Association between sitting-time at work and incidence of erosive esophagitis diagnosed by esophagogastroduodenoscopy: a Korean cohort study
Article information

Abstract
Background
Most previous longitudinal studies on lifestyle and gastroesophageal reflux disease (GERD) have focused on physical activity rather than sitting time. The main purpose of this study was to investigate the relationship between prolonged sitting time and the development of erosive esophagitis (EE).
Methods
A self-report questionnaire was used for measuring sitting time in the Kangbuk Samsung Health Study. Sitting time was categorized into four groups: ≤ 6, 7–8, 9–10, and ≥ 11 hours/day. Esophagogastroduodenoscopy (EGD) was performed by experienced endoscopists who were unawared of the aims of this study. Hazard ratios (HRs) and 95% confidence intervals (CIs) for the development of EE were estimated using Cox proportional hazards analyses with ≤ 6 hours/day sitting time as the reference.
Results
There were 6,524 participants included in the study. During a mean follow-up of 3.14 years, 2,048 incident cases developed EE. In age- and sex-adjusted models, the HR in the group sitting ≥ 11 hours per day compared ≤ 6 hours per day was 0.88 (95% CI: 0.76–0.99). After further adjusting for alcohol intake, smoking status, educational level, history of diabetes, and history of dyslipidemia, sitting time was still significantly related to the risk of EE (HR, 0.87; 95% CI: 0.76–0.98). After further adjustment for exercise frequency, this association persisted (HR, 0.86; 95% CI: 0.76–0.98). In subgroup analysis by obesity, the relationship between sitting time and EE was only significant among participants with body mass index < 25 kg/m2 (HR, 0.82; 95% CI: 0.71–0.95).
Conclusions
Generally, prolonged sitting time is harmful to health, but with regard to EE, it is difficult to conclude that this is the case.
BACKGROUND
Gastroesophageal reflux disease (GERD) is a common gastrointestinal disease that affects quality of life.12 GERD can be diagnosed if there are related symptoms or reactions to proton pump inhibitors, but it is also possible to observe inflammation through esophagogastroduodenoscopy (EGD).3
As reported by a multicenter study using EGD findings and questionnaires for GERD diagnosis at 40 hospitals in South Korea, the prevalence of GERD was 12%, and GERD can be divided into non-erosive reflux disease and erosive esophagitis (EE).4 In addition, the prevalence of GERD has gradually increased in Asia, including South Korea.356 Obesity,789 smoking,9101112 alcohol intake,1113 diet,1213 and vigorous physical activity1415161718192021 are known as GERD risk factors whereas recreational physical activity reduces GERD risk.22 Most previous studies on lifestyle as a risk factor for GERD have focused on physical activity, but studies regarding sitting time as a risk factor for GERD are rare.
According to the Korea National Health and Nutrition Examination Survey (KNHANES), the average daily sitting time of adults aged 19 years and older was 7.5 hours in 2014 and 8.6 hours in 2019; this indicates that sitting time is increasing.23 To date, sitting time is known to be associated with hypertension,24 diabetes,24 mortality,25 and musculoskeletal disorders,2627 but the relationship between prolonged sitting time and GERD is unclear.
Previous cross-sectional study suggesting sedentary lifestyle is a risk factor of GERD have limitation because they have measured subjective symptoms, mainly using questions or structured questionnaires.28 Also, there are studies suggesting sedentary white collar worker had less gastritis29 and prolonged sitting time was associated with peptic ulcer and other digestive.30 However, it is difficult to conclude that prolonged sitting time, in other words, sedentary lifestyle is a risk factor for GERD from above studies because demographic characteristics, definition of each variable, and methods are different. The mechanism underlying the association between prolonged sitting time and GERD still remains unclear. Therefore, through this longitudinal study, we aimed to overcome the limitations of previous studies and explore the effect of prolonged sitting time during the day on the development of GERD by using EGD results in a large-scale longitudinal study.
METHODS
Study population
Data for the study were obtained from the Kangbuk Samsung Health Study (KSHS, A cohort of Korean men and women aged 18 years or older who underwent comprehensive annual or biennial screening health examinations at the two Kangbuk Samsung Hospital Health Screening Centers in Seoul and Suwon, South Korea). KSHS data was obtained by performing data cleaning process for accurate analysis, such as removing potential errors including duplicates. More than 80% of participants were employees of various companies and local governmental organizations, or their spouses. In addition to the examination items guaranteed by South Korean Industrial Safety and Health, all participants were provided with other tests from the company. This annual or biennial comprehensive screening health examination included anthropometric measurements, various laboratory studies, chest radiography, EGD, abdominal sonography, epidemiological questionnaire on lifestyle factors, medication use, chronic disease, and history of malignancy. This was a longitudinal study of participants in the KSHS between January 2012 and December 2018. Data from 218,904 participants were available. We used the question “During the past week, did you work?” to check whether participants worked or not, and all participants answered “Yes”. The exclusion criteria were missing data regarding sitting time (n = 46,764), absence of an EGD or EGD failure (n = 34), and abnormal findings on EGD at baseline (n = 210,365). Finally, total 6,524 participants were included in this analysis (Fig. 1).
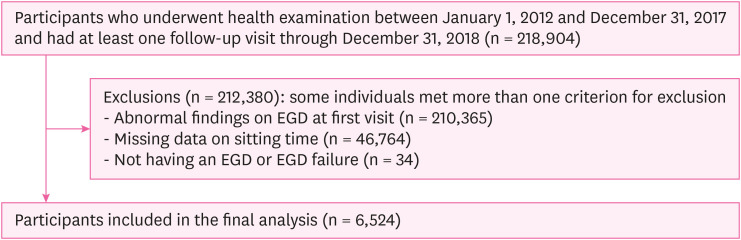
Flowchart of study participants.
EGD: esophagogastroduodenoscopy.
Measurements
Data on demographic characteristics, medical history, education level, and health-related behaviors including smoking status, alcohol intake, and exercise frequency were measured using self-administered, standardized questionnaires. We defined sitting time using the validated Korean version of the International Physical Activity Questionnaire (IPAQ) short form.3132 Total sitting time on weekdays was defined by the answers to the question, ‘During the last 7 days, how much time did you usually spend sitting on a weekday?’. We categorized the sitting time measured in integer units into the following groups and allocated as much as 25%: ≤ 6, 7–8, 9–10, and ≥ 11 hours/day. The minimum unit of measurement was one hour. Sitting time was measured at each visit, and the first visit data was used as baseline for analysis.
EGD was performed by experienced endoscopists who were unaware of the aims of this study. EE was defined as the presence of mucosal breaks at the gastroesophageal junction or Barrett’s esophagitis. Clinical factors, such as height and body weight, were measured by trained nurses. Alcohol intake (g/day) was calculated using type of drink, frequency of drinking, and drink amount per time, and divided into 2 categories: ≥ 10 g/day and < 10 g/day. Diabetes was defined as a glycated hemoglobin concentration (HbA1c) ≥ 6.5%. Dyslipidemia was defined as the current use of antidyslipidemic drug, and the use of statins may prevent the occurrence of EE in patients with GERD.33 The frequency of exercise each week was also assessed by the IPAQ.3132 Exercise was divided into 2 categories: ≥ 3 times/week and < 3 times/week. Education level was divided into two categories: less than college, college graduate, and lower education level may be associated with GERD.34
Statistical analysis
Baseline characteristics of the study populations were explored according to categorized sitting time using trend test. Data were presented as percentages for categorical variables and means with standard deviation (SD) for continuous variables. The primary endpoint was the development of EE in the EGD study. Study participants were followed up from the baseline to the primary endpoint visit or to the last available visit before December 31, 2018, whichever came first.
The incidence rates were calculated as the number of incident cases divided by person-years of follow-up. Cox proportional hazards regression analysis was used to estimate the adjusted hazard ratio (HR) with 95% confidence intervals (CIs) for incident EE. We used three models with progressive adjustments. Model 1 was adjusted for age and sex. Model 2 was further adjusted for alcohol intake, smoking status, educational level, history of diabetes, and history of dyslipidemia. Model 3 was further adjusted for exercise frequency. In addition, we performed a subgroup analysis stratified by body mass index (BMI) (< 25 vs. ≥ 25 kg/m2).
Statistical analysis was performed using STATA version 16.1 (StataCorp LP, College Station, TX, USA). All reported p-values were two-tailed. Statistical significance was set at p < 0.05.
Ethical consideration
The study was approved by the Institutional Review Board of Kangbuk Samsung Hospital (approval number: KBSMC 2021–08–036). The requirement for informed consent was waived owing to the use of de-identified data.
RESULTS
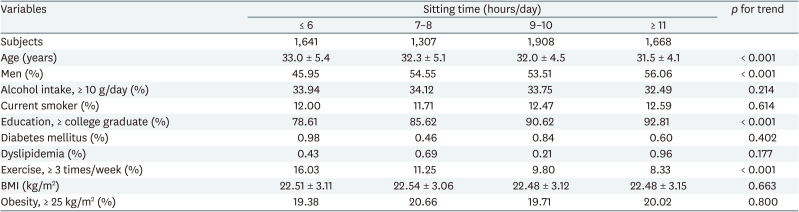
The mean sitting time of participants was 8.8 hours, and it was relatively evenly distributed by 25% in 4 categories: ≤ 6, 7–8, 9–10, and ≥ 11 hours/day. The mean ± SD age, BMI were 32.2 ± 4.8 years, and 22.50 ± 3.11 kg/m2, respectively. Sitting time was associated with age, sex, educational level, and exercise frequency. Participants in the prolonged sitting time category were more likely to be younger, highly educated, and less likely to exercise (Table 1).
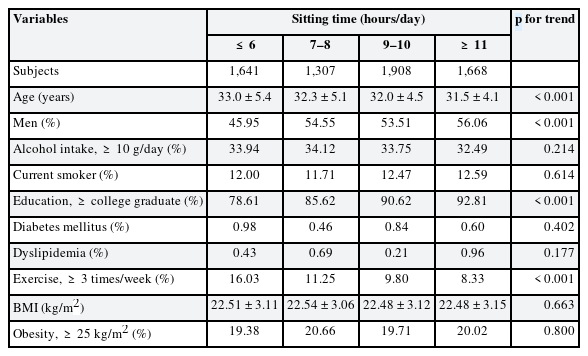
Baseline characteristics of study population by sitting time per day
We identified 2,048 incident cases of EE during 20,497.1 person-years of follow-up (incident rate 1.0 per 10 person-years). The mean follow-up period for participants was 3.14 years. In the crude models, there were no statistically significant differences. However, in multivariable-adjusted models, as the sitting time increased sequentially, the incidence of EE decreased (Table 2). In age- and sex-adjusted models, the HR (95% CI) in group sitting more than 11 hours per day comparing to less than 6 hours per day were 0.88 (0.76–0.99). After further adjusting for smoking status, educational level, history of diabetes, history of dyslipidemia, and sitting time were still significantly related to the risk of EE (HR, 0.87; 95% CI: 0.76–0.98). After further adjustment for exercise frequency, this association persisted. (HR, 0.86; 95% CI: 0.76–0.98).
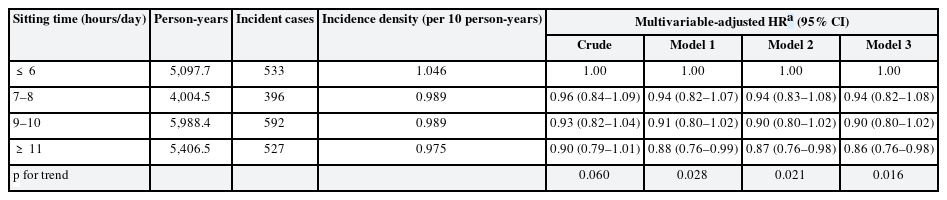
HR for the incidence of erosive esophagitis by sitting time per day
We additionally performed subgroup analysis on obesity, known as a risk factor for EE, and found that the relationship between sitting time and EE was only significant among participants with BMI < 25 kg/m2 (HR, 0.82; 95% CI: 0.71–0.95) (Table 3).
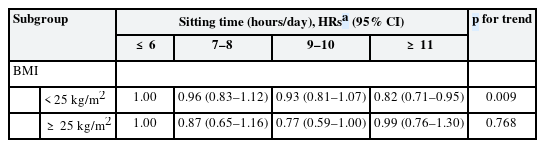
Incidence of erosive esophagitis by sitting time per day stratified by obesity
DISCUSSION
In our longitudinal study, prolonged sitting time was associated with a significantly lower risk of EE. Even after adjusting for relevant covariates including age, sex, alcohol intake, smoking status, education level, history of diabetes known as risk factor of GERD,35 use of antidyslipidemic drug, and exercise, the association was still significant. In subgroup analysis, the effects of prolonged sitting time on EE differed according to obesity, while the association was only significant in the non-obese group.
There have been several previous studies on lifestyle and gastrointestinal diseases. However, longitudinal studies on prolonged sitting time as a risk factor for GERD are rare. Most previous studies of lifestyle as a risk factor for GERD have focused on physical activity and, along with recent 2020 World Health Organization guidelines, recommend avoiding physical inactivity and sedentary lifestyle which are known as risk factors for hypertension, diabetes, obesity, cardiovascular disease, all-cause mortality, malignancy, and mental health.36
While prolonged sitting time can have a different effect on each gastrointestinal disease, physical activity, except vigorous activity, has a protective effect on gastrointestinal disease. In a Korean cross-sectional study using Samsung Medical Center’s Health Promotion data, physical activity was inversely associated with EE independent of BMI.37 There are several studies supporting the above results.1222383940 However, physical activity at work22 and vigorous activity can induce acid reflux and eventually cause GERD.1415161718192021 An Indian cross-sectional study, contrary to our study, suggested sedentary lifestyle could be a risk factor for development of GERD.28 However, they defined sedentary physical activity only by asking questions about occupational, domestic, and leisure time without measuring the average sitting time per day. And they defined GERD using symptom scores measured by questionnaires. In a Greek cross-sectional study of workers using EGD and colonoscopy, sedentary white-collar workers had less gastritis than blue-collar workers, while blue-collar workers had less Crohn’s disease than white-collar workers.29 However, in a Cancer Prevention Study-II (CPS-II) Nutrition Cohort Study of adults aged 50–74 years using International Classification of Diseases (ICD) codes, prolonged sitting time was associated with peptic ulcer and other digestive diseases (relative risk, 1.31; 95% CI: 1.09–1.57).30
The mechanism underlying the association between prolonged sitting time and GERD still remains unclear. However, several studies supporting physical activity and obesity are related to GERD, and proposed mechanisms are consistent with our findings. In a previous study on the association between physical activity and GERD, athletes had more acid reflux events than the general population.1415161718192021 Increased abdominal wall pressure caused by air inhalation into the stomach and contracted skeletal muscle when exercising with partly digested stomach contents can induce acid reflux. In addition, other studies have reported that recreational physical activity reduces GERD risk, while vigorous work and physical activity at work increase GERD risk.22 According to the above studies, physical activity at work may actually increase the risk of acid reflux when food in the stomach is incompletely digested. Most Korean workers have a lunch break of less than an hour. In the case of office workers, they continue their sedentary work, but in the case of workers engaged in manufacturing, they restart their physical work without sufficient digestion time. Our study subjects were all workers. Therefore, the group sitting more than 11 hours per day is likely to be office workers. Conversely, the group sitting less than 6 hours per day is likely to engage in physical activity while on duty. Therefore, people who spend more time sitting are likely to engage in sedentary work and thus could have more time to digest lunch, and finally have fewer gastric acid reflux events during the daytime.
Meanwhile, in our study, the incidence of EE decreased as the sitting time increased only in the non-obese group. We estimated that obesity may play a role as a confounder or mediator in the relationship between sitting time and EE, because it is well-known that obesity is risk factor of GERD.41 Therefore, we performed a subgroup analysis according to obesity, and it was confirmed that sitting time was associated with EE only in the non-obese group. Because it is possible that the effect of prolonged sitting time on the development of EE may be strongly confounded by obesity.
There were several limitations to this cohort study. First, our study data consisted of relatively healthy and well-educated young and middle-aged adults. Our data may not accurately reflect socioeconomic status (SES) because various SES data such as income and occupation were incompletely collected. However, general health risk factors such as diabetes mellitus and dyslipidemia and educational level have been factored into adjustments. Therefore, results similar to those of our study could be expected in populations with poorer health, other medical conditions and other SES. Second, measurement bias could not be avoided because we used a sitting time questionnaire (single item). However, we attempted to overcome this bias by investigating and correcting the exercise frequencies. Third, other possible confounders, such as diet and medication use (proton pump inhibitors, antacids), were not factored into adjustments. Fourth, because the Helicobacter pylori test cannot be performed on everyone for ethical reasons, the H. pylori state was not considered. Despite these limitations, our study has the advantage of analyzing the association between sitting time and GERD using EGD findings in a large-scale cohort study. Fifth, dietary and lifestyle habits such as coffee intake, postprandial posture, late night snack frequency was not considered. Further studies are needed to reflect various dietary and lifestyle habits.
In conclusion, it is generally recognized that a sedentary lifestyle is harmful to health, but with regard to EE, it is difficult to conclude that it is the case. In large-scale surveys including our cohort survey, the KNHANES and the Labor Panel Survey, the measurement of sitting time and the frequency and amount of physical activities during the day in the questionnaires are very simple, probably due to limitations of manpower, time, and financial resources. Therefore, the establishment of a strategy to prevent GERD, which is a common disease, in the working environment is still lacking. In the future, it will be necessary to conduct a more detailed investigation into the time spent sitting and the work environment after meals.
Notes
Funding: This work was supported by the Korean Society of Occupational and Environmental Medicine (KSOEM).
Competing interests: The authors declare that they have no competing interests.
Author Contributions:
Conceptualization: Lee W.
Investigation: Lee Y, Mun E, Seo E, Lee W.
Methodology: Kim D, Lee Y, Jeong Y, Lee J, Lee W.
Supervision: Jeong J.
Writing - original draft: Kim D.
Writing - review & editing: Lee W.
Abbreviations
BMI
body mass index
CI
confidence interval
CPS-II
Cancer Prevention Study-II
EE
erosive esophagitis
EGD
esophagogastroduodenoscopy
GERD
gastroesophageal reflux disease
HbA1c
hemoglobin concentration
HR
hazard ratio
ICD
International Classification of Diseases
IPAQ
International Physical Activity Questionnaire
KNHANES
Korea National Health and Nutrition Examination Survey
KSHS
Kangbuk Samsung Health Study
SD
standard deviation
SES
socioeconomic status