Association between shift work and serum homocysteine level in female electronic manufacturing services workers
Article information

Abstract
Background
Shift work has been shown to increase the risk of cardiovascular disease (CVD) based on several evidences. The classic risk factors of CVD include age, hypertension, smoking, obesity and diabetes. Recently, the serum homocysteine level has been reported to be a valuable indicator of CVD risk. This study aimed to determine the variation in serum homocysteine level as a cardiovascular risk indicator among female workers according to shift work.
Methods
The data of regular health examination of workers at an electronic manufacturing services company in Yeongnam region, South Korea in 2019 were examined in this study. The investigation was based on a cross-sectional study conducted on 697 female workers (199 day workers and 498 shift workers). The sociodemographic and biochemical characteristics were compared between day workers and shift workers. Through a logistic regression analysis, the odds ratio (OR) of the increased serum homocysteine level in relation to shift work was determined.
Results
Compared to female day workers, female shift workers showed significantly higher level of serum homocysteine (8.85 ± 2.16 vs. 9.42 ± 2.04 μmol/mL; p = 0.001). The OR of day workers against shift workers was 1.81 (95% confidence interval [CI]: 1.25–2.63). With the adjustment of variables that may influence the level of serum homocysteine, the adjusted OR was 1.68 (95% CI: 1.09–2.60).
Conclusions
The serum homocysteine level was significantly higher in shift workers than in day workers. It is thus likely to be a useful predictor of CVD in shift workers.
BACKGROUND
Cardiovascular disease (CVD) shows the second highest mortality after cancer among chronic diseases in South Korea.1 The known CVD risk factors are hypertension, smoking, abdominal obesity, dyslipidemia and diabetes as well as excessive stress, lack of exercise and sleep disorder.2 Among these factors, insomnia or hypersomnia may be caused by shift work, and despite insufficient data to define shift work as an independent factor, the CVD risk is known to increase in shift workers.2
Shift work can be defined in 2 ways: narrow and broad. In a narrow sense, shift work refers to a method of arranging working hours in which workers work continuously in shifts with the goal of increasing total working hours.3 4 In a broad sense, it refers to all forms of work in non-weekly working hours, which are hours other than weekly working hours, regardless of shifts.4 5 In this study, we will use the term shift work in a narrow sense.
Several studies have reported the association between shift work and the various CVD risk factors. Bøggild et al.6 reviewed 17 studies to show that shift work could increase the CVD risk by 40%, and in Torquati et al.,7 the CVD risk in shift workers was approximately 20% higher than in day workers with the risk increasing by 7% on average after 5 years of exposure to shift work.
The level of serum homocysteine is known to be a useful indicator of CVD risk and in the review by Humphrey et al.,8 an increase in serum homocysteine level by 5 μmol/mL was shown to increase the CVD risk by 20%–50% in most of the 26 reviewed studies. In Wald et al.,910 where a meta-analysis was performed on genetic and prospective cohort studies, an increase in serum homocysteine level by 5 μmol/mL led to a significant increase in CVD risk, but when the level of serum homocysteine was decreased by 3 μmol/mL through the intake of folic acid, for example, the risks of ischemic heart disease, deep vein thrombosis and stroke were predicted to fall by 16%, 25% and 24%, respectively.
Based on these findings, the serum homocysteine level can be regarded as a valuable predictor of CVD risk. Of note is that the serum homocysteine level could be higher in shift workers than in non-shift workers as shift workers are more susceptible to CVD. In Kang et al.,11 a study on the workers at a steel manufacturing company in South Korea, the serum homocysteine level was shown to be significantly higher in male shift workers with a certain length of work than in male day workers. However, no study has yet reported on the correlation between serum homocysteine level and CVD risk of female workers in South Korea. Another study conducted in South Korea on the reference level of serum homocysteine in males and females, reported that the reference level in females was lower than in males by approximately 5 μmol/mL.12 This implies that the serum homocysteine reference level applied in females should differ from that in males. In this study, therefore, a different serum homocysteine level(10 μmol/mL) compared to existing pathological reference value (15 μmol/mL) was applied in comparing female shift workers and female non-shift workers with respect to the serum homocysteine level, with an aim to determine the association between the serum homocysteine and the CVD in female shift workers.
METHODS
Subjects
In this study, the data of 2,779 workers at an electronic manufacturing services (EMS) company in Yeongnam region, South Korea, who received a health examination including the test of serum homocysteine level at a university hospital in Changwon, Yeongnam region between January 1, 2019 and December 31, 2019, were collected. As the study aimed to determine the association between the serum homocysteine level and shift work in female workers, 2,703 male workers were excluded. From the data of 706 female workers, those holding missing values were excluded (n = 9). The final set of data included the data of 697 female workers to perform a correlation analysis on the serum homocysteine level and shift work. The subjects in this study thus comprised 199 day workers and 498 shift workers.
Among the participants, day workers worked from 8:00 am to 5:00 pm from Monday to Friday, and can adjust their working hours through voluntary work adjustment within 52 hours per week. Shift workers work 4 days a week, 2 days off, 4 nights work, 2 days off. The day shift and night shift were from 8:00 am to 8:00 pm and from 8:00 pm to 8:00 am, respectively.
General characteristics
For sociodemographic factors, the age, marital status, education, drinking, smoking and regular exercise were investigated. The marital status was categorized into married and others (unmarried, divorced or bereaved). The level of education was divided into ≤ high school and ≥ college degree. The level of alcohol drinking was categorized into drinker (≥ once a week) and non-drinker (< once a week). In the case of men, the mortality rate due to drinking significantly increased when the amount of alcohol was 100 g or more per week and less than that in the case of women.13 Since the amount of alcohol consumed was not accurately measured, drinkers were defined based on the number of times of drinking. The level of smoking was categorized into current smoker and current non-smoker. Current smokers are classified as such because they are known to have a generally increased risk of CVD compared to non-smokers.14 The subjects were also divided between regular exercise group (≥ 3 times a week) and non-regular exercise group (< 3 times a week). Exercising for 30 to 60 minutes at least 3 times a week is known to be effective in reducing CVD risk.15 Due to the limitations of the questionnaire, the exercise time was not accurately known, so it was classified as above.
Serum homocysteine level
Hyperhomocysteinemia is generally diagnosed based on 15 μmol/mL of serum homocysteine.16 However, as the level of serum homocysteine is lower in females than in males with a trend of increase as age increases, and considering that 15 μmol/mL of serum homocysteine indicates the need for disease treatment, 10 μmol/mL was determined suitable for screening, which was thus set as the uppermost level of serum homocysteine in this study. The criteria for the serum homocysteine level was set to 10 μmol/mL in this study in reference to various studies. In a study analyzing the data of 809 healthy Korean individuals to estimate the reference level of serum homocysteine in males and females, the upper limit was reported to be 19.21–19.76 μmol/mL in males but 14.99–15.16 μmol/mL in females.12 In another study, the level of serum homocysteine was higher in individuals of higher age groups when compared before and after the intake of folic acid supplement.17 In this regard, it seems more plausible to apply a level lower than the conventional 15 μmol/mL for it to function as a CVD indicator for younger female workers. In a study conducted on healthy undergraduate students at a university in Portugal with respect to the reference range, a level above or equal to 11.6 μmol/mL was reported to necessitate a follow-up monitoring.18 In a prospective study on the risk of cardiac infarction in relation to serum homocysteine, a level of approximately 10 μmol/mL was reported to show a significant variation.19 In another study conducted on CVD patients rather than healthy individuals, the reference level of 9.0 μmol/mL was shown to increase the mortality across all following ranges; 9.0–14.9 μmol/mL, 15.0–19.9 μmol/mL and ≥ 20 μmol/mL. In a cell culture study, although the results may not apply in the human body, a level above or equal to 10 μmol/mL was shown to mediate the generation of reactive oxygen species (ROS), a cause of atherosclerosis.20 Based on the findings of these diverse studies, the criteria for the serum homocysteine level in this study was set to 10 μmol/mL as a level suitable for the screening across younger female adults.
Statistical analysis
To compare the general, psychiatric and biochemical characteristics between shift workers and day workers, t-test and chi-square test were used. To analyze the linear relationship between the serum homocysteine level and the CVD risk factors, a partial correlation analysis was performed with adjustment for age, which is known to be positively correlated with the level of homocysteine in general. To identify the odds ratio (OR) of the group of high serum homocysteine level according to work type, a logistic regression analysis was performed with adjustment for potential confounders between shift work and serum homocysteine. The confidence interval (CI) and significance level were set to 95% and p < 0.05, and the IBM SPSS Statistics for Windows version 25.0 (IBM Corp., Armonk, NY, USA) was used as a statistical program.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Samsung Changwon Hospital before implementation (approval No. SCMC 2022-08-013) and waived the requirement for informed consent. This was due to the use of anonymized data that were routinely collected as part of a health checkup program.
RESULTS
General characteristics of the subjects
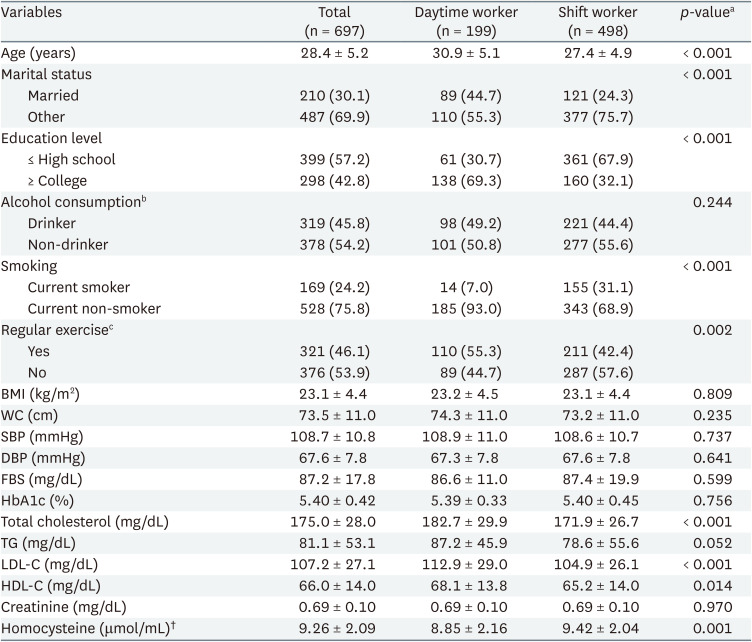
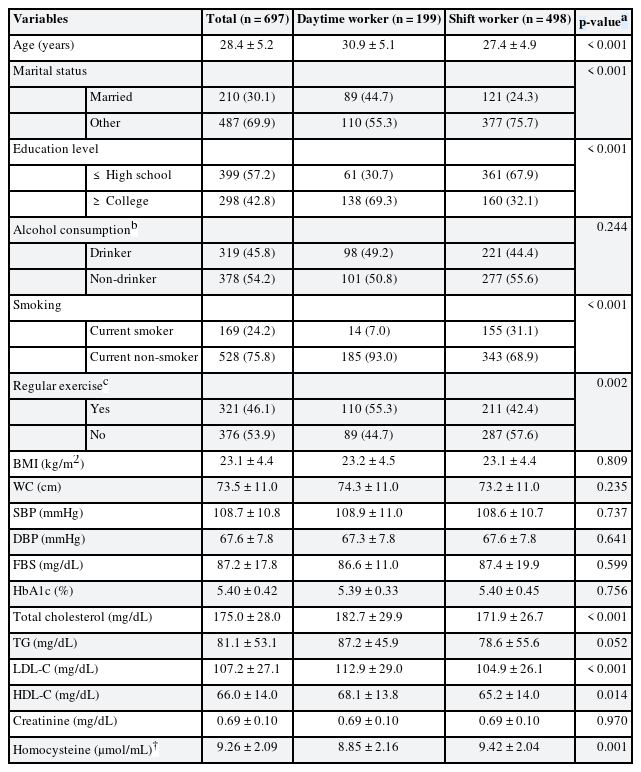
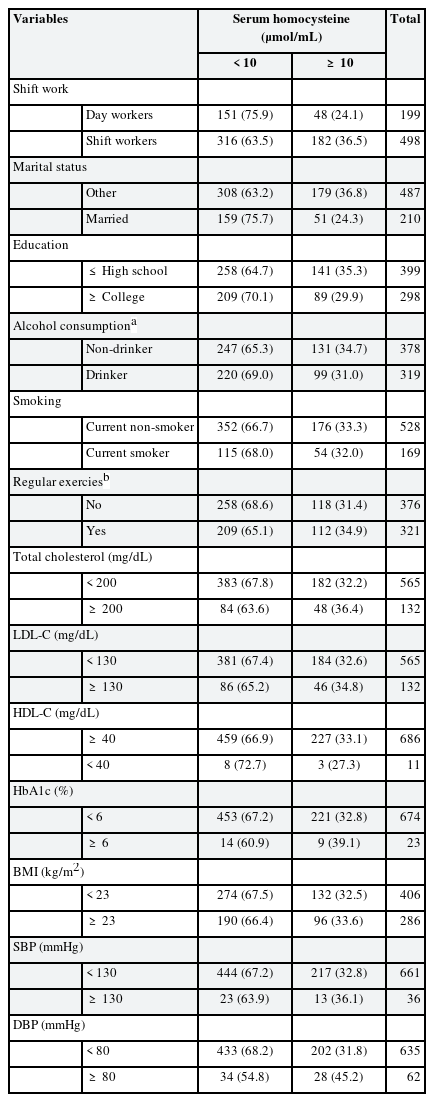
Among the 697 subjects, 498 were shift workers (71.4%) and 199 were day workers (28.6%). The mean age of day workers was 30.9 ± 5.1 years, which was significantly higher than shift workers at 27.4 ± 4.9 years (p < 0.001). The percentage of married was significantly higher in day workers (44.7%) than in shift workers (24.3%) (p < 0.001). The percentage of ≥ college degree was significantly higher in day workers (69.3%) than in shift workers (32.1%) (p < 0.001). The percentage of current smokers was significantly higher in shift workers (31.1%) than in day workers (7.0%) (p < 0.001). Between day workers and shift workers, the measurements of body mass index (BMI), waist circumference (WC), systolic blood pressure (SBP), diastolic blood pressure (DBP), fasting blood glucose (FBS), glycated hemoglobin (HbA1c), triglyceride (TG) and creatinine, did not vary significantly. The total cholesterol (182.7 ± 29.9 vs. 171.9 ± 26.7, p < 0.001), low-density lipoprotein cholesterol (LDL-C, 112.9 ± 29.0 vs. 104.9 ± 26.1, p < 0.001) and high-density lipoprotein cholesterol (HDL-C, 68.1 ± 13.8 vs. 65.2 ± 14.0, p = 0.014) were significantly higher in day workers, while the serum homocysteine level was significantly higher in shift workers (9.42 ± 2.04 μmol/mL) than in day workers (8.85 ± 2.16 μmol/mL) (p = 0.001) (Table 1). For additional information, the general characteristics of the subjects and their relationship with homocysteine were tabulated (Table 2). Detailed distributions for continuous variables are attached through the Supplementary Fig. 1.
General characteristics of the subjects
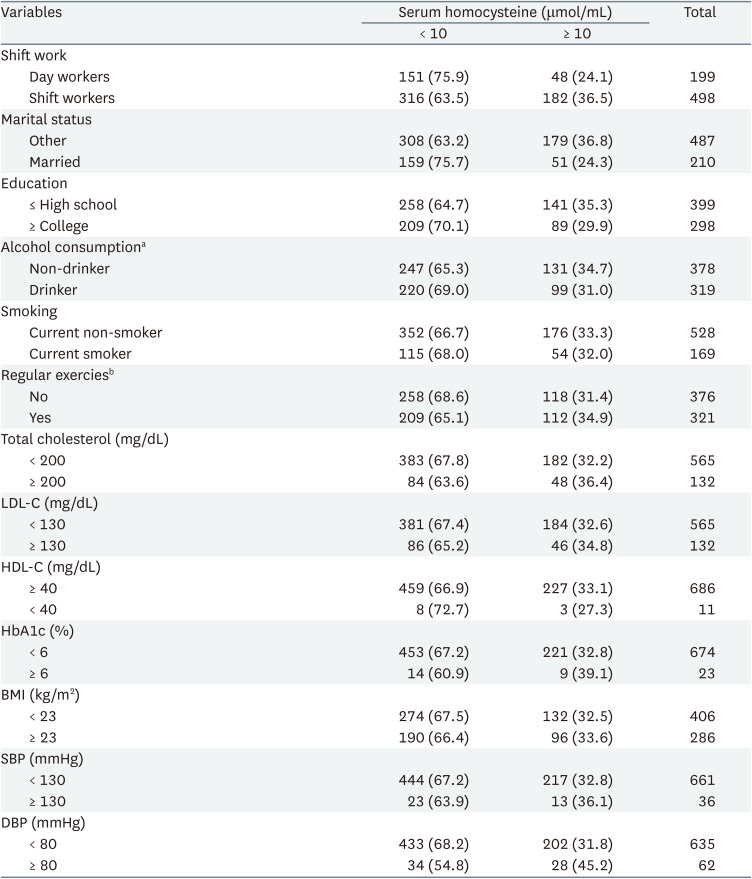
Relationship between subject’s serum homocysteine and general characteristics
Correlation between serum homocysteine level and study parameters
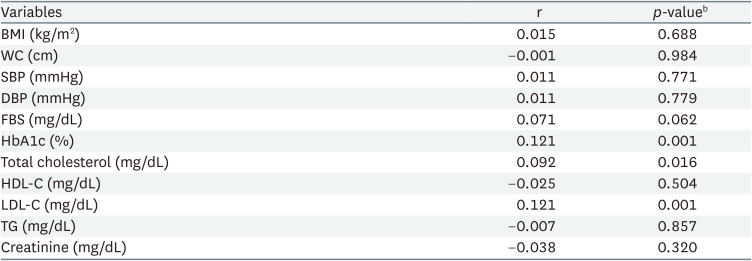
The partial correlation analysis with adjustment for age showed a positive correlation of the serum homocysteine level with HbA1c, LDL-C and total cholesterol as the CVD risk factors. No correlation was found for BMI, WC, SBP, DBP, HDL-C, TG (Table 3).
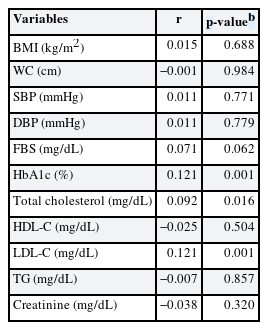
Correlation of homocysteine with clinical or biochemical parametersa
Comparison of serum homocysteine levels by age
Age is an important risk factor for CVD. In this study, subjects were classified according to shift type, and there was an age difference between groups. To better assess the effect of age on serum homocysteine levels, we compared homocysteine levels by age independent of shift status. Since all workers belonged to the age group of 19 to 39, they were categorized into 4 groups at 5-year intervals and compared. 175 were 19–24 years old, 272 were 25–29, 133 were 30–34, and 117 were 35–39. In serum homocysteine level by age, the age group of 19–24 (10.0 ± 2.2) was higher than that of the age group of 35–39 (8.7 ± 1.9, p < 0.001), and the probability of belonging to the serum homocysteine group of 10 or more was also higher in the younger group (p < 0.001). Contrary to general perception, the older the age, the lower the homocysteine level (Table 4).
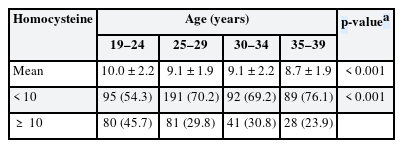
Comparison of serum homocysteine levels according to age group
Logistic regression model for high serum homocysteine level by work type
The logistic regression analysis taking the day workers as the reference to analyze the increase in serum homocysteine level and shift workers, showed a significant variation based on OR 1.81 (95% CI: 1.25–2.63). In model 1 with adjustment for age which considered to be the most important confounding variable, the estimated OR was 1.56 (95% CI: 1.06–2.31). In model 2 with additional adjustments for the general characteristics that exhibited significant variations between shift workers and day workers in model 1; alcohol consumption, marital status, education, smoking and regular exercise the estimated OR was 1.60 (95% CI: 1.04–2.46). In model 3 with the adjustments for BMI, SBP, DBP, HbA1c and LDL-C, the factors that can cause CVD as a complication in model 2, the OR was 1.68 (95% CI: 1.09–2.60) (Table 5).

Logistic regression model of high homocysteine according to work typea
DISCUSSION
In this study, female shift workers showed a significantly higher serum homocysteine level than female day workers. The lifestyle factors previously reported to be related to CVD in shift workers (unmarried,21 low education level,22 smoking23 and insufficient exercise24) were shown to have a role to increase the level of serum homocysteine, but even after the adjustments for these variables, the serum homocysteine level was high in shift workers. The level was also high after the adjustments for BMI, SBP, DBP, HbA1c and LDL-C, the known risk factors of CVD. Compared to day workers, shift workers showed a significantly higher serum homocysteine level, while the biochemical markers that may serve as additional CVD risk factors either did not vary significantly (BMI, WC, SBP, DBP, FBS, HbA1c and TG) or was significantly lower in shift workers (total cholesterol and LDL-C). The level of HDL-C was significantly lower in shift workers although at a minimum variation (68.1 ± 13.8 vs. 65.2 ± 14.0 mg/dL). Considering the mechanism of serum homocysteine causing atherosclerosis, it is possible that the level of serum homocysteine could serve as an indicator of CVD risk at an earlier time than other indicators, which coincides with the result that only the serum homocysteine level varied between shift workers and non-shift workers. This suggests that, with shift work as a known risk factor of CVD, the serum homocysteine level may be a more practical CVD indicator than other quantitative markers.
Age is a factor known to be positively correlated with the incidence of CVD. Aging causes hypertension, changes in lipid metabolism, and increased insulin resistance through changes in various molecular units, which are factors that cause CVD through atherosclerosis. In addition, aging causes an increase in heart weight and a decrease in the number of cardiomyocytes, lowers the threshold of myocardial necrosis, and increases the possibility of CVD.2526 Age is an important factor in CVD, but in this study, older age groups showed lower plasma homocysteine results. Therefore, it is possible that the low ratio of shift work may have acted as a confounding factor.
Among the previous studies reporting similar results are the aforementioned study by Kang et al.11 as well as others on the correlation between shift work and the serum homocysteine level. In Martins et al.,27 a study conducted on 30 Brazilian shift work bus drivers and 22 control subjects, the serum homocysteine level was significantly higher in shift workers than in the control (18.57 vs. 9.43 μmol). In Zhang et al.,28 a study comparing night shift workers and non-night shift workers across 6,846 steel manufacturing workers in China, the OR on the probability of hyperhomocysteinemia with a 15 μmol/mL or higher level of serum homocysteine, was higher in night shift workers (1.23, 95% CI: 1.06–1.44), while the level of serum homocysteine significantly increased according to the length of night shift work.
Other studies reported deviating results, including Copertaro et al.,29 a study comparing the serum homocysteine level between 30 shift work nurses and 28-day work nurses, where there was no significant variation. This seems largely due to the insufficient number of study subjects.
Among the biochemical mechanisms driving serum homocysteine to induce CVD is the facilitated thrombogenesis to cause atherosclerosis. Serum homocysteine is known to stimulate the platelet generation for thromboxane A2 to facilitate the coagulation to cause thrombogenesis30; the level of coagulation is increased as factor V is activated through the activation of protein C and suppression of thrombomodulin expression, and the DNA synthesis is inhibited to downregulate the activities of anticoagulants.31 Another mechanism involves the generation of ROS. The auto-oxidized sulfhydryl groups of homocysteine react with the nitric oxide in endothelial cells to facilitate the ROS production. A high level of serum homocysteine reduces the ability of the key glutamate-cysteine ligases in the production of glutathione that removes ROS so as to interfere with the glutathione production.32 Other mechanisms are related to endothelial cells and smooth muscle cells. Hyperhomocysteinemia is known to facilitate the generation of smooth muscle cells in the endothelium of blood vessels and the irregular production of extracellular matrix collagen. The homocysteine in blood induces endothelial cell detachment, which is fatal to such cells. At a level of pathological significance, homocysteine stimulates the interaction between the neutrophils and the endothelial cells that induce the migration of neutrophils, in a way that resembles the inflammatory process.33 In addition, hyperhomocysteinemia causes hyperuricemia, which increases the levels of ROS that deteriorate the functions of endothelial cells.34 This process leading to atherosclerosis can induce or aggravate CVD.
Some studies reported on the pathogenesis of CVD in relation to shift work. In Puttonen et al.,35 shift work was shown to increase the risk of CVD through psychosocial, behavioral and physiological mechanisms. The psychosocial mechanism is related to the difficulty of controlling work hours, the reduced balance between work and life and the insufficient recovery after work. The most well-known examples of behavioral change are weight gain and smoking. The physiological mechanism involves the activation of the autonomic nervous system and the changes related to inflammation, lipid and glucose metabolism, atherosclerosis, metabolic syndromes and type II diabetes. On the other hand, Aisbett et al.36 showed that shift work was associated with sleep deprivation as well as type II diabetes, weight gain, CVD and cancer. These findings may provide the theoretical ground for the association between shift workers and high serum homocysteine levels.
Hyperhomocysteinemia is known to arise in patients with end-stage renal disease, who require dialysis or kidney transplantation.37 With the reduction in renal functions, hyperhomocysteinemia tends to occur because the kidneys have a critical role in the processing of homocysteine.38 In this study, the level of creatinine was measured to identify renal disease. No significant difference was found between shift workers and day workers, while no correlation with the serum homocysteine level was found. Considering that the creatinine level was normal across all subjects, the impact on homocysteine may only apply in individuals with a problem of clearance due to renal disease.
There are several limitations in this study. First, as a cross-sectional study, the cause-effect relation could not be identified, for which a follow-up prospective study should be conducted on a large-scale cohort. Second, the data of sociodemographic characteristics were obtained solely through a questionnaire, which implies potential inaccuracy of data. Third, the negative influencing factors that are exposed due to the differences in work between day workers and shift workers could not be analyzed. For example, since there is no information on working hours, length of service, and occupation, harmful factors may affect serum homocysteine, which may act as a confounding factor, and care should be taken in interpreting the results. Fourth, while the risk of congestive heart failure, senile macular degeneration, Alzheimer’s dementia, hearing impairment, or cancer and the intake of folic acid are known to be associated with the serum homocysteine level, these factors were not analyzed in this study, implying their potential confounding effects.
Despite these limitations, the significance of this study lies in investigating the association between shift work in female workers in South Korea and the serum homocysteine level for the first time. The serum homocysteine level was significantly higher in shift workers than in day workers even after the adjustment for potential influencing factors of the serum homocysteine, which confirms the association between shift work and increased level of serum homocysteine. The correlation between the increased level of serum homocysteine and the onset of CVD has been reported in a multitude of studies, and the findings collectively suggest that the follow-up monitoring of serum homocysteine level in shift workers is likely to contribute in the early detection of CVD for these workers. Meanwhile, a prospective study should be conducted regarding the prediction of the risk of CVD based on the measurement of serum homocysteine level in shift workers.
CONCLUSIONS
In this study, a significant variation in the serum homocysteine level was found between female shift workers and female day workers, even after the adjustment for all other variables. In various previous studies, the cause-effect relation between the increased level of serum homocysteine and the onset of CVD has been verified. Thus, it is predicted that a follow-up monitoring of the serum homocysteine level would contribute in the early detection of CVD in shift workers.
Notes
Competing interests: The authors declare that they have no competing interests.
Authors contributions:
Conceptualization: Lim JW.
Data curation: Kim CW.
Formal analysis: Park HO.
Funding acquisition: Chung EY.
Investigation: Son J.
Methodology: Shin YH, Park SH.
Software: Choi SM.
Validation: Chae C.
Visualization: Lim JW.
Writing - original draft: Lim JW.
Writing - review & editing: Lim JW, Kim CW, Park HO.
Abbreviations
BMI
body mass index
CI
confidence interval
CVD
cardiovascular disease
DBP
diastolic blood pressure
EMS
electronic manufacturing services
FBS
fasting blood sugar
HbA1c
glycated hemoglobin
HDL-C
high density lipoprotein-cholesterol
LDL-C
low density lipoprotein-cholesterol
OR
odds ratio
ROS
reactive oxygen species
SBP
systolic blood pressure
r
correlation coefficient
TG
triglyceride
WC
waist circumference
References
SUPPLEMENTARY MATERIAL
Supplementary Fig. 1
Detailed distributions for continuous variables of study.