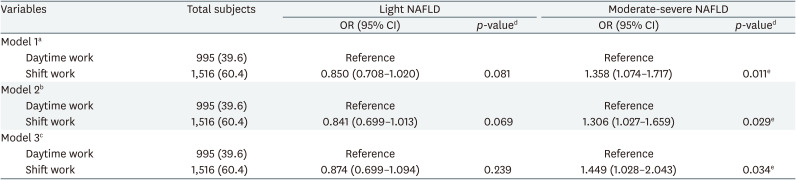
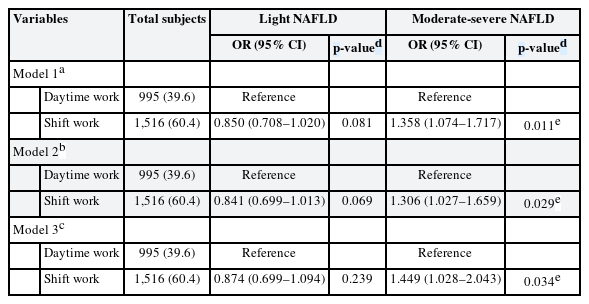
Table 3 presents the association between shift work and NAFLD according to multinomial logistic regression. Compared to daytime workers, the OR of light NAFLD in shift workers was found to be low, but the difference was not significant in all models. Moreover, compared to daytime workers, the OR of moderate-severe NAFLD was significantly higher in shift workers. After adjusting for associated variables (model 3), the OR of moderate-severe NAFLD in shift workers was 1.499 (95% CI, 1.028–2.043) compared to daytime workers.
OR of NAFLD according to shift work
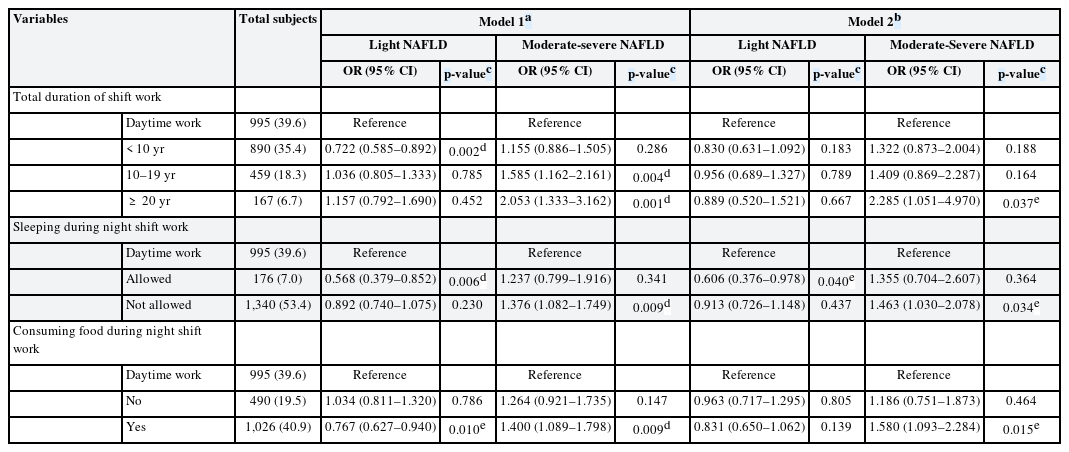
ORs of NAFLD according to shift work-related variables
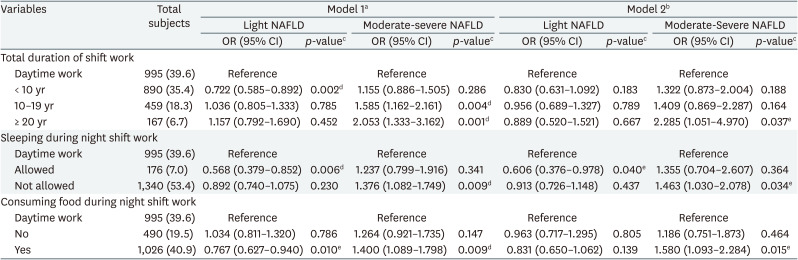
The associations between shift work-related variables and NAFLD from multinomial logistic regression are presented in Table 4. After adjusting for associated variables (model 2), compared to daytime workers, the ORs of light NAFLD was found to be significantly lower for the group that was allowed to sleep during night shift work (OR, 0.606; 95% CI, 0.376–0.978). Compared to daytime workers, the ORs of moderate-severe NAFLD were significantly higher for the group that engaged in total shift work duration for more than 20 years (OR, 2.285; 95% CI, 1.051–4.970), the group that was not allowed to sleep during night shift work (OR, 1.463; 95% CI, 1.030–2.078), and the group that consumed food during night shift work (OR, 1.580; 95% CI, 1.093–2.284).
ORs of NAFLD according to shift work-related variables
DISCUSSION
NAFLD risk factors known to date include obesity,31 diabetes,2 dyslipidemia,32 metabolic syndrome,33 decreased physical activity and sarcopenia,1734 genetic factors,35 hypothyroidism,36 and pituitary dysfunction.37 In this study, factors such as high blood pressure known to be diagnostic criteria for metabolic syndrome, physical activity, diabetes, and dyslipidemia were adjusted and analyzed. However, tests for other risk factors were not conducted. Nonetheless, this study controlled these risk factors by investigating past medical history through a detailed questionnaire. Since diseases such as hypothyroidism and pituitary dysfunction have a lower prevalence than other tested variables,3839 their effects on results might be insignificant.
The NAFLD proportion in all subjects in this study was 44.5%. This differed from the prevalence of NAFLD in Korea that had been analyzed through a meta-analysis.4 However, the prevalence stated in that meta-analysis was the prevalence of the entire Korean population. Meanwhile, according to another study,5 the pooled overall prevalence of NAFLD in Korean adult men was 41.1%, and the prevalence of NAFLD in Korean adult men in the period from 2008–2014 was 44.4%. This is similar to the prevalence in this study, where the study subjects are composed of adult men.
The results presented in Table 3 suggest that shift work has a correlation with moderate-severe NAFLD. In this study, the OR of moderate-severe NAFLD for shift workers was 1.449 (95% CI, 1.028–2.043). This OR is similar to the OR of moderate-severe NAFLD for shift workers that was reported in a previous study.15 This study additionally investigated and analyzed TASH-causing materials, which were not covered in that previous study.15 This additional investigation has contributed to a more precise analysis of the correlation between shift work and NAFLD.
The mechanisms by which shift work causes NAFLD are as follows: First, the body’s circadian rhythm is repeated in a constant cycle. The circadian rhythm is typically consistent with the environmental cycle of day and night.40 The circadian rhythm is associated with several mechanisms related to metabolism: for example, the circadian rhythm has a regulatory role in glucose, lipid, and bile acid homeostasis in the liver.41 In shift work, it is inevitable to avoid exposure to light during the night, which affects the secretion of melatonin.42 Disturbed melatonin hormone secretion and circadian rhythm disturbance can affect the metabolic homeostasis of the liver, resulting in imbalance in the use and accumulation of nutrients through bile acid degeneration. The broken balance of carbohydrate and fat metabolism causes fat build-up in the liver, which leads to NAFLD.41 Second, there is a possible mechanism related to the oxidative stress protection role of melatonin. Oxidative stress is known to cause mitochondrial dysfunction, which is associated with fat accumulation in the liver.43 Melatonin is known to protect mitochondria from oxidative stress.44 However, if melatonin secretion is disturbed by shift work,42 this protective effect will become insufficient, resulting in NAFLD due to oxidative stress.
This study showed that total shift work duration, restriction on sleep during night shift work, and food intake during night shift work were all correlated with moderate-severe NAFLD. As can be seen in Table 4, the group with more than 20 years of total shift work duration showed a higher moderate-severe NAFLD risk than the daytime work group (OR, 2.285; 95% CI, 1.051–4.970). A previous study also showed significantly higher moderate-severe NAFLD risk in the group with shift work duration over 20 years compared to the group that never worked shift work.15 It is believed that circadian rhythm disturbance caused by chronic shift work may be correlated with the development of moderate-severe NAFLD.
The group that was not allowed to sleep during night shift work showed significantly higher moderate-severe NAFLD risk compared to daytime workers (OR, 1.463; 95% CI, 1.030–2.078). A possible cause for this is that sleeping during night shift work could reduce disturbance of the circadian rhythm.45 In view of this result, ensuring adequate sleep time for shift workers might help prevent fatty liver development in shift workers. However, this study only analyzed simple sleep availability, rather than making an accurate classification according to the number of sleep sessions, the duration of sleep, and the quality of sleep. Therefore, a future study in this area should include a deeper analysis of sleep condition.
The group that consumed food during night shift work showed a higher moderate-severe NAFLD risk than daytime workers (OR, 1.580; 95% CI, 1.093–2.284). The abnormal dietary intake of shift workers is known to cause chronic sleep disorders and increase fat needs, thus leading to obesity and diabetes.46 In another study,47 the results of measuring post-meal hormones and blood sugar in simulated shift work suggested that consuming meals during shift work could lower insulin sensitivity and affect blood sugar, which affect fat metabolism in the liver.48 To reduce the impact of shift work on NAFLD, it may be necessary to consider establishing restrictions on food intake during night shift work.
In multinomial logistic regression analysis, moderate-severe NAFLD showed statistically significant differences between shift workers and daytime workers, whereas light NAFLD mostly did not show statistically significant differences. This might be due to the characteristics of NAFLD diagnosis through abdominal ultrasound. Although abdominal ultrasound is reliable for diagnosing moderate or higher NAFLD, its diagnostic value is low for light NAFLD because of its relatively low sensitivity and specificity compared to moderate or higher NAFLD, leading to possible misdiagnosis.17 Thus, such statistically insignificant results could be due to limitations of abdominal ultrasound, which could not accurately distinguish between normal and light NAFLD.
This study has several limitations: First, since this was a cross-sectional survey study, it could not clearly analyze the causal relationship between variables. Second, since this study did not consider previous shift work history (aside from total duration of shift work) and only considered current shift work status, there is a limitation in that it was not possible to analyze the impact of changes in the shift work status; however, this study excluded examinees who had changed departments within the past year to alleviate this limitation. Third, there are several biases that could not be avoided because some variables were investigated through a self-report questionnaire. Fourth, since this study only concerned the presence or absence of NAFLD, correlations of shift work with steatohepatitis49 and cirrhosis,50 which are both known to be important factors for the prognosis of NAFLD, were not analyzed. Future research should consider these factors. Finally, there was a limitation in that the impact on women could not be analyzed because there were no female shift workers among the subjects of this study. Therefore, there was a population bias, which limits the generalizability of the results of this study to the entire population.
However, this study has the following advantages: First, the presence or absence of fatty liver was determined through imaging tests known to have high diagnostic accuracy. Second, it is meaningful in that this is a study with a large number of subjects among studies using imaging tests on NAFLD. Third, specific weekly average alcohol intake along with exercise intensity and time were investigated through questionnaires to set more quantitative and detailed variables. Finally, not only the correlation between shift work and NAFLD, but also variables related to shift work were checked to analyze which variables were related to NAFLD.
CONCLUSIONS
There was a correlation between shift work and moderate-severe NAFLD in male steel manufacturing workers. From an industrial health perspective, this study is significant in that it confirms the necessity of preventing and managing NAFLD among shift workers.
ACKNOWLEDGEMENTS
We would like to thank Harrisco (www.harrisco.net) for English language editing.
Notes
Funding: This work was supported by the Soonchunhyang University Research Fund.
Competing interests: The authors declare that they have no competing interests.
Author Contributions:
Conceptualization: Kim K.
Data curation: Kim K, Kim SH Formal analysis.
Software: Kim K.
Validation: Kim K.
Visualization: Lee HK, Baek G.
Writing - original draft: Kim K, Jang EC.
Writing - review & editing: Jang EC, Lee YJ, Kwon SC, Min YS.