Relationship between chronotype and depressive symptoms among newly hired hospital nurses in the Republic of Korea
Article information

Abstract
Background
This study was conducted to examine the relationship between chronotype and depressive symptoms to provide grounded knowledge in establishing nurses’ health promotion strategies.
Methods
The subjects of this study were 493 newly hired nurses working in 2 general hospitals within the university from September 2018 to September 2020. Sociodemographic and work-related characteristics were collected from a medical examination database and a self-reported questionnaire. These included sex, age, marital status, living situation, education level, alcohol consumption, physical activity, prior work experience before 3 months, workplace, and departments. To analyze the associations between the chronotype and depressive symptoms, multiple logistic regression analyses were performed to calculate odds ratios (ORs).
Results
Among participants, 9.1% had depressive symptoms and 16.4% had insomnia. The subjects are divided into morningness (30.2%), intermediate (48.7%), and eveningness (21.1%). The multiple logistic regression analysis controlling for age, living status, education level, alcohol consumption, physical activity, workplace, prior work experience before 3 months, and insomnia, revealed that the OR of depressive symptoms in the eveningness group was 3.71 (95% confidence interval [CI]: 1.50–9.18) compared to the morningness group, and the R2 value was 0.151. It also can be confirmed that insomnia symptoms have a statistically significant effect on depressive symptoms (OR: 2.16, 95% CI: 1.03–4.52).
Conclusions
Our findings suggest that evening-type nurses are more likely to have depression than morning-type nurses. We should consider interventions in a high-risk group such as the evening type nurses to reduce depressive symptoms in nurses.
BACKGROUND
Depression among nurses is one of the important health problems. Depression can affect nurses’ professional performances and leads to nursing errors and negligence.12 It is important to manage a nurse’s mental health not only for the nurse’s health but also for the patient’s health. Nurses are exposed to occupational risk factors for depression, such as long working hours, shift work, emotional labor, and high-intensity work stress.34
In addition to these occupational risk factors, non-occupational risk factors are also important for nurses’ depression. These non-occupational risk factors for depression include sex, age, marital status, housing type, alcohol consumption, physical activity, and chronotype.5678
Among them, chronotype has been known as a risk factor for depression that has recently been attracting attention. Many studies on depression among nurses have been mainly related to shift work, which is the main occupational characteristic of nurses.910 The effect of shift work on mental health is interpreted as being caused by the misalignment between the individual’s circadian rhythm and the socially required circadian rhythm. Therefore, research on individual circadian rhythms is also needed. One of the methods to evaluate an individual’s circadian rhythm is the chronotype.
Chronotype is an intrinsic characteristic classified according to circadian rhythmic expression. The circadian rhythmic expression is a variety of physiological phenomena that appear in a cycle of 24 hours. Physiological parameters such as body temperature, hormone levels, and metabolism change with circadian rhythm.11 A person’s wake, bedtime, and activity time are also related to circadian rhythm. The circadian rhythm is expressed as a complex phenotype under the influence of the interaction of genetic and environmental factors associated with chronotype. Some people prefer to be active early in the day and others prefer to be active late in the day. These traits are termed morningness and eveningness, respectively. Based on morningness-eveningness, the actual activity tendency, including the response to the external schedule, is expressed in the concept of a chronotype. The chronotype can be divided into 3 types: morning type, evening type, and intermediate type. The morning type goes to bed early and wakes up early to be active early in the day, whereas the evening type sleeps relatively late and wakes up late and is active later in the day.12 Methods for measuring an individual’s chronotype are largely divided into those using a physiological test and a self-report questionnaire. It has been reported that the chronotype affects mood and that eveningness is particularly associated with depression. An increase in the diagnosis of major depressive disorder in the eveningness was reported in a case-control study conducted in the Netherlands using a cohort of patients with depression.13 A large population-based study conducted in Finland also reported an increase in depression-related indicators such as depression symptoms and antidepressant use in the eveningness.14
There are not many previous studies on chronotype and depression among nurses. A cross-sectional study of Japanese nurses reported that a greater evening type score was independently associated with a higher degree of depressive symptoms.15 Meanwhile, in a prospective study using the Nurses’ Health Study II cohort in the United States, the risk of depression was lower in those who reported themselves as early chronotypes. However, the risk of the evening type was not clear.16 It seems that studies have not accumulated enough to produce clear results. This study was conducted to examine the relationship between chronotype and depressive symptoms to provide grounded knowledge in establishing nurses’ health promotion strategies.
METHODS
Study population
The subjects of this study were newly hired nurses working in two general hospitals within the university from September 2018 to September 2020. The subjects were nurses who received pre-placement health checkups for the night shift at the department of occupational medicine of a university hospital. This health checkup is for nurses who have not started the night shift, but are performing duties including the day or evening shift before being assigned to the night shift. 509 newly employed at two university hospitals were included as study subjects. We excluded participants who did not respond to the questionnaire on insomnia (n = 1), depressive symptoms (n = 1), and chronotype (n = 14). The final number of study subjects was 493.
Measurements
Sociodemographic and work-related characteristics were collected from a medical examination database and a self-reported questionnaire. These included sex, age, marital status, living situation, education level, alcohol consumption, physical activity, prior work experience before 3 months, workplace, and departments.
Assessment of chronotypes
The chronotype was evaluated using the Korean translation of the Composite Scale (KtCS).1718 It consists of a total of 13 items, of which 3 items are scored on a scale of 1–5 points, and 10 items are scored on a 1–4 points scale, indicating the distribution of points ranging from 13 to 55 points. A lower score indicates an eveningness, and a higher score indicates a morningness of chronotype. In this study, based on the 25th percentile, 26 points or less were classified as eveningness, and those with 34 or more points were classified as morningness.
Assessment of depressive symptoms
Depressive symptoms were assessed using a Korean version of the Center for Epidemiological Studies Depression scale (CES-D) with 20 items.19 The total score is calculated by summing the scores of the questions (0–3 points for each). A higher score indicates greater severity of depressive symptoms. The presence of depressive symptoms was defined as the sum of the CES-D scores of 16 or more.
Assessment of covariates
Regarding alcohol consumption, participants were classified as non-drinkers, moderate drinkers, and risky drinkers according to the World Health Organization criteria on the pre-placement health checkup questionnaire. A moderate drinker is someone who consumes small amounts of alcohol at a time (e.g., 20 g or less for women and 40 g or less for men) less than once a week. Conversely, a risky drinker is a person who consumes more than the aforementioned amount. The degree of physical activity was classified as “insufficient,” “sufficient,” and “fully sufficient” according to the Korean Physical Activity Guidelines based on the 2008 Physical Activity Guidelines for Americans. Aerobic activity of fewer than 150 minutes per week was classified as “insufficient,” and moderate-intensity aerobic activity of 300 minutes or more was classified as “fully sufficient” 3–5 times per week. “Sufficient” was an amount between “insufficient” and “fully sufficient.”
Prior work experience before 3 months was defined as those who responded that they had work experience in the past 3 months. The workplace was classified by labeling the 2 hospitals belonging to the study participants as hospital A and hospital B, respectively. Departments were classified into physician assistant (PA), special, and general according to the department registered in the pre-placement health checkup. Physician assistants are nurses who partially perform the duties of a doctor under the guidance and supervision of a doctor, such as surgical assistants, ward patient management, and outpatient consultation. Special includes workers in the operating room, anesthesia recovery room, intensive care unit, nervous system intensive care unit, neonatal intensive care unit, and cardiovascular intensive care unit. Those who worked in a general ward that did not fall under special were classified as general.
Insomnia was assessed using the Korean version of the Insomnia Severity Index (ISI).20 It consists of a total of 7 items, of which are scored on a 0–4 points scale, indicating the distribution of points ranging from 0 to 28 points. If the total score exceeds 8 points, it is classified as a risk group for insomnia.
Statistical analysis
All statistical analysis was performed using SPSS IBM software (version 22; IBM Corp., Armonk, NY, USA). The results of descriptive analyses were reported as proportions. The associations of individual characteristics assessed by categorical variables with the chronotype and depressive symptoms were evaluated by chi-square tests except for those of sex and marital status with depressive symptoms. Those were evaluated by Fisher’s exact test. Since the age was not normally distributed, the Kruskal-Wallis tests were performed to test the differences in the distribution of the age. To analyze the associations between the chronotype and depressive symptoms, multiple logistic regression analyses were performed to calculate odds ratios (ORs).
Model 1 presents crude ORs calculated without covariates. Model 2 is adjusted for sociodemographics and lifestyle risk factors. Model 3 was adjusted for work-related data in addition to the covariates of model 2. Model 4 was adjusted for insomnia symptoms in addition to the covariates of model 3. In addition, the analysis was stratified according to the workplace. The ORs were calculated by adjusting the variables excluding the workplace, which was the stratification standard.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Ewha Womans University Mokdong Hospital (EUMC 2018-05-017) and was conducted in full accordance with the Declaration of Helsinki developed by the World Medical Association. Written informed consent was obtained from all subjects when they were enrolled.
RESULTS
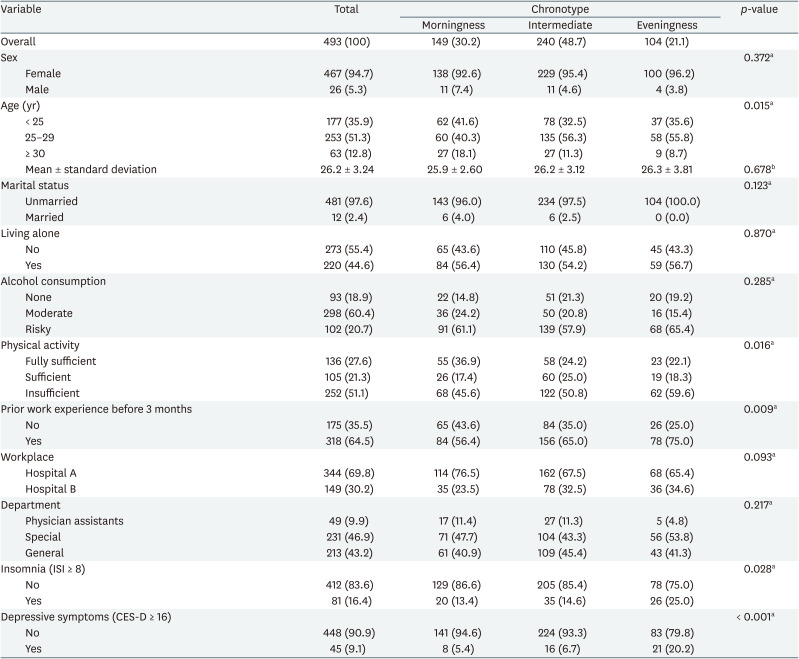
Characteristics of the study population according to the chronotype were presented in Table 1. A total of 493 participants who completed the survey were included in the study. Most of the participants were female (94.7%), under the age of 30 (87.2%), and unmarried (97.6%). The number of nurses living alone was 273 (55.4%). According to alcohol consumption, 93 (18.9%) non-drinkers, 298 (60.4%) moderate drinkers, and 102 (20.7%) risky drinkers were identified. There were 136 (27.6%) people with fully sufficient physical activity, 105 (21.3%) with sufficient physical activity, and 252 people (51.1%) with insufficient physical activity. There were 318 (64.5%) participants with work experience within the past 3 months. The number of participants working at Hospital A was 344 (69.8%), which was higher than that of 149 (30.2%) working at Hospital B. There were 231 nurses (46.9%) classified as special departments and 213 (43.2%) nurses classified as general departments. The number of physician assistants was 49 (9.9%). Among them, 81 (16.4%) participants had insomnia and 45 (9.1%) participants had depressive symptoms. According to KtCS, the subjects are divided into 149 morningness (30.2%), 240 intermediate (48.7%), and 104 eveningness (21.1%). In the 3 groups according to the chronotype, the proportion of individual characteristics was not statistically significantly different except for age, physical activity, prior work experience before 3 months, and insomnia. The proportions of nurses with high physical activity (p = 0.016), with no work experience before 3 months (p = 0.009), and without insomnia (p = 0.028) were higher in the evening group than in the other 2 groups. The proportion of the under 25 years old and over 30 years old nurses was higher in the eveningness group than in the morningness and intermediate groups (p = 0.015). Meanwhile, there was no statistically significant difference in the mean age of each group.
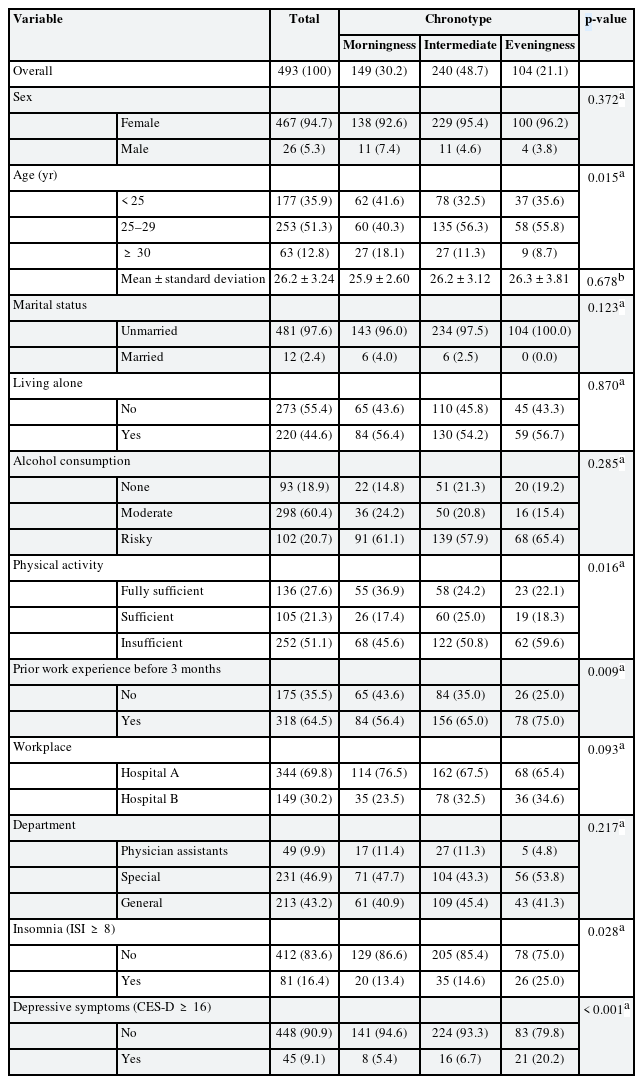
Baseline characteristics of newly hired nurses according to the chronotype
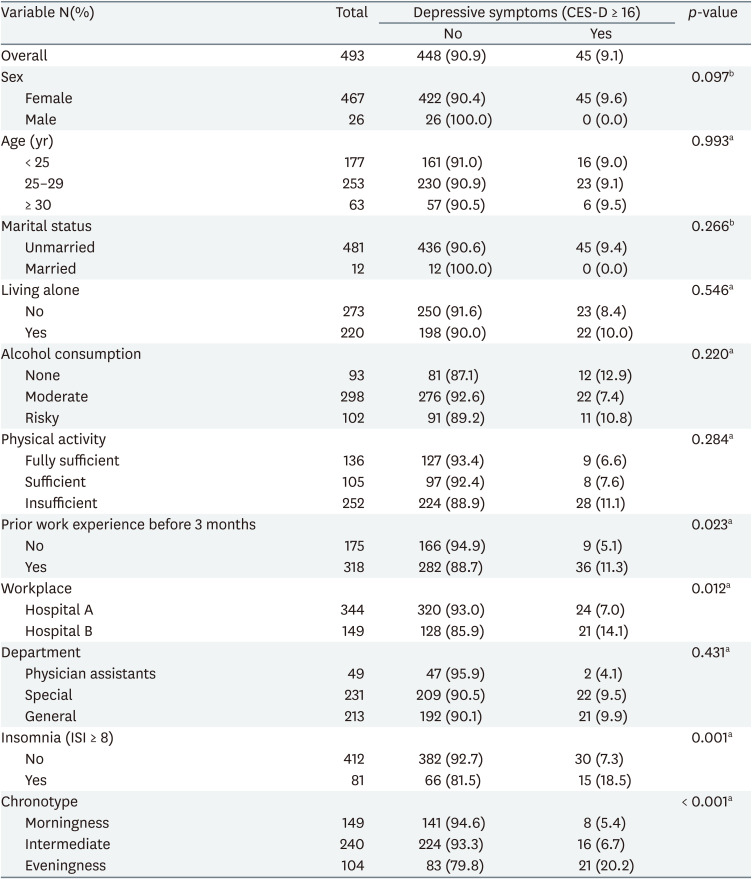
Table 2 shows the differences by groups in the prevalence of depressive symptoms assessed by the CES-D questionnaire. The prevalence of depressive symptoms was statistically significantly higher in the group of eveningness than in the group of morningness (p < 0.001). Also, the group with insomnia symptoms and with working experience before 3 months showed statistically significantly more depressive symptoms compared to those without (p = 0.001 and p = 0.023, respectively). The rates of depressive symptoms were statistically significantly different between the study subjects of the two hospitals included in the study (p = 0.012). There was no statistically significant difference in the prevalence of depressive symptoms according to sex, age, marital status, living alone, education level, alcohol consumption, physical activity, and departments.
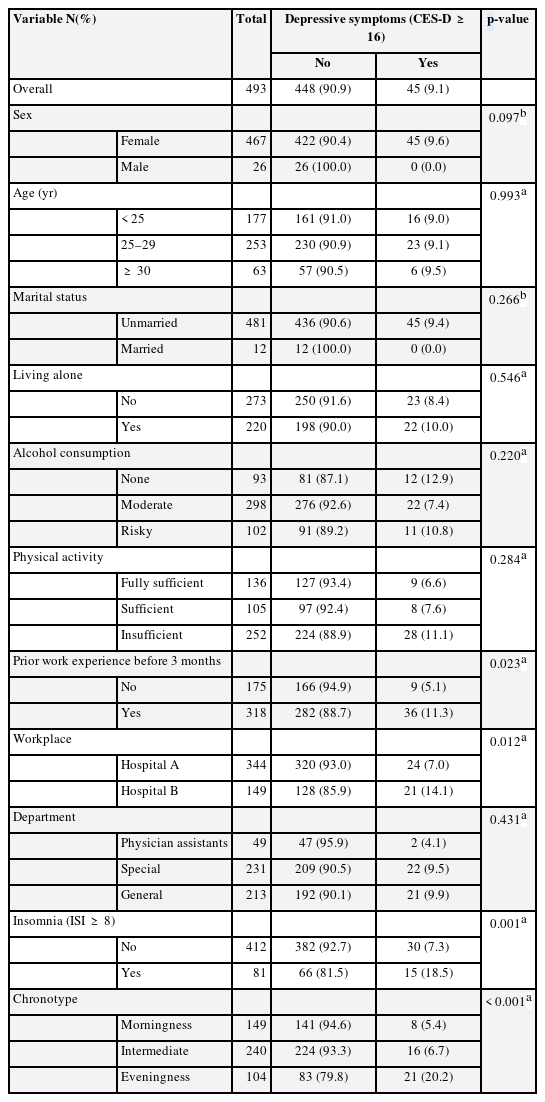
The prevalence of depressive symptoms according to the characteristics among newly hired nurses
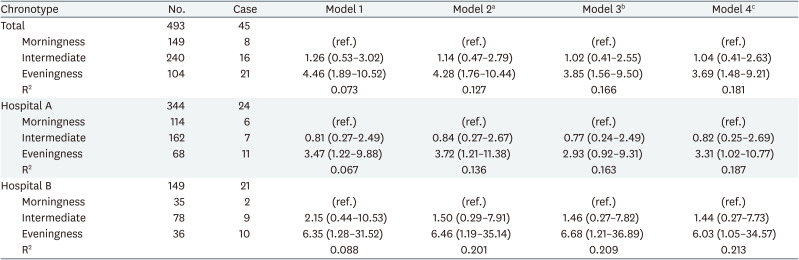
Table 3 presents four statistical models with different covariates to evaluate ORs for depressive symptoms according to chronotypes among nurses as a whole and by workplace. Compared to the group of morningness, in the group of eveningness, the OR for depression was statistically significantly higher in all models among nurses as both a whole and by the workplace.
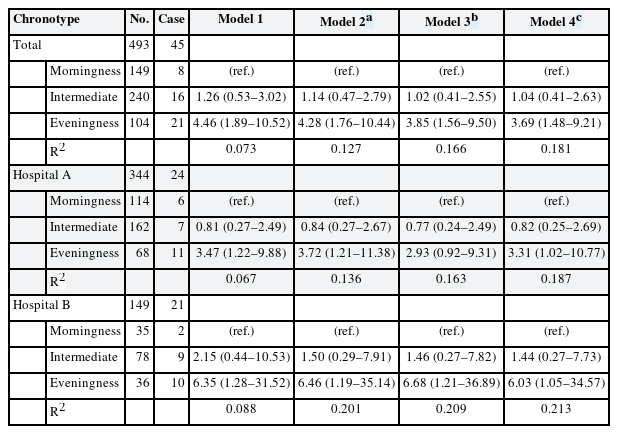
Odds ratios of chronotype for depressive symptoms among newly hired nurses
In model 1, which is a crude model, the OR of the chronotype among overall nurses was 4.46 (95% confidence interval [CI]: 1.89–10.52) and the R2 value was 0.073. It is shown in models 2, 3, and 4 that the OR decreased and the R2 value increased whenever the confounding variable was added. In model 4, the final model, the OR of depressive symptoms in the eveningness group among overall nurses was 3.71 (95% CI: 1.50–9.18) compared to the morning group, and the R2 value was 0.151. In model 4, it also can be confirmed that insomnia symptoms have a statistically significant effect on depressive symptoms (OR: 2.16, 95% CI: 1.03–4.52). In nurses of Hospital A and Hospital B, it is also shown that the OR decreased and the R-squared value increased. In model 4, the OR of depressive symptoms in the eveningness group among nurses of Hospital A was 3.31 (95% CI: 1.02–10.77) and that of Hospital B was 6.03 (95% CI: 1.05–34.57)
DISCUSSION
The most significant finding of our study was that the nurses with evening type had a higher risk of depressive symptoms than those with morning type, even after adjusting for confounding variables such as demographics, lifestyle, work characteristics, and insomnia. The explanatory power of the model in our study is not high. If more risk factors were included as study variables, it could be increased. The increased risk of depressive symptoms in the group with the evening type shows consistent results in the studies conducted with students2122232425 or shift workers.26 In a cross-sectional study conducted on nurses in Japan, the score of depressive symptoms had a statistically significant positive correlation with the score of eveningness.15 However, in the Nurses’ Health Study II, a large cohort study in the United States, the risk of depression was 1.13 times higher in the evening type group than in the intermediate group, but it did not show a statistically significant increase.16 This study differs from our study in that the health outcome was physician-diagnosed depression. Our study provides additional evidence for the possibility that evening-type individuals may increase the risk of depressive symptoms.
Several articles reported on the mechanism of association between eveningness and depression. Since morning-based circadian rhythms are often socially required, evening types are more likely to experience circadian misalignment than other types. Many regulatory hormones are associated with circadian rhythms. Some hormones, such as growth hormone and prolactin, are regulated by sleep, others such as cortisol and melatonin are affected by the circadian cycle, and others such as insulin are affected by eating and fasting.27 The association between these hormones and depression has been suggested by several studies. Depression is considered more common in the general population in the presence of adult-onset isolated growth hormone deficiency, which is improved by growth hormone supplementation.28 The rise in morning cortisol levels is reported to be associated with depression in adolescents and young adults.29 Melatonin is known to induce antidepressant effects.30 In addition, the interaction effect between melatonin and serotonin signals significantly affects depression.30 Insulin has been suggested to have a potential role in the onset of depression.31 Circadian misalignment can result in dysregulation of these hormones, which affects downstream physiological processes and health outcomes.3233 This misalignment often referred to as “social jet lag,” has been suggested as a link between eveningness and depression as well as other general health risks.1434
Although it was not statistically significant, the prevalence of depression tended to be lower in male nurses than in female nurses. None of the male nurses in the study had depressive symptoms. It is known that the prevalence of depression in women is twice that of men.35 This trend may have been reflected in this study as well. However, the number of men included in the study was 26, which is too small to judge, so more research is needed.
Most of the previous studies exploring the relationship between chronotype and depression did not use sleep-related variables as confounding variables. Depressive symptoms are closely related to sleep problems. These 2 symptoms may be coexisting problems, or one may act as the cause of the other.36 That is why it is necessary to deal with sleep problems delicately when exploring the causes of depression. Rarely, there have been studies that suggested the results of adjusting for sleep time15 and sleep quality.37 As far as we know, no studies evaluated using the ISI. In our study, sleep problems were evaluated using the ISI. As a multivariate analysis model to suggest the association between chronotype and insomnia, both models with and without the ISI were presented. If it can be assumed that insomnia symptoms are not related to chronotype or depressive symptoms, the risk of chronotype to depressive symptoms can be estimated from the effect presented in model 4. In this study and previous studies,1537 the evening type has an increased probability of developing depression regardless of sleep quality, sufficiency, or sleep disturbance.
Meanwhile, the OR was slightly decreased in model 4, which was adjusted for the sleep problem, compared to model 3, which was adjusted for the sleep problem. It is necessary to interpret this result considering that it may be an over-adjustment. A study confirming the mediating effect of sleep quality on the increase in evening-type depressive symptoms showed that sleep quality partially mediated the increase in depressive symptoms.37 Therefore, the evidence to date suggests that the depressive symptoms observed in the evening type are not solely due to sleep disturbance.
The results of this study should be interpreted in consideration of the following suggestions. First, it is difficult to identify a causal relationship as it is a cross-sectional study. This study is based on the basic data of the follow-up study, and additional follow-up is required. It is highly likely a temporal of precedence relationship between chronotype and depression. It is known that chronotype is mainly determined by an individual’s unchanging attributes such as genes,38 age,39 sex,40 and season of birth.41 Although chronotype may change with everyday light exposure,42 our study was conducted before the night shift assignment. In other words, we think that the chronotype is more likely to precede depressive symptoms. In a longitudinal study, it was confirmed with a group of students.43 Second, chronotype, depressive symptoms, and some other covariates such as insomnia were evaluated using self-reported questionnaires. Concerning the validity of these measurement tools, structured questionnaires were used, and it can be said that structural validity is guaranteed. Furthermore, the reliability of these tools in the Korean population has been verified.17181920 Meanwhile, there is a possibility that depressive symptoms and insomnia symptoms may be underreported because these were evaluated during the pre-placement medical examination. However, since this is a non-differential error, it is thought that it had little effect on the evaluation of the association between chronotype and depressive symptoms.
There are strengths in our study as follows. First, although there were several studies that analyzed the depressive symptoms of nurses in the past, this study was reported in a situation where there were not many studies on chronotype and depressive symptoms in the nurse group. We recruited a relatively large-scale study target for a single occupational group of newly hired nurses. Second, we used a structured questionnaire and multiple statistical models to enhance explanatory power through more sophisticated analysis. In the Nurses’ Health Study II, the chronotype was evaluated with one question what kind of chronotype you consider yourself to be.16 Since the chronotype, insomnia, and depressive symptoms were evaluated through a structured questionnaire in this study, the reliability of the result could be increased compared to the previous study. In addition, in statistical analysis, we used several statistical models including various confounding variables such as demographic, lifestyle, work-related characteristics, and insomnia symptoms. Through this, we think that we can have a rich understanding of the factors related to depressive symptoms in nurses. Based on the results of this study, it will be possible to contribute to improving the mental health of nurses by intervening in nurses who are at high risk for depression.
CONCLUSIONS
Our findings suggest that evening-type nurses are more likely to have depression than morning-type nurses. We should consider interventions in a high-risk group such as the evening type nurses to reduce depressive symptoms in nurses.
Notes
Funding: This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (grant number: 2018R1A2B6004110).
Competing interests: The authors declare that they have no competing interests.
Author Contributions:
Conceptualization: Lee SM, Kim HJ.
Data curation: Lee SM, Ryu J.
Formal analysis: Lee SM, Jung HN, Kim HJ.
Funding acquisition: Kim HJ.
Investigation: Lee SM, Kim HJ.
Writing - original draft: Lee SM, Kim HJ.
Writing - review & editing: Lee SM, Jung HN, Ryu J, Jung WC, Kim YM, Kim HJ.