Association between work from home and health-related productivity loss among Korean employees
Article information

Abstract
Background
After the coronavirus disease 2019 pandemic, the widespread adoption of working from home, or teleworking, has prompted extensive research regarding its effects on work productivity and the physical and mental health of employees. In this context, our study aimed to investigate the association between working from home and health-related productivity loss (HRPL).
Methods
An online survey was conducted with a sample of 1,078 workers. HRPL was estimated by the Work Productivity and Activity Impairment Questionnaire: General Health version. Workers that have been working from home in the last 6 months were categorized into the “work from home” group. Generalized linear models were used to compare the mean difference of HRPL between “work from home” and “commuters” group. Stratified analyses were conducted based on various factors including gender, age, income level, occupation, education level, previous diagnosis of chronic disease, presence of preschool children, living in studio apartment, living alone, commuting time, working hours and regular exercise.
Results
The overall HRPL was higher in the “work from home” group than in the “commuters” group with a mean difference of 4.05 (95% confidence interval [CI]: 0.09–8.01). In the stratified analyses, significant differences were observed in workers with chronic diseases (mean difference: 8.23, 95% CI: 0.38–16.09), who do not live alone (mean difference: 4.84, 95% CI: 0.35–9.33), and workers that do not exercise regularly (mean difference: 4.96, 95% CI: 0.12–9.80).
Conclusions
Working from home is associated with an increased HRPL in the Korean working population, especially among those with chronic diseases, those who do not live alone, and those who do not exercise regularly.
BACKGROUND
Following the coronavirus disease 2019 (COVID-19), the government emphasized and recommended physical distancing. Therefore, working from home, a working model in which workers do their job at home,1 has been widely implemented. According to Statistics Korea, the number of workers working from home has increased by 10 times after the pandemic, from 95,000 in August 2019 to 956,000 in August 2022.2 Working from home is also referred to as remote working, telecommuting or teleworking.
Previous research has presented the heterogeneous health outcomes of working from home. In terms of physical health, the absence of proper work equipment and environment can have a negative effect,3 while another study showed that men experienced lower level of pain when they worked from home.4 Women had a lower possibility of having improved health outcomes from working from home.5 Teleworking has been reported to have detrimental effects on mental health. Teleworkers reported greater loneliness, irritability, worry, guilt and increased mental health symptoms of stress.6 Working from home is associated with more stress, particularly among parents.7 On the other hand, some studies found that remote work was associated with a reduction of psychological and physical stress,8 and a lower prevalence of depression when the amount of teleworking is less than eight hours per month.9
Regarding work productivity, working from home was associated with decreased productivity.10 Another study demonstrated relationship between working from home and increased presenteeism.8 However, studies on health-related productivity loss (HRPL) are limited, with a significant lack of evidence focusing on Korean workers. Thus, our study aimed to examine the association between working from home and HRPL among Korean workers using the Work Productivity and Activity Impairment Questionnaire: General Health version (WPAI:GH), which measures HRPL as the sum of presenteeism and absenteeism. Furthermore, stratified analyses on various dimensions including basic demographics, occupational factors and life style, which are known to influence HRPL,1112 were conducted to determine the subgroups that were significantly associated with working from home and HRPL.
METHODS
Study participants
The target population was waged workers in Korea, aged ≥ 19 years. Data were collected in September 2021 using a web-based questionnaire through an online panel survey service (Data Spring Korea Inc., Seoul, Korea). A total of 1,078 participants completed the questionnaires. The respondents were all individuals who agreed to participate in the survey, resulting in a 100% response rate. The survey incorporated questions about basic demographic information (gender, age, education level, and marital status), health status, lifestyle and working environment including whether they worked from home.
Measurement of variables
HRPL
There are several methods for measuring HRPL, including the effect of health on presenteeism and absenteeism.13 Among them, the WPAI:GH was used in this study. The WPAI:GH consists of six questions that ask about current employment status, hours missed due to health problems (Q2), hours missed due to other reasons (Q3), hours actually worked (Q4), the degree to which health affected productivity while working (using a 0–10 numeric scale) (Q5), and the degree to which health affected productivity in regular unpaid activities (using a 0–10 numeric scale) (Q6). Absenteeism was calculated as the percentage of work time missed owing to health problems, which is Q2/(Q2+Q4) * 100. Presenteeism was calculated as the actual work time multiplied by the subjective amount of impairment while working due to health as perceived by workers, presented as a percentage, which is {1-Q2/(Q2+Q4)} * (Q5/10) * 100. The overall percentage of HRPL was calculated as the sum of absenteeism and presenteeism. The reliability and validity of the WPAI:GH have been established in prior research,14 and the Korean version was developed through independent translation, harmonization, and expert review.15
Work from home
Among the participants who answered yes to the question “Have you been working from home in the last 6 months?”, workers that worked from home more than 3 days a week were considered in the “work from home” group.
Covariates
Basic characteristics included gender, age (20–29, 30–39, 40–49, 50–59, 60 years–), education level (high school or less, college or university, and graduate school), marital status (single, married, separated, widowed, and divorced), and health status (diagnosis of chronic diseases including hypertension, diabetes, hyperlipidemia, angina or myocardial infarction, stroke or other cerebrovascular disease, major depressive disorder, anxiety disorder and cancer). We chose to use the term gender rather than sex to emphasize the sociological meaning. Monthly income was inquired and divided into four groups of equal size using quartiles.
The Korean Standard Classification of Occupations was used to survey occupations. Managers, professionals and related workers and office workers were classified as white collar; clerks, service workers and sales workers were classified as pink collar; and skilled agricultural, forestry and fishery workers, craft and related trades workers and equipment, and mechanic operating and assembling workers were classified as blue collar. Although blue-collar workers are commonly perceived to be unable to work from home, according to the report for “Guideline Development for Establishing a Healthy Telecommuting Environment” by the Korea Occupational Safety and Health Agency,16 19.2% of manufacturing workers and 3.7% of transportation workers reported working from their own home. Furthermore, based on the “Excellent Utilization Cases of Working from Home, 2022” issued by the Ministry of Employment and Labor,17 it is evident that even production workers in the manufacturing sector were able to work from home. There were some approaches such as receiving work materials at home, processing or producing products, and then sending the final products to the workplace, and adjusting equipment or facilities at home. Therefore, we decided to include blue collar workers for our study.
The question regarding working hours was asked in the form of h/week, and grouped as follows: < 40, 40 ≤ and < 52, and 52 ≤. Other lifestyle-related variables included presence of preschool children at home, living alone, living in a studio apartment (one room), commuting time, and regular exercise. Commuting time was categorized into three groups: less than 1 hour, between 1 hour and 2 hours, and more than 2 hours.
Covariates including basic demographic characteristics were selected based on previous research,1112 and those are work-related factors such as working hours and occupational category, and individual factors such as health condition and lifestyle.
Statistical analysis
Basic demographic characteristics were analyzed using the χ2 test according to whether the participants were working from home. Generalized linear models utilizing identity function were used to compare HRPL between the two groups. The adjusted variables were gender, age, occupation, marital status, education level, income level, previous diagnosis of chronic disease, working hours, commuting time and living alone. Stratified analyses were conducted according to gender, age, income level, occupation, education level, previous diagnosis of chronic disease, presence of preschool children, living in studio apartments, living alone, commuting time, working hours and regular exercise. All statistical analyses were performed using SAS (version 9.4; SAS Institute, Cary, NC, USA), and p values < 0.05 were considered significant.
Ethics statement
This study was approved by the Institutional Review Board of the Seoul National University College of Medicine (C2107-253-1242).
RESULTS
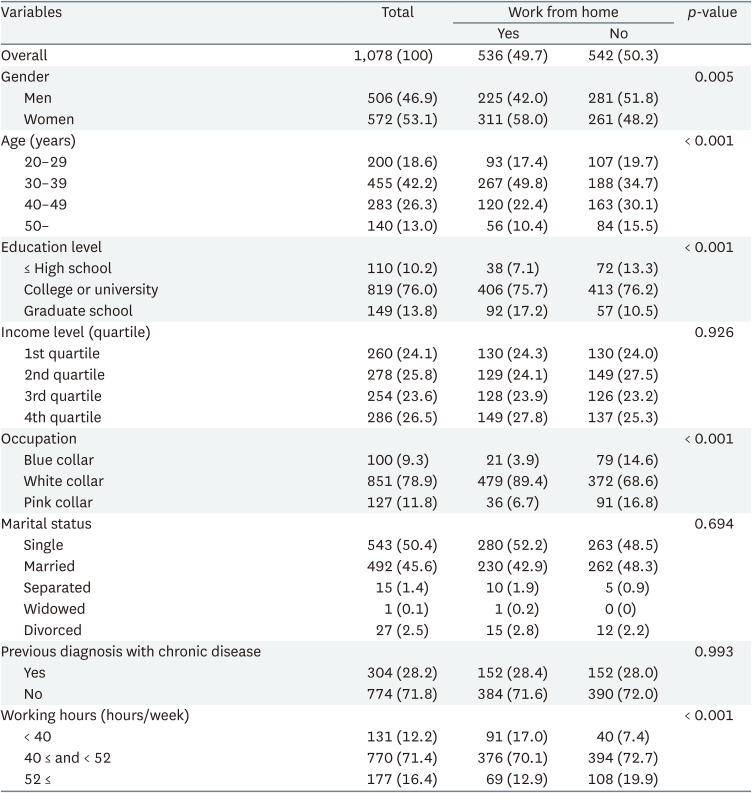
We recruited 536 workers that worked from home and 542 workers that commuted. The basic characteristics of the 1,078 participants including 506 men (46.9%) and 572 women (53.1%) are shown in Table 1. Of these, 536 (49.7%) were working from home and 542 (50.3%) were not. More women (58.0%) worked from home than men (42.0%). The majority of the workers who worked from home were aged 30–39 years (49.8%), graduated from college or university (75.7%), were white collar (89.4%), and worked 40–52 hours a week (70.1%). There were no significant differences in income levels, marital statuses or health statuses.
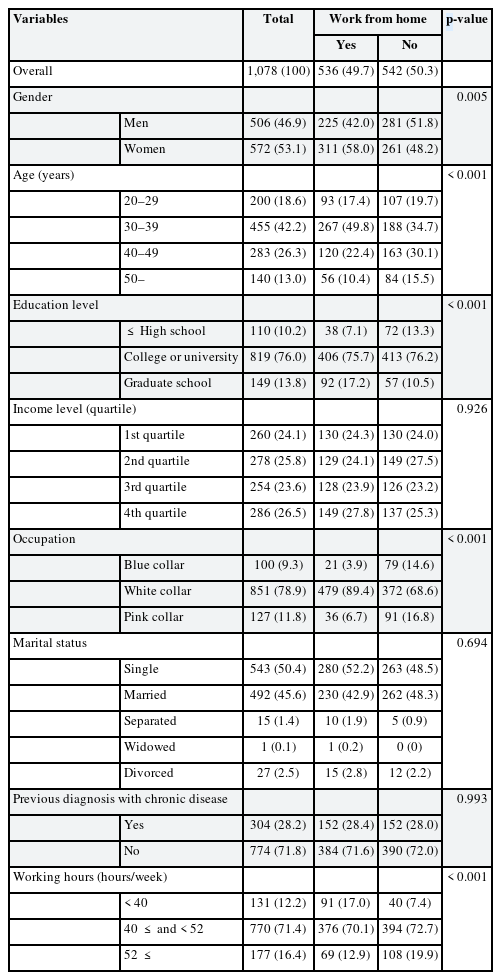
Baseline characteristics according to work from home
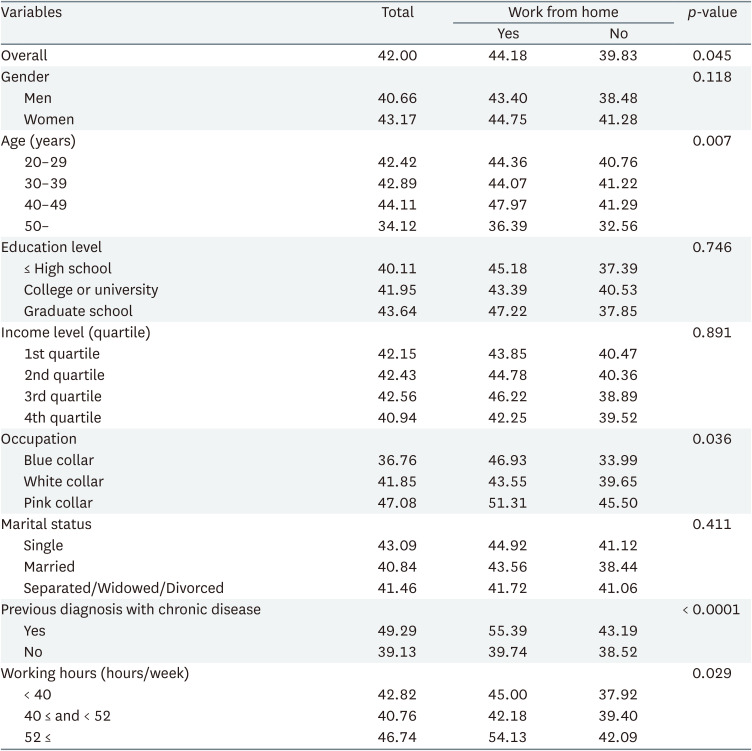
The mean HRPL of the participants was 42.00 (Table 2). The mean HRPL of the workers that worked from home was 44.18 and that of commuters was 39.83 (p = 0.045). Statistically significant differences were observed based on age (p = 0.007), occupation (p = 0.036), previous diagnosis with chronic disease (p < 0.0001), and working hours (p = 0.029).
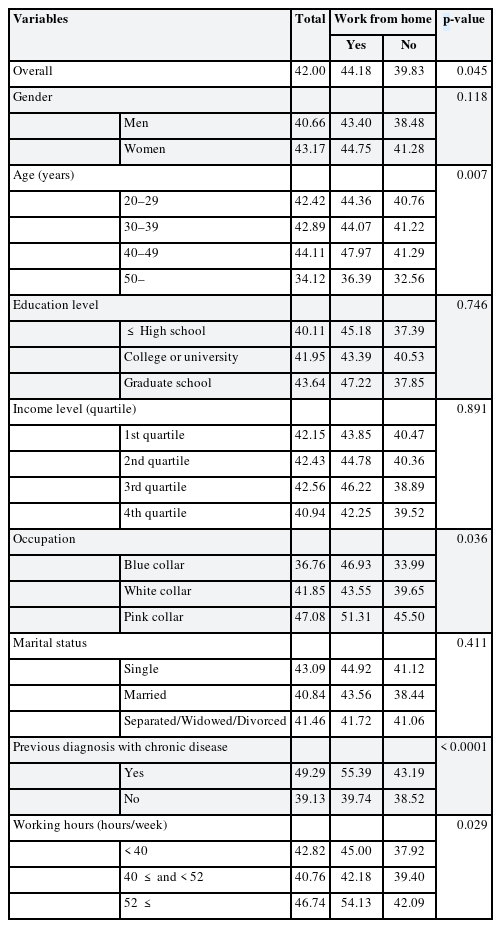
Mean HRPL according to work from home (%)
Table 3 shows the mean differences in HRPL between the two groups: (work from home) - (commuters). The results were presented as percentage and were adjusted for gender, age, occupation, marital status, education level, income level, previous diagnosis of chronic disease, working hours, commuting time and living alone. The mean difference of presenteeism and absenteeism were not statistically significant. In terms of overall HRPL, the mean difference was 4.05 (95% confidence interval [CI]: 0.09–8.01).
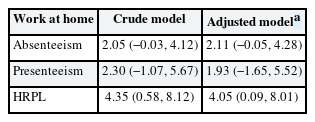
Mean differences (least square means) of health-related productivity loss according to work from home (95% confidence interval)
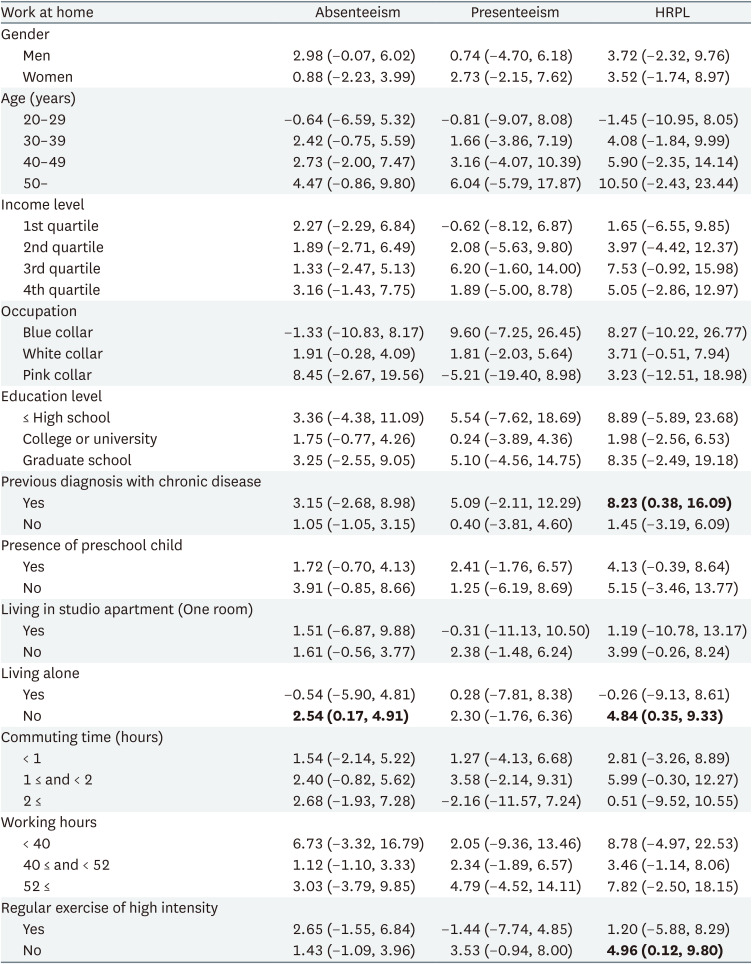
The results of the stratified analyses are presented in Table 4. The mean difference in absenteeism of workers who live with others was 2.54 (95% CI: 0.17–4.91). There were no significant differences in presenteeism in the stratified analyses. The overall HRPL was significantly different in the three subgroups: workers with chronic diseases (mean difference: 8.23, 95% CI: 0.38–16.09), workers living with others (mean difference: 4.84, 95% CI: 0.35–9.33), and workers that do not exercise regularly (mean difference: 4.96, 95% CI: 0.12–9.80). Mean differences in absenteeism, presenteeism and HRPL increased with age. The results of the stratified analyses are presented in Supplementary Fig. 1 as bar graphs.
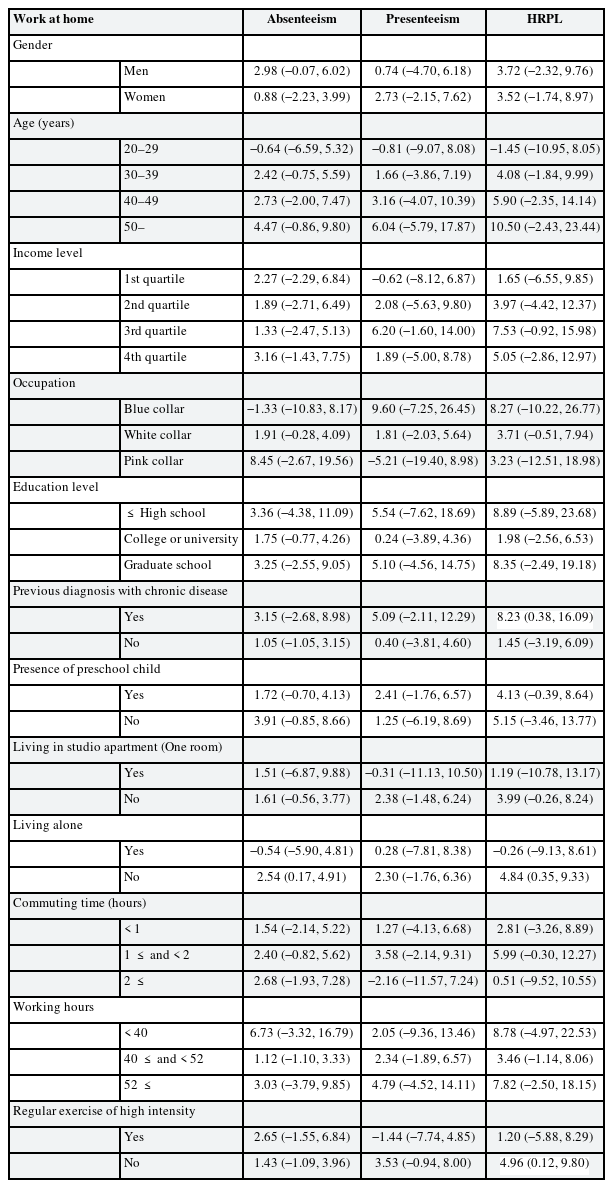
Stratified analyses of mean differences (least square means) of health-related productivity loss according to work from home (95% confidence interval)
DISCUSSION
This study explored the association between working from home and HRPL. Workers who work from home experience a 4% point higher HRPL than those who do not work from home. In the stratified analyses, the “work from home” group had a significantly higher HRPL than the “commuters” group among workers with chronic diseases, workers who did not live alone, and workers who did not engage in physical activity regularly. Although prior studies are not abundant and the results are inconsistent, it is more evident that there is a negative association between working from home and health or productivity18 and it is supported by the results of our study.
Some possible factors of working from home can result in a higher HRPL. The first is the lack of boundary between work and family or other private lives. Increased time spent at home can escalate family-work conflicts and lead to less productivity and more stress.19 Women experience more conflict than men, indicating a higher burden of housework and caregiving.20 A previous study has suggested that work-to-family conflict negatively affects work-related wellbeing, including emotional exhaustion and burnout.21 In addition, longer hours of working home were associated with role ambiguity, role conflicts and work-private life conflict.22 Elevated occupational stress owing to this conflict may be associated with increased HRPL.23 The results of our study, which observed a higher mean difference in HRPL among workers who did not live alone, are consistent with these previous findings. Workers who live alone face fewer barriers when working at home. However, workers with cohabitants can be interrupted by their families, especially those who require caregiving.
Another approach involves ergonomics. A prospective cohort study showed that lack of space for concentration, lack of sufficient light and foot space, and inadequate temperature and humidity impaired work function.24 Working from home, which is not specifically designed for work, leads to lower workstation ergonomic suitability, and to musculoskeletal symptoms.25 This was especially true for those who started working from home after the COVID-19 pandemic and did not have a fully prepared environment.
Third, working from home can lead to social isolation and increase work-related stress.19 The longer a person works from home, contact with colleagues naturally decreases and there is less social support from colleagues.22 This can result in various negative work outcomes, including increased burnout21 and stress due to psychological detachment.25
Working from home could abruptly change workers’ lifestyles by interfering with their daily routines. Workers who worked from home had a significantly higher risk of sleep disturbance26 and impaired sleep quality.27 In addition, teleworkers reported increased alcohol consumption,28 especially if they preferred to commute daily.29 These changes are explicit factors that can negatively affect both physical and mental health, and might have led to a higher prevalence of depression and anxiety among teleworkers.27
In the stratified analyses, workers with chronic diseases who did not exercise regularly had significantly higher mean differences in HRPL when working from home. A Japanese study proposed that people working from home had higher sedentary time and lacked physical activity during work, both light intensity and moderate-to-vigorous.30 This might be explained by the reduction in commuting, however, research on physical activity during daily trips on transportation can refute. Although non-commuting trips were greater among teleworkers, the total amount of physical activity on daily trips was less than that of non-teleworkers before, during and after COVID-19.31 This indicates that teleworkers must engage in extra physical activity to replace the amount ensured by commuting trips. Working from home is not only associated with decreased physical activity during worktime but also with decreased physical activity overall.32 This decline in physical activity is more harmful to people who do not exercise voluntarily. Additionally, an increase in sedentary time can aggravate chronic diseases.33 It has also been stated that sudden workstyle changes due to COVID-19 and teleworking are associated with loss of health consciousness, which means that people care less about their chronic condition.31
It was also noted that the difference in HRPL owing to teleworking was higher in the older age group. One study demonstrated that older age is associated with lower job performance when teleworking.34 This might indicate that older workers struggle more adapt to working from home, which can lead to a higher HRPL. In fact, older workers felt more discontent when working from home. In a survey evaluating work efficiency, older employees were likely to highlight disadvantages,35 and they perceived themselves as being less competent in technological aspect.36 The experience of frustration due to low professional self-efficacy can lead to higher level of work stress and exhaustion.37
This study is the first in Korea to investigate the relationship between working from home and HRPL, and our overall findings are consistent with those of earlier studies from other countries. One of the limitations of our study was that it was cross-sectional, thus no causal relationships could be established. Furthermore, it should be considered that a significant number of workers started working from home because of the physical distancing policy implemented after COVID-19. Workers who were teleworking before the pandemic and had more autonomy to choose where to work, were less likely to report the disadvantages of working from home.38 Owing to a lack of information, our study cannot shed lights on the difference between voluntary and non-voluntary teleworkers; therefore, further research is needed.
CONCLUSIONS
Our study suggests that working from home is associated with a high HRPL and the difference is greater in workers with chronic diseases, those living with others, and those who do not exercise regularly. We also found that older teleworkers exhibited greater differences in HRPL. As working from home has widely expanded in many workplaces even after the pandemic, it is important to pay attention to the health and HRPL of teleworkers. Employers should be careful not to compromise teleworkers’ health outcome, by securing a proper home environment or promoting communication. Workers may have to maintain a separate workspace at home, to divide work from private life, especially if they have cohabitants. Workers with old age, chronic diseases and lack of physical activity, who are the more vulnerable group, should be more mindful of their health and lifestyles.
Notes
Funding: This research is supported by National Research Foundation of Korea (NRF-2022R1F1A1066498).
Competing interests: The authors declare that they have no competing interests.
Author Contributions:
Conceptualization: Kang MY.
Data curation: Lee DW, Hong YC.
Formal analysis: Kim HJ.
Validation: Kang MY.
Visualization: Kim HJ.
Writing - original draft: Kim HJ.
Writing - review & editing: Lee DW, Choi J, Kang MY.
Abbreviations
CI
confidence interval
COVID-19
coronavirus disease 2019
HRPL
health-related productivity loss
WPAI:GH
Work Productivity and Activity Impairment Questionnaire: General Health version
References
SUPPLEMENTARY MATERIAL
Supplementary Fig. 1
Stratified analyses of mean differences of health-related productivity loss according to work from home. Absenteeism and presenteeism (%) are presented as bars. 95% confidential intervals are presented as black lines. Adjusted by gender, age, occupation, marital status, education level, income level, previous diagnosis with chronic disease, working hours, commuting time and living alone.