Technetium-99m hand perfusion scintigraphy (Raynaud’s scan) as a method of verification in hand arm vibration syndrome: a review
Article information

Abstract
It is important to assess the blood flow of fingers in the verification of hand-arm vibration syndrome. In the Republic of Korea, most assessments of the blood flow in the fingers are performed using a cold provocation test with finger skin color change. However, this test is a non-objective method with a relatively low sensitivity, leading to possible social and legal problems. Thus, we reviewed the characteristics of several tests that assess the blood flow in the fingers. Among these tests, using the radioactive isotope method, Raynaud’s scan has a relatively higher sensitivity and specificity than other tests, provides objective results, and is approachable in many hospitals. So we suggest using Raynaud's scan as an alternative test when cold provocation test with finger skin color change is negative in vibration exposed worker.
BACKGROUND
Raynaud’s phenomenon is a symptom of color change in the finger skin due to decreased digital blood flow. Primary Raynaud’s phenomenon refers to the absence of an underlying pathological cause, whereas secondary Raynaud’s phenomenon includes pathological causes such as rheumatoid, hematological, autoimmune, and vascular diseases. The known causes of Raynaud’s phenomenon include large vessel, occupational, autoimmune rheumatic, drug/chemical-related, and vaso-occlusive diseases.1 The prevalence of Raynaud’s phenomenon was shown to be 3.8%,2 9.6% (for women), 5.8% (for men),3 and 3.5% (4.3% [for women], 2.7% [for men])4 in the United States, respectively.
Occupational vibration exposure affects the skin, blood vessels, and nerves of the extremities, leading to symptoms known as hand-arm vibration syndrome (HAVS). Vascular symptoms mainly appear as cold-induced spasms of fingers vessels and are called vibration white fingers (VWFs).5 VWF has a prevalence of 53% among workers who use pneumatic chipping and grinding tools in foundries and shipyards in the United States,6 21.7% among forestry workers who use brush saws and chain saws and stone workers who use rotary and percussive tools for marble processing (the median duration of daily exposure was 126 minutes),7 and 15.4% among grinding workers who use belt grinding machines in sports equipment factory in China (the mean exposure duration was 6.9 ± 1.4 hours).8 The Republic of Korea (ROK) conducts medical examination for workers exposed to vibration. According to a report by the Ministry of Employment and Labor in 2021, 10,925 workplaces had vibration work and 167,062 people were exposed to vibration work. Among them, 276 patients had possible occupational diseases and 10 patients had probable occupational diseases.9 The prevalence in ROK was lower than the prevalence studies among other countries. This is thought to be partially because, while the ROK’s medical examination for workers exposed to vibration evaluates peripheral circulation, nerve function, and motor function without cold provocation in the first examination, other papers evaluated by cold provocation test or past VWF history. In addition, there are differences in the study subjects such as exposure level.
Methods for assessing decreased finger blood flow include cold and vibration provocation tests with finger color change, finger skin temperature, finger systolic pressure, finger arterial inflow, and finger blood flow using Doppler or radioactive isotopes.10 There is no reproducible “gold standard” diagnostic test for Raynaud’s phenomenon (RP) yet,11 so most of articles set their own gold standard for anamnestic diagnosis based on the patient’s RP history. But anamnestic diagnosis is not a true method of reference under all circumstance. Anamnestically non-symptomatic RP in vibration-exposed worker with or without a positive history of RP can be exist. This implies that the specificity of objective test is probably higher than estimated with the interview as a reference.12
Guidelines on Raynaud’s syndrome have been prepared in the ROK13; however, current standardized diagnosis criteria are still lacking. In ROK, in order to receive compensation for Raynaud’s syndrome according to the guidelines on Raynaud’s syndrome of Industrial Accident Compensation Insurance Act, it is necessary to take a photo of Raynaud’s phenomenon. Other tests such as Raynaud’s scan, skin temperature test, finger blood pressure test, and nail pressure test should also be performed if necessary.13 Among those who have actual symptoms and want compensation for Raynaud’s syndrome, the symptoms were not reproduced in the cold provocation test, so the diagnosis of Raynaud’s syndrome was not confirmed. In this case, there was a limitation in determining whether to compensate only by taking pictures. Since only the cold provocation test with finger skin color change is fixed as an essential test, most of the work-relatedness assessments in many cases use only the cold provocation test with finger skin color change as a diagnostic indicator. Among the work-relatedness assessments (23 cases) related to Raynaud’s syndrome conducted by the Korea Labor and Welfare Service from January to June 2016, 19 patients underwent the cold provocation test with finger skin color change only, and three patients underwent the cold provocation test with finger skin color change and Raynaud’s scan test.14 A cold provocation test with finger skin color change and nail compression test were performed in one patient. The approval rate conducted by the Korea Labor and Welfare Service that performed only the cold provocation test with finger skin color change was 34.8%, and the approval rate was 66.7% when the cold provocation test with finger skin color change and Raynaud’s scan were combined.14
We reviewed precedents related to HAVS. In some cases, the cold provocation test with finger skin color change was performed only in the work-relatedness assessment, which resulted in no finger skin color change. Therefore, they were not approved of work relatedness and applied for the trial. Subsequently, the decrease in blood flow in the finger was confirmed using Raynaud’s scan during the trial. Raynaud’s scan helped diagnosis of Raynaud’s phenomenon by discriminate false-negative result from the cold provocation test with finger skin color change. The court reversed the previous decision resulted from no finger skin color change in the cold provocation test with finger skin color change.1516 Other judgment decided that the cold provocation test with finger skin color change had limitations in reproducibility and sensitivity, and that Raynaud’s Scan was the most helpful in verifying Raynaud’s phenomenon.17
METHODS
This study aimed to review the characteristics of the cold provocation test with finger skin color change and other tests related to HAVS. And we aimed for findings a recommendation for an objective test that presents consistently high sensitivity as a diagnostic tool, satisfying the social requirements for compensation for HAVS.
We reviewed studies related to Raynaud’s phenomenon, HAVS, and VWFs. Our main focus was the methods used to diagnose Raynaud’s phenomenon. The characteristics, sensitivity and specificity of each diagnostic method were evaluated and compared. Searches were conducted using the EMBASE and Medline data bases.
The following were the search terms used: “hand arm vibration syndrome” OR “vibration white finger” OR “Raynaud’s phenomenon” And “cold provocation test” OR “hand chilling test” And “sensitivity” OR “specificity.” All articles published up to 20 February 2022 were searched. We included studies that satisfied the following criteria: 1) articles on the diagnosis of Raynaud’s phenomenon and 2) articles presenting sensitivity and specificity. All relevant published articles were included regardless of published date. Even if the entire original text cannot be reviewed, studies suggesting the research method, sensitivity, and specificity in the abstract or other review articles have also been added. If the study was about Raynaud’s scan, only the test method was extracted, regardless if the sensitivity or specificity was not presented.
REVIEWS
Cold provocation test with finger skin color change
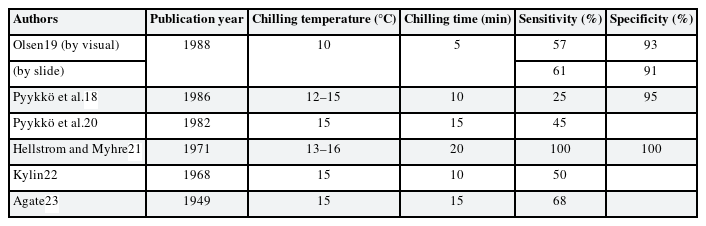
A cold provocation test with finger skin color change assessed for color change in fingers after immersing both hands in cold water. The cold provocation varied with the temperature of the cold water being 10°C–16°C, with a cold provocation time of 5–20 minutes. After cold provocation, a finger color change was observed for at least 10 minutes.13
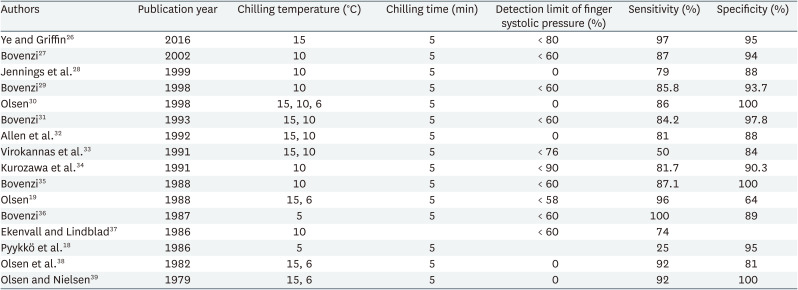
Sensitivity (25%–100%) and specificity (93%–100%) varied from study to study (Table 1), but the sensitivity was relatively low whereas the specificity was relatively high. In one study, the kappa coefficient was 0.38 in tests performed on the same day with a time difference of at least 2 hours in the same subjects.12 When the test was repeated with a time difference of more than 2 hours, there were cases where subject who showed a positive result in one test and subsequently showed negative result a follow-up test.18 Because the color change of the finger is judged by the subjective eyes of each doctor, subjective judgment occurs when the color change is unclear. In addition, one study suggested that this test has low sensitivity; thus, even if a negative result is obtained, diagnosis cannot be ruled out.12 In some studies, body chilling or metal cylinder squeezing was accompanied during cold provocation. Another study used a smartphone-monitoring application. This monitoring application prompted subjects to take pictures of their hands during Raynaud’s phenomenon, and the researchers then subsequently analyzed the pictures.24 Poole et al.25 recommended that use photographs during the attack of blanching for the classification of HAVS. If the most severe attack is not captured, scoring is pending. They also opposed to routine angiography.
Characteristics of cold provocation test with finger skin color change
Cold provocation test with finger systolic pressure
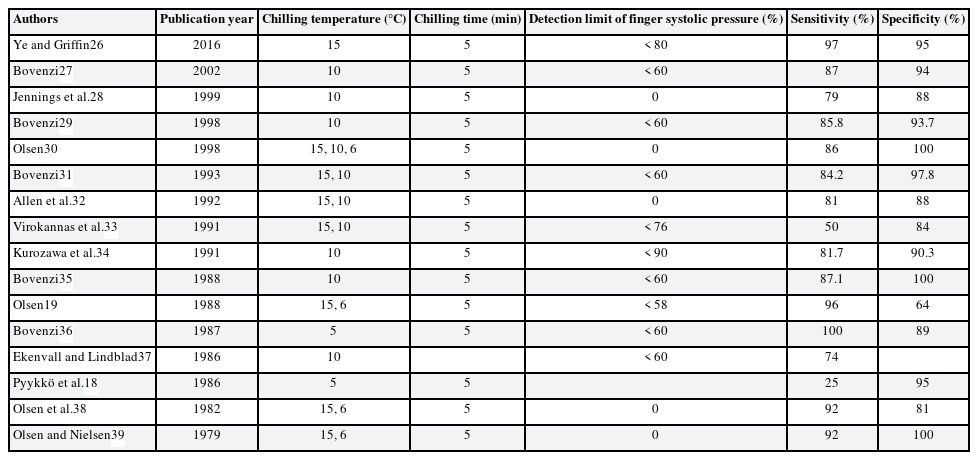
A cold provocation test with finger systolic blood pressure can be performed one finger at a time; therefore, the operator must select the target finger to be tested. The target finger was equipped with a tourniquet cuff to blocking blood flow during cold provocation in the proximal phalanx, a cuff for cooling and blood pressure measurement in the middle phalanx, and a photoplethysmography device for checking blood flow in the distal phalanx. The target finger is cooled locally by circulating cold water in the cuff of the middle phalanx, while the tourniquet cuff of the proximal phalanx blocks blood flow to the target finger. After cooling, the tourniquet cuff was released, the pressure of the blood pressure cuff was gradually lowered, and the blood pressure at the moment when blood flow was confirmed on the photoplethysmography device of the distal phalanx was recorded. The ratio (finger systolic pressure% [FSP%]) of the systolic blood pressure (with cooling) of the target finger and the systolic blood pressure (without cooling) of the other finger is calculated.26
The lower normal limit of FSP% varied from 0% to 89%. In several studies, body chilling was accompanied during cold provocation. The sensitivity was 70%–100% and the specificity was 58%–100% (Table 2). In one study, the participants performed a psychological challenge during the cooling, but there was no statistically significant difference.28
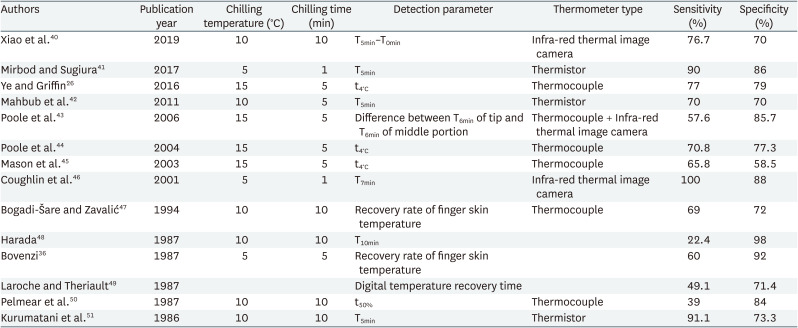
Characteristics of cold provocation test with finger systolic pressure
Cold provocation test with finger skin temperature
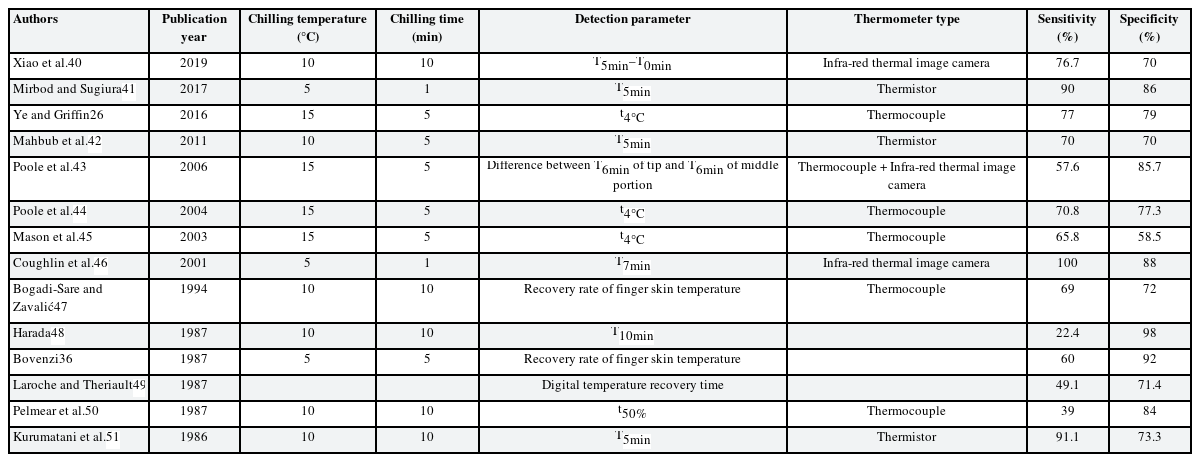
Finger skin temperature can be measured in two ways. One is to attach a temperature sensor (thermocouple or thermistor) to the target point, and the other is to use an infrared camera for thermal imaging.
The detection parameters used in the test were varied, including the rewarmed skin temperature after cooling, times for fingers to rewarm, and rewarming rate after cooling. The sensitivity was 14%–100%, and the specificity was 37%–100% (Table 3). Another previous study also derived the temperature difference between the center of the palm and the fingers (or the temperature difference between the center of sole and the big toe) as a detection parameter without any cooling required.52
Characteristics of cold provocation test with finger skin temperature
Perfusion scintigraphy using radioactive isotopes (Raynaud’s scan)
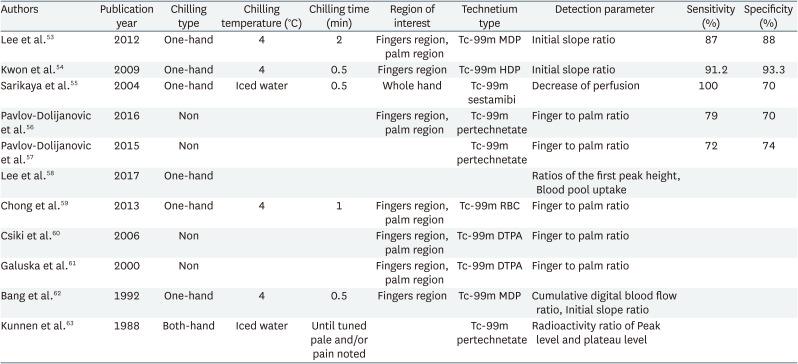
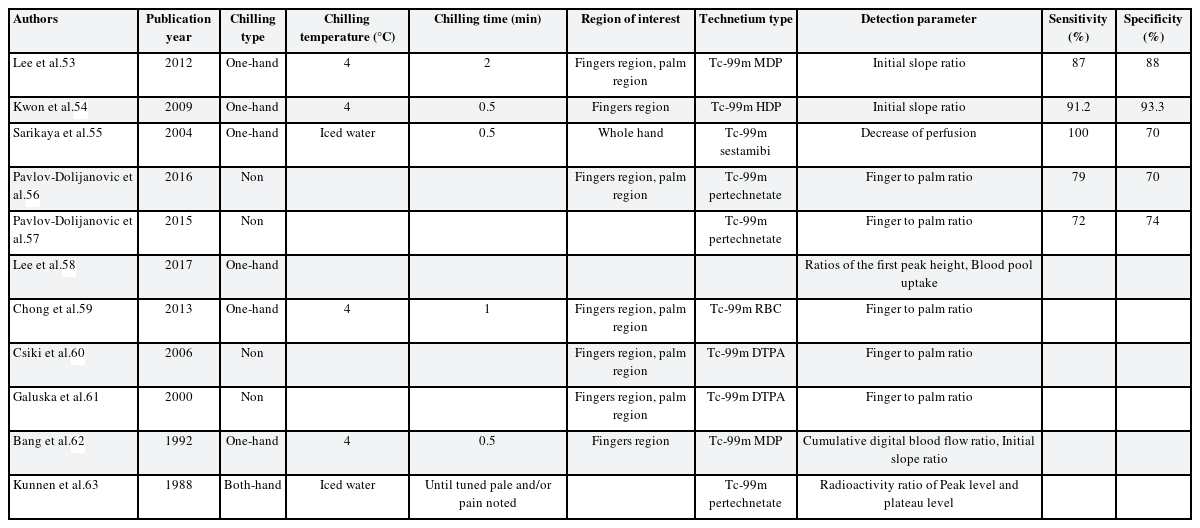
In most perfusion scintigraphy using radioactive isotopes, the one-hand chilling method is often preferred. Among both hands, the more symptomatic hand is cooled for a certain period of time and given a recovery time, before injecting the radioactive isotopes. After the injection, static and dynamic images were acquired using a gamma camera. Subsequently, a region of interest (ROI) is drawn from the obtained image for quantitative calculation.53 The ROI is often manually drawn by dividing the area of the four fingers (excluding the thumb) and the palm. There have been studies with and without cold provocation, and the cold provocation method was also varied. The radioactive isotopes used were technetium-99m bound with various ligands, such as Technetium-99m methylene diphosphonate, Technetium-99m red blood cell, Technetium-99m hydroxymethylene diphosphonate, Technetium-99m pertechnetate. For the detection parameters, the finger-to-palm ratio calculated from the blood flow of the two ROIs, initial slope in the time-count graph, and first peak height of the count were used (Table 4).
Characteristics of Raynaud’s scan
In one study, perfusion scintigraphy was performed by dividing the participants into the one-hand chilling group and the non-chilling group, and this study showed that the one-hand chilling method had higher sensitivity and specificity.53 In only one study, a both-hand chilling method was performed.63 In a case report, to test both hands, the left hand was tested first, and after 1 week, the right hand was tested.59 In another study, first peak height and initial slope were lower in HAVS-related occupational Raynaud’s phenomenon than in primary Raynaud’s phenomenon. These findings suggest the possibility of using Raynaud’s scan as a differential test between primary Raynaud’s phenomenon and HAVS-related occupational Raynaud’s phenomenon.58
DISCUSSION
The main cause of HAVS is local vibration, and the main frequency that causes damage is between 25 and 320 Hz. The pathogenesis of HAVS is complex and not fully understood.5 Its vascular symptoms are caused by an imbalance between vasoconstriction and vasodilatation. This imbalance leads to the predominance of vasoconstriction due to arterial smooth muscle hypertrophy, periarterial fibrosis, and damage of endothelial cells and receptors.64 The main pathological findings in HAVS are i) muscular layer of the artery wall thickening with muscle cell hypertrophy, ii) peripheral demyelinating neuropathy with increased numbers of Schwann cells and fibroblasts, and iii) increased amounts of connective tissue that causes perivascular and perineural fibrosis.65 Furthermore, these changes become more severe as the vibration exposure increases.66
The diagnosis of HAVS is difficult because it is possible only after identifying related symptoms, occupational vibration exposure, and other causes of secondary Raynaud’s syndrome. Decreased blood flow in the fingers of patients with vibration exposure, while other causes of secondary Raynaud’s syndrome have not been identified, is key to HAVS verification and compensation. Work-relatedness assessment and compensation are related to social and legal issues beyond medical judgment.67 Thus, in the work-relatedness assessment of HAVS, there is a social demand for objective verification. However, there is no gold-standard test for this purpose currently. Therefore, we compared tests that could assess the decrease in finger blood flow among patients with suspected HAVS.
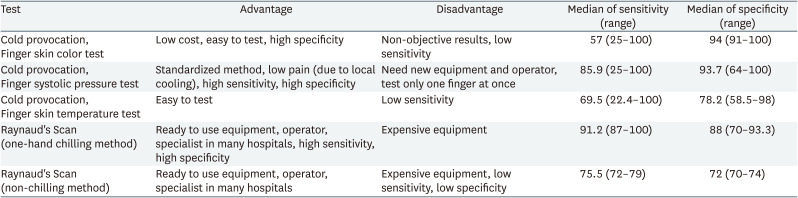
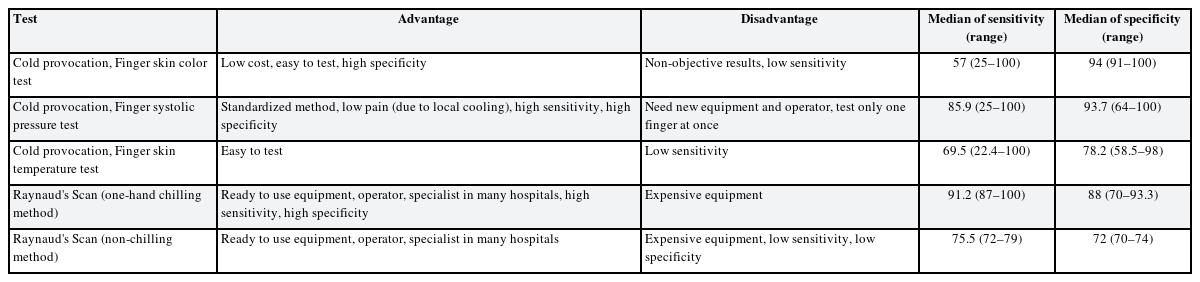
The cold provocation test with finger skin color change has relatively low costs, ease of testing, and high specificity. Therefore, this can be suggested as a first test for HAVS in a clinical setting. Because of its high specificity, it is helpful in diagnosing HAVS if color changes are observed during the test. However, if the finger color change is not checked or remains unclear, an additional objective examination is necessary, considering the low sensitivity and nonobjective characteristics of the cold provocation test with finger skin color change. In addition, the use of imaging diagnostic criteria for case definition in the diagnosis and compensation of occupational musculoskeletal disorders provides higher quality than using only physical examinations.68
The nail pressure test (Lewis-Prusik test) is also used to evaluate HAVS. But this test is poorly standardized and the result unlikely to be helpful unless it is grossly abnormal.69 Also, considering that the tester judges the return to normal color, it’s results considered to be subjective like skin color change test.
The advantage of the cold provocation test with finger systolic blood pressure is that it uses a standardized test method, and the patients experience minimal pain as a result of local cooling.12 It also has relatively high sensitivity and specificity (Table 5). However, many hospitals do not have testing equipment (finger cuff, finger blood pressure gauge, finger photoplethysmograph, and recorder works with blood pressure gauge and photoplethysmograph); therefore, new expensive equipment and operators are required.12 Additionally, only one finger can be tested simultaneously. Thus, to assess the work-relatedness of HAVS, the test needs to be repeated when information about another fingers or other hand is required.
The advantage of the cold provocation test with finger skin temperature is that it can test all fingers simultaneously, and the test method is easy.12 Although it provides objective results, it has a low sensitivity similar to that of the cold provocation test with finger skin color change (Table 5). Therefore, in cases where the skin color test was negative, cold provocation test with finger skin temperature was not suitable as an additional test. Proud et al. concluded that Cold provocation test with measurement of digital rewarming times was no value in evaluating the presence or severity of HAVS.70
Perfusion scintigraphy using radioactive isotopes (Raynaud’s scan) with one-hand chilling had the highest sensitivity and relatively high specificity (Table 5). However, the gamma camera used in this test is expensive. Nonetheless, in many hospitals that provide nuclear medicine tests (diagnostic imaging of the thyroid, salivary gland, urinary bladder, vesicoureteral reflux, and nasolacrimal drainage, Meckel’s diverticulum, bone, cardiac perfusion imaging, cerebral perfusion imaging used to localize the area of stroke), operators and specialists, and gamma camera are already prepared, allowing Raynaud’s scan to be performed easily in simple settings.62 Currently, there are 303 gamma cameras in ROK in 201971 and 331 in 2021.72 Considering that there are 356 general hospitals in ROK (in 2019),73 almost all general hospitals can use gamma cameras.
In secondary Raynaud’s phenomenon with unilateral attack, abnormalities in peripheral vessels, trauma, embolism, or work-related secondary Raynaud’s phenomenon may be suspected.74 Authors found two cases of unilateral Raynaud’s phenomenon caused by vibration injury of digital vessels.75 In one study conducted in the ROK, 69.1% of patients had more severe symptoms in the right hand. Considering the left-handedness rate (5.8%) of the ROK, the study suggested the possibility of an association between the right-handed rate and the severity of symptoms was relatively low. They also suggested the possibility of an association between the severity of symptoms and the method of using vibration tools (vibration exposure history).76 Therefore, in the work-relatedness assessment of HAVS, it is necessary to evaluate the vibration exposure history (duration, intensity of vibration, which hand is mostly used, type of tools) and the severity of symptoms in both hands.
Raynaud scan has highest median of sensitivity with hand-chilling, but median of sensitivity decreased without the hand-chilling (Table 5). Considering this, hand-chilling is essential when performing Raynaud scan. Most of the reviewed studies used Raynaud’s scan with one-hand chilling method (Table 5). This is because the secondary Raynaud’s phenomenon is often due to systemic causes such as rheumatoid, hematological, and autoimmune factors; therefore, diagnosis can be made only by decreased blood flow on one hand.53 However, in the case of HAVS, the history of vibration exposure in both hands may differ depending on the method of using the vibrating tools. Therefore, it is necessary to match the decrease of blood flow in both hands with the history of vibration exposure. To compare both hands, authors recommend Raynaud’s scan with both-hand chilling. In Raynaud’s scan with both-hand chilling, Raynaud’s scan with non-chilling is done first, followed by Raynaud’s scan with both-hand chilling. By comparing these two results, the decrease of blood flow in both hands can be assessed. By considering objective results of Raynaud’s scan and vibration history, the verification of the HAVS will provide additional clinical, social and economic benefits.
In ROK, authors confirmed that the approval rate of compensation by Korea Labor Welfare Corporation was higher in the case that cold provocation test with finger skin color change and Raynaud’s scan than in the case that performed only the cold provocation test with finger skin color change.14 Authors think this is related to the high sensitivity and objective results of Raynaud’s scan. However, in most work-relatedness assessments, only the cold provocation test with finger skin color change was conducted.14 In many cases where work-relatedness assessment ends with negative result in the cold provocation test with finger skin color change, a trial is carried out.1516 The inconvenience of the subject, time loss, and social costs occur during this process. Therefore, if a vibration-exposed worker has symptoms of HAVS and results of the cold provocation test with finger skin color change is negative, an additional Raynaud’s scan should be performed to objectively assess the decrease of blood flow in both hands. Accurate diagnosis by Raynaud’s scan is essential part to decide work-relatedness of the disease.
In the studies that performed Raynaud’s scan, the detection parameters, radioactive isotopes, chilling time were different with no standard protocols which is adopted internationally and the number of articles was small. Therefore, additional research on Raynaud scan to unify protocols and more numbers of article is needed.
In this situation, more data are required to use Raynaud scan for compensation of work related disease. However, it is true that it shows that there are advantages than other methods.
CONCLUSIONS
Various diagnostic methods have been proposed to verify Raynaud’s phenomenon in HAVS, but an appropriate and objective gold standard test has not been established due to low test sensitivity, high test costs, and side complications. Raynaud’s scan is a test to verify Raynaud’s phenomenon in HAVS and it has relatively higher sensitivity and specificity than other tests, provides objective results, and is approachable in many hospitals. So we suggest using Raynaud’s scan as an alternative test when cold provocation test with finger skin color change is negative in vibration exposed worker.
Notes
Competing interests: The authors declare that they have no competing interests.
Author Contributions:
Conceptualization: Ha TW, Oh HC, Kim JW.
Data curation: Ha TW, Oh HC.
Investigation: Ha TW, Kim JW.
Writing - original draft: Ha TW.
Writing - review & editing: Oh HC, Kim JW.