Association between discrimination in the workplace and insomnia symptoms
Article information

Abstract
Background
In Korea, little research has focused on the relationship between discrimination in the workplace and sleep health. Thus, this study aims to investigate the association between such discriminatory experiences and insomnia, a common sleep disorder, using Korean employees’ data.
Methods
This study used data from the 6th Korea Working Conditions Survey. Discrimination experiences due to age, ethnic background, nationality, race, sex, religion, disability, sexual orientation, educational level, hometown, and employment status were investigated. The Minimal Insomnia Symptom Scale estimated insomnia symptoms. The association between discrimination experience and insomnia symptoms were analyzed using survey-weighted logistic regression analysis.
Results
Based on experiences of discrimination over the past 12 months, insomnia symptoms were associated with discrimination experience due to religion (odds ratio [OR]: 3.70; 95% confidential interval [CI]: 1.58–8.69), sex (OR: 2.51; 95% CI: 1.87–3.37), age (OR: 2.30; 95% CI: 1.88–2.81), hometown (OR: 2.07; 95% CI: 1.44–2.97), employment status (OR: 1.69; 95% CI: 1.37–2.10), and educational level (OR: 1.67; 95% CI: 1.31–2.14). Furthermore, the prevalence of insomnia symptoms increased with the number of discrimination experiences.
Conclusions
In this study, discrimination experiences due to religion, sex, age, hometown, employment status, and educational level were significantly associated with insomnia symptoms. Furthermore, as the number of discrimination experiences increased, so did the prevalence of insomnia. Preventing workplace discrimination may improve workers’ sleep health.
BACKGROUND
Sleep is an essential component of human life, and ordinary people spend around one-third of their life asleep.1 The cumulative short- and long-term effects of sleep disorders have been shown to lower a person’s attention and concentration, leading to memory impairment, depression, and increased metabolic and cardio-cerebrovascular diseases.2 The most common type of sleep disorder is insomnia.3 It is characterized by difficulty initiating, maintaining, and/or resuming sleep when waking up early in the morning.456 The reported prevalence of insomnia is 5%–23% in Korea, 10%–50% in North America, and 10%–60% worldwide.789101112
Discrimination is defined in the Oxford English Dictionary as “unjust or prejudicial treatment of a person or group, esp. on the grounds of race, sex, sexual orientation, etc.”13 Discrimination comprises actions, practices, or policies based on the social group to which the discriminated person belongs.141516 People experience different kinds of discrimination in their lives. It can be more prevalent in vulnerable groups, negatively affecting their mental and physical health and increasing mortality rates.1718192021
Discrimination in the workplace can influence workers’ social activities and it can also negatively affect their sleep. The association between workplace discrimination and sleep disorders was previously investigated, particularly in the United States. The interrelation between racial/ethnic discrimination and sleep has been a topic of interest.2223242526 Although discrimination based on sex, age, and socioeconomic status is equally important, related studies are lacking and few previous studies, particularly in Korea, have reported this as their main focus.2223242526 Thus, this study aims to investigate the association between discrimination experiences in the workplace and insomnia symptoms using a large representative sample of employees in Korea.
METHODS
Study participants
This study utilized publicly available data from the 6th Korea Working Conditions Survey (KWCS) (https://oshri.kosha.or.kr/oshri/researchField/downWorkingEnvironmentSurvey.do) conducted by the Korea Occupational Safety and Health Agency. The survey was performed in 2020. The KWCS was compared to the European Working Conditions Surveys conducted by Eurofound, an EU-affiliated organization. The KWCS investigated work environment characteristics such as work type, employment type, occupation type, industry, risk factor exposure, and employment stability. The study participants were employees aged 15 years or older living in Korea at the time of the survey. A total of 50,538 people were surveyed from 17 districts nationwide. Of these, 38,518 employees were analyzed. We excluded self-employed persons without employees (n = 7,827), self-employed persons with employees (n = 2,444), and non-paid familial workers (n = 1,749).
Study variables
Insomnia symptoms
The Minimal Insomnia Symptom Scale (MISS) was used to estimate insomnia symptoms in the 6th KWCS. The MISS asks respondents to recall difficulty falling asleep, waking up repeatedly during sleep, and waking up with exhaustion and fatigue over the past 12 months.27 Respondents then selected how often they experienced each of these symptoms on the following scale: never (0 points), infrequently (1 point), several times a month (2 points), several times a week (3 points), daily (4 points), and no opinion or refused to reply. Participants choosing “no opinion” or “refused” were excluded from this study. The MISS score can range between 0 and 12 points. Patients with 6 or more points were considered to have insomnia symptoms.27
Discrimination
The 6th KWCS included 11 questions about discrimination experience in the workplace over the past 12 months. The questions asked about discrimination due to age, ethnic background, nationality, race, sex, religion, disability, sexual orientation, educational level, hometown, and employment status. Participants choosing “yes” were considered to have experienced discrimination, and those answering “no” were assumed to have no discrimination experience. Participants choosing “not applicable,” “no opinion,” or “refuse” were excluded from the analysis.
Covariates
Variables related to any of the insomnia symptoms were included in the analysis.28 These included sex, age, education level, income, employment status, occupation, weekly working hours, shift work, and self-rated health. Age groups were categorized as 15–39, 40–49, 50–59, and ≥ 60 years. Education level was categorized into middle school or lower, high school, and college or higher. By splitting monthly income into quarters, the income level was classed into the lowest, low-middle, high-middle, and highest quartiles. Employment status was categorized into regular, temporary, and daily. Occupation was categorized into professional & managerial, clerical (office work), sales & service, and manual. Weekly working hours were categorized into 1–34, 35–40, 41–52, 53–60, and > 60 hours. Shift work was investigated using the question “Do you work shifts?,” where respondents could answer “yes” or “no.” Self-rated health was based on the reply to “How is your general health?.” Participants choosing “very good” or “good” were considered to have no health problems, whilst those choosing “fair,” “poor,” or “very poor” were considered to have health problems. Participants choosing “no opinion” or “refuse” were excluded from the analysis.
Statistical analysis
Categorical characteristics of the study participants, discrimination experience, the prevalence of insomnia symptoms, and the number of discrimination experiences and insomnia symptoms are presented as numbers and percentages. Survey-weighted logistic regression analysis was performed to examine the relationships between discrimination experience and insomnia symptoms. The number of discrimination experiences and insomnia symptoms was analyzed using the Cochran-Armitage trend test. The unadjusted and adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were based on Models 1–3. Model 1 adjusted for sex, age, employment status, occupation, education, and income. Model 2 adjusted for the variables in Model 1, shiftwork, and weekly working hours. Model 3 adjusted for the variables in Model 2 and self-rated health status. Statistical analysis was performed using STATA 17.0 (StataCorp, College Station, TX, USA).
Ethics statement
This study used the publicly-available data from the KWCS and was approved by the Institutional Review Board of Dong-A (approval No.2-1040709-AB-N-01-202205-HR-029-020).
RESULTS
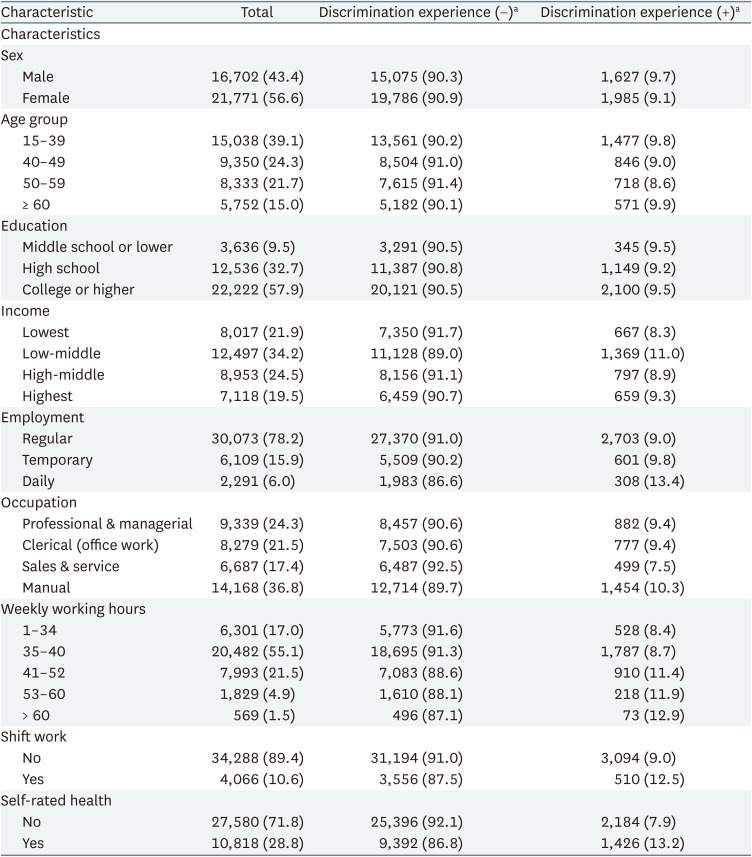
Table 1 shows the characteristics of the study participants. The proportion of male participants who experienced discrimination was higher than that of female participants (9.7% vs. 9.1%). Participants aged 15–39 (9.8%) and > 60 (9.9%) were more likely to experience discrimination than other age groups. The low-middle income group (11%) experienced more discrimination than the other income groups. Regarding employment status, 13.4% of the daily workers, 9.8% of the temporary workers, and 9.0% of the regular workers experienced discrimination. The highest proportion of workers experiencing discrimination were among the manual workers (10.3%). Discrimination was also higher among shift workers (12.5%) and those who thought they had health problems (13.2%) compared to their respective opposite groups. The proportion of workers experiencing discrimination increased with the number of weekly working hours.
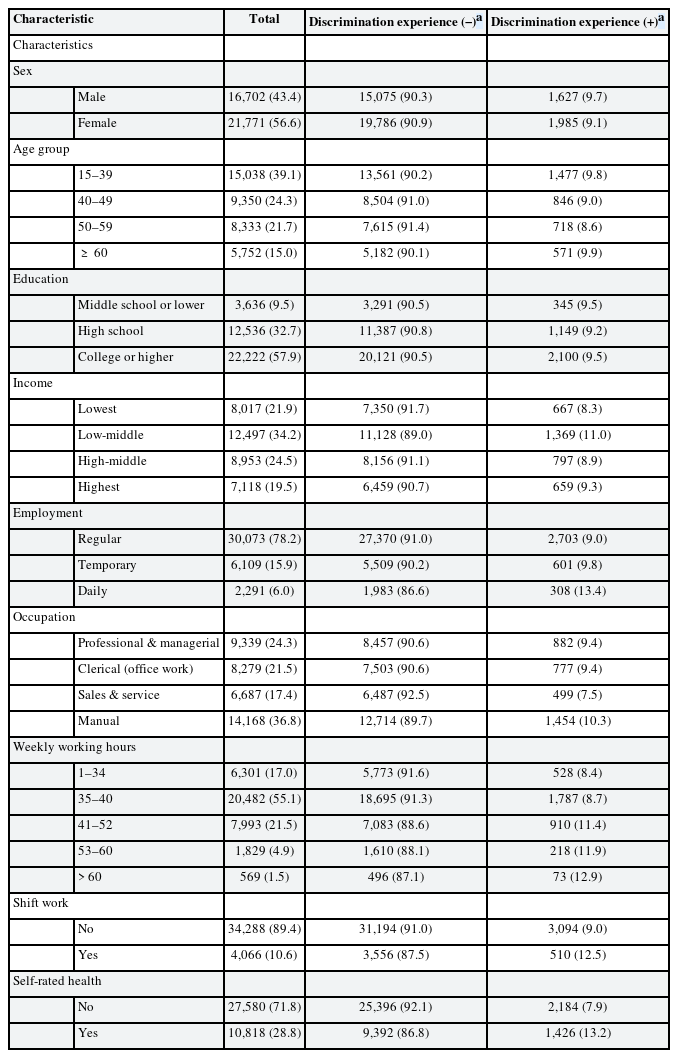
Characteristics of the study participants according to their discrimination experience
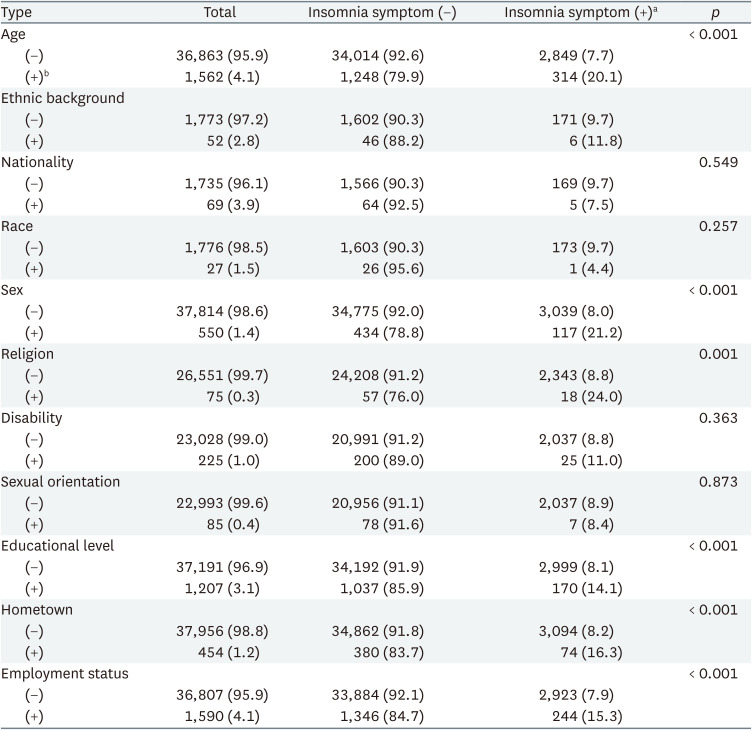
Table 2 presents the association between each discrimination experience and the prevalence of insomnia symptoms. Participants who experienced discrimination due to their age (20.1%), sex (21.2%), religion (24.0%), educational level (14.1%), hometown (16.3%), or employment status (15.3%) showed significantly more insomnia symptoms than those who were not discriminated against (p ≤ 0.001).
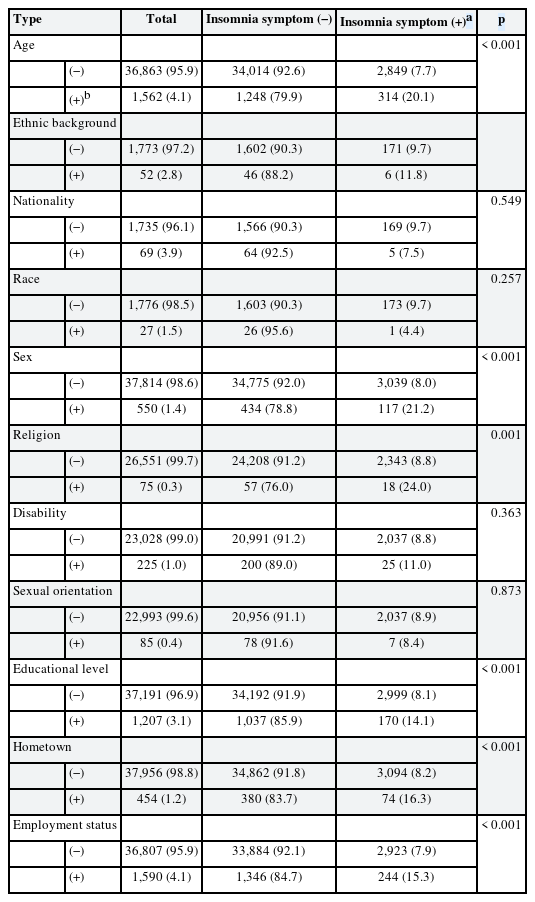
The association between each discrimination experience and the prevalence of insomnia symptoms
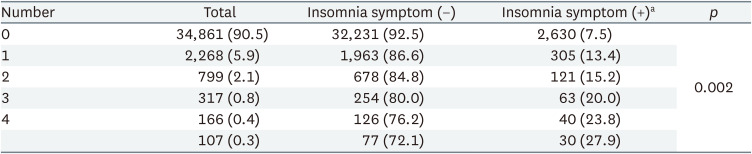
Table 3 shows the association between the number of discrimination experiences and the prevalence of insomnia symptoms. The table is composed of 6 rows, each of which corresponds to a different number of discrimination experiences, ranging from 0 to ≥ 5, and 2 columns, which indicate whether insomnia symptoms are present or not. The proportion of participants reporting insomnia symptoms increased as the number of discrimination experiences increased. For example, only 5.9% of participants with no discrimination experiences reported insomnia symptoms, compared to 27.9% of participants with 5 or more discrimination experiences.
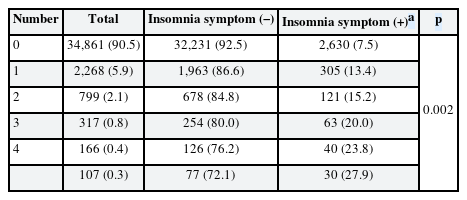
Numbers of discrimination experiences and insomnia symptoms
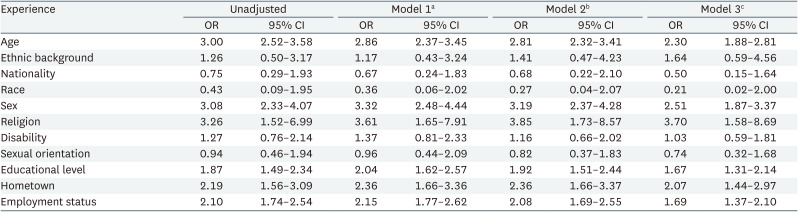
The association between the discrimination experience and insomnia symptoms by survey-weighted logistic regression analysis is shown in Table 4. Discriminations due to age, ethnic background, sex, religion, disability, educational level, hometown, and employment status were associated with insomnia symptoms regardless of whether the model was adjusted. Discrimination due to religion had the greatest influence on insomnia symptoms in Model 3 (OR: 3.70; 95% CI: 1.58–8.69), followed by discrimination due to sex (OR: 2.51; 95% CI: 1.87–3.37) and age (OR: 2.30; 95% CI: 1.88–2.81).
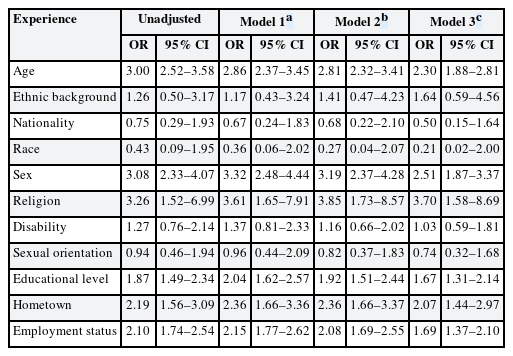
Association between discrimination experience and insomnia symptoms by survey-weighted logistic regression analysis
The association between the number of discrimination experiences and insomnia symptoms by survey-weighted logistic regression analysis is presented in Table 5. Excluding ≥ 5 experiences, the ORs showed an increasing pattern in adjusted models.
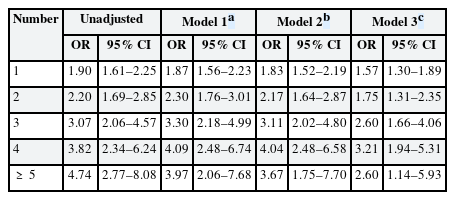
Association between the number of discrimination experiences and insomnia symptoms by survey-weighted logistic regression analysis
DISCUSSION
This study observed the association between discrimination in the workplace and insomnia symptoms by analyzing the 6th KWCS. Discrimination experiences due to religion, sex, age, hometown, employment status, and educational level were significantly associated with insomnia symptoms. Furthermore, as the number of discrimination experiences increased, so did the prevalence of insomnia.
A systematic review of articles published between 1971 and July 2014 on discrimination and sleep was reported in 2016.29 A total of 17 studies were included, and the association between organizational justice,303132 low income,31 race,333435363738 ethnicity,35363738394041 nationality,42 unfair treatment,43 job stress,44 sex,45 age,45 and sleep problems29 was examined. The association between discrimination based on sex,46 sexual orientation,474849 religion,50 disability,51 educational level,52 and sleep problems was identified in other studies published after 2014. There was only one paper on employment status based discrimination and sleep, but it was categorized according to whether or not the person was working, as opposed to our study, which was divided into regular, temporary, and daily workers.53 Studies on hometown (or regional) discrimination and sleep problems have not been identified.
The mechanism by which the prevalence of insomnia increases as the number of discrimination experiences increases is unknown. Perhaps the negative repercussions of experiencing discrimination, such as stress or depressive symptoms, increases resulting in these outcomes. In Table 5, when unadjusted, the OR increased as the number of discrimination experiences increased. However, when adjusted, the OR tended to drop when the number of discrimination experiences was greater than 5, and the gap tended to widen as the number of items of adjustment increased. Socioeconomic and occupational factors are likely to interact, and persons with poor socioeconomic and occupational factors are likely to rate their own health as poor. Consequently, this tendency may be partially explained by the fact that the attenuation effect increased as socioeconomic factors (employment status, occupation, education, income), occupational factors (shiftwork, weekly working hours), and self-rated health variables were adjusted in Models 1, 2, and 3.
A previous systemic review showed consistent results that discrimination experiences are associated with poorer sleep outcomes.29 A few prospective studies and a natural experiment also showed a relationship of temporal precedence.30313240 However, further clarity is required about the nuances of this connection.29 Studies on the direct mechanism by which discrimination affects sleep are lacking and the mechanism is not fully understood.3 It was shown that discrimination and depressive symptoms positively correlated with each other and that depressive symptoms could lead to sleep disturbances.245455 However, the association between discrimination and poor sleep is also independent of depression.29 Mental distress such as depression, anxiety, and anger may have a negative effect on sleep in the same manner that worry keeps one up at night.565758 The stress of discrimination may cause physiological arousal that reduces sleep quality.596061 There have been attempts to explain its association with the hypothalamus-pituitary-adrenal gland axis and sympathetic nervous system hyperactivity.61 Under stressful situations, cortisol levels rise, resulting in an increase in norepinephrine and a sense of arousal.61
Although there is little research on the direct relationship between sleep health and discrimination experience, a few cross-sectional studies in Korea have focused on the relationship between sleep health and sociopsychological conditions similar to workplace discrimination. One study investigated the association between job stressors and sleep disorders by analyzing the 3rd KWCS, and it showed that discrimination experience was associated with sleep disorders.62 Our study differs in several ways. First, the previous study analyzed 5 types of discrimination as a single variable, whereas our study analyzed eleven types of discrimination as separate variables. Thus, it is possible to examine the association between each type of discrimination and insomnia symptoms. Second, this study examined the presence of sleep disorders using a simple questionnaire, whereas our study determined insomnia using the validated MISS questionnaire. Third, socioeconomic and occupational factors were more detail adjusted in this study’s models.
Another study investigated the association between work-related sleep problems and organizational factors, and it showed an association between sex discrimination, age discrimination, and other psychosocial working environments and sleep problems.45 A third group studied the association between job-related stress and insomnia, and examined that insomnia was more prevalent among those with relatively elevated job-related distress.44 The fourth investigated whether experiencing workplace injustice, including discrimination, harassment, and violence, was associated with physical and mental health problems (i.e., anxiety/depression and/or sleeping problems) and absenteeism.63 The fifth study was conducted on the discrimination experienced by transgender people which observed that individuals who experienced transgender discrimination had more sleep problems than those who did not.48 The sixth study examined the influence that discrimination experienced by lesbian, gay, and bisexual Korean adults had on sleep health effects and it revealed a correlation between sexual orientation and sleep problems.49
This study has several strengths. First, it analyzed a large sample that represents the Korean workforce. Second, this study examined insomnia symptoms using the validated MISS questionnaire. Third, this study examined the association between 11 different kinds of discrimination and insomnia symptoms, and it was difficult to find previously conducted studies worldwide that evaluated the association between so many different kinds of discrimination and insomnia across many groups. Fourth, statistically significant associations between discrimination experienced on the basis of religion, sex, age, hometown, employment status, and educational level, which has been less investigated globally, and insomnia has been investigated.
There are several limitations to this study. First, since the present study is a cross-sectional study, we were unable to determine the temporal relationship between discrimination experiences and insomnia symptoms. To investigate the temporal relationship in the future, more prospective studies are required. Second, the reported insomnia symptoms in this study were not objective as a self-reported questionnaire was employed. For the objective measurement of sleep health, equipment such as polysomnography or actigraphy should be utilized in future studies. Third, because few immigrant workers were included in the survey, the results may have found little association between insomnia symptoms and experiencing discrimination based on race and nationality, despite the fact that previous studies have found such a relationship.
CONCLUSIONS
This study observed that discrimination experiences due to religion, sex, age, hometown, employment status, and educational level in the workplace were associated with insomnia symptoms and the prevalence of insomnia increases as the number of discriminations experienced increases. Therefore, preventing workplace discrimination may improve workers’ sleep health.
Acknowledgements
This research is supported by the National Research Foundation of Korea (NRF-2021R1C1C1007796).
The authors appreciate the Occupational Safety and Health Research Institute and the Korea Occupational Safety and Health Agency for providing us with the raw data from the 6th Korea Working Conditions Survey.
Notes
Funding: This research is supported by the National Research Foundation of Korea (NRF-2021R1C1C1007796).
Competing interests: The authors declare that they have no competing interests.
Authors contributions:
Conceptualization: Ju S, Cho SS.
Formal analysis: Ju S, Cho SS, Ryu H.
Funding acquisition: Cho SS.
Methodology: Ju S, Cho SS, Ryu H.
Writing - original draft: Ju S.
Writing - review & editing: Cho SS, Kim JI, Ryu H, Kim H.
Abbreviations
CI
confidential interval
KWCS
Korea Working Conditions Survey
MISS
Minimal Insomnia Symptom Scale
OR
odds ratio