Relationship between workplace violence and work-related depression/anxiety, separating the types of perpetrators: a cross-sectional study using data from the fourth and fifth Korean Working Conditions Surveys (KWCS)
Article information

Abstract
Background
Work is an inseparable element of a person’s life, and violence in the workplace has various effects on individual workers and companies. While most studies have focused on specific industries, very few studies have investigated the influence of workplace violence by co-workers. Therefore, this study aimed to evaluate the association between workplace violence and work-related depression/anxiety in various occupations by differentiating the perpetrators of violence as co-workers and clients.
Methods
This study was conducted based on data from the 4th and 5th Korean Working Conditions Surveys (KWCS). The experience of workplace violence was classified in terms of the perpetrator: workplace violence by co-workers and that by clients. Work-related depression and anxiety were assessed using questions about health problems related to depression and anxiety and whether the problems were related to work. Descriptive statistics, χ2 tests, and multiple logistic regression analyses were performed using the SPSS 26.0.
Results
After adjusting for sociodemographic characteristics (age, education, income, subjective health status) and occupational characteristics (occupation, weekly working hours, type of employment, size of workplace, and shift work), male workers with experience of workplace violence by co-workers were found to be at a higher risk of work-related depression/anxiety (odds ratio [OR], 11.52; 95% confidence interval [CI], 8.65–15.36). The same was confirmed for female workers (OR, 10.89; 95% CI, 7.90–15.02).
Conclusions
Employees who experienced workplace violence from co-workers were found to be more vulnerable to work-related depression/anxiety. Continuous contact between the victim and the perpetrator may occur, and the possibility of a secondary assault can frighten the victim. Appropriate prevention and intervention measures that focus on the perpetrators of violence are needed.
BACKGROUND
Work is an inseparable element of a person’s life, and an average wage worker spends approximately half of their waking hours at the workplace. According to the 2020 American Time Use Survey, employed persons work an average of 7.64 hours a day.1 Workplace refers to all places where workers need to be at or to go by reason of their work, where they are under the direct or indirect control of the employer.2 Violence in the workplace has various effects on individual workers and companies.
Workplace violence is defined as incidents in which employees are abused, threatened, assaulted, or subjected to other offensive behaviors in circumstances related to their work.3 In the United States, 2 million workers are exposed to workplace violence every year,4 and 17% of European employees report antisocial behavior in their workplaces.5 Fourteen% of male workers and 15.6% of female workers in Korea reported workplace mistreatment including workplace-related discrimination, violence, abuse, and harassment.6
Exposure to workplace violence adversely affects workers and companies. In addition to the direct physical damage that can occur due to the violence itself, workplace violence is harmful to the mental health of the victim, leading to depression, anxiety, somatic symptom disorder, post-traumatic stress disorder, and insomnia,789 and even significantly increases the incidence of cardiovascular disease.1011 From a corporate perspective, workplace violence hinders a company’s productivity and competitiveness. Labor loss is inevitable until an individual who has been assaulted recovers from the violence. Furthermore, damage to corporate culture leads to a decline in morale and work satisfaction among workers and drives them to seek another job.12
Recently, studies have been conducted on the effects of workplace violence on mental health in various occupations. In most studies, the participants were healthcare workers and service/sales workers, and the perpetrators of workplace violence were mainly patients/guardians or clients/customers.1314 The influence of workplace violence by colleagues or bosses may not have been adequately addressed in these studies. In this context, statistical definitions are being developed to classify workplace violence according to perpetrators.2
Immediate psychological coping responses to workplace violence can manifest as symptoms of depression and anxiety.1516 Therefore, this study aimed to evaluate the association between workplace violence and work-related depression/anxiety in employees aged 18 or older working in various industries in Korea, distinguishing violence according to its perpetrators.
METHODS
Data sources and study population
This study analyzed data from the 4th and 5th Korean Working Conditions Surveys (KWCS) conducted by the Korea Occupational Safety and Health Agency. The KWCS is a nationwide survey that has been conducted since 2006 to investigate the overall working environment and work-related exposure to hazardous elements, and to provide preliminary data for establishing policies to improve working conditions. The participants of the KWCS were an economically active population aged 15 years or older. The 4th KWCS examined 50,007 workers in 2014, and the 5th KWCS examined 50,205 workers in 2017.
Of the total 100,212 workers, 109 individuals aged under 18 were excluded, as were 33,690 self-employed or unpaid family workers, and 11,212 people who did not respond at least one of the questionnaires used in this study (Fig. 1).
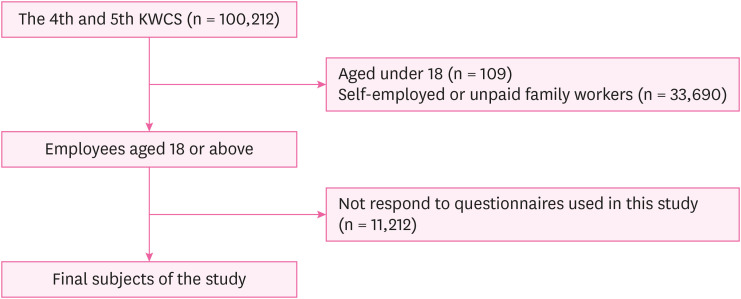
Flow chart of the selection of study subjects.
KWCS: Korean Working Conditions Survey.
Measurements
Work-related depression/anxiety
Work-related depression/anxiety was assessed using yes-or-no questions as follow, “Have you had any of the following health problems in the past 12 months?” and “[If yes] Did it happen because of your job?”. Those who answered “yes” to these consecutive questions about depression and anxiety were considered to have work-related depression/anxiety.
Workplace violence
The participants were asked whether they had experienced verbal abuse, unwanted sexual attention, or threatening or humiliating behavior during the past month, and whether the perpetrator was a client (students, patients, etc.) or a co-worker (colleague, boss, subordinate, etc.). Participants were also asked whether they had experienced physical violence, sexual harassment, bullying or harassment during the past 12 months. Those who answered “yes” to at least one of these questions were categorized as having experienced workplace violence.
Sociodemographic characteristics
Sociodemographic characteristics included sex, age (30, 30–39, 40–49, 50–59, and ≥ 60 years), educational level (below middle school graduate, high school graduate, and university graduate or higher), income (low 1/3, middle 1/3, and high 1/3), and subjective health status. Considering the wage gap over time, monthly income was classified into tertiles for both the 4th and 5th KWCS and later collected.
Occupational characteristics
Occupations were divided into three categories: white-collar (managers, professionals, and office workers), blue-collar (technicians, skilled agricultural and fishery workers, craft and related trade workers, plant and machine operators, elementary workers, and military personnel), and pink-collar (service and sales workers). Weekly working hours (< 40, 40–51, and ≥ 52 hours), type of employment (regular or temporary), size of the workplace (small [1–9 workers], medium [10–249 workers], and large [≥ 250 workers]), and shift work were also included as occupational characteristics.
Statistical analysis
A frequency analysis was performed to assess sociodemographic characteristics, occupational characteristics, experience of workplace violence, and perpetrators of violence among the study population. To compare the differences in the experience of workplace violence between those with and without work-related depression/anxiety, a χ2 test was conducted. The odds ratios (ORs) and 95% confidence intervals (CIs) for work-related depression/anxiety with respect to the experience of workplace violence were calculated using multiple logistic regression, adjusted for sociodemographic and occupational characteristics. All statistical analyses were performed using SPSS 26.0 (IBM Inc., Armonk, NY, USA).
Ethics statement
This study used only de-identified database disclosed to the public without personal identification information; therefore, neither approval by the Institutional Review Board nor obtainment of the informed consent is necessary.
RESULTS
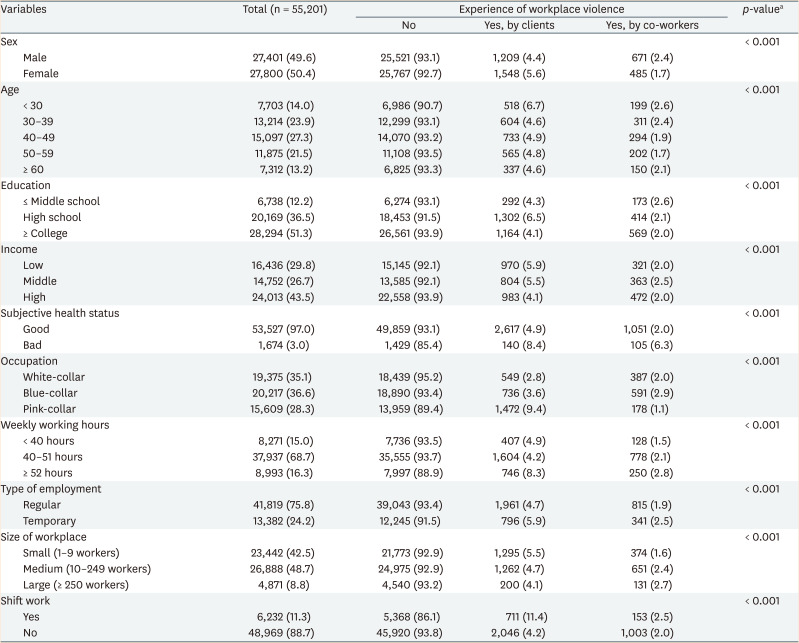
Table 1 displays the general characteristics of the 55,201 workers with respect to their experiences and perpetrators of workplace violence. The sample included slightly more women (50.4%) than men (49.6%). The youngest age group (< 30 years) had more experiences of workplace violence more than any other age group, both by clients (6.7%) and co-workers (2.6%). More than half the participants had a college degree or higher (51.3%).
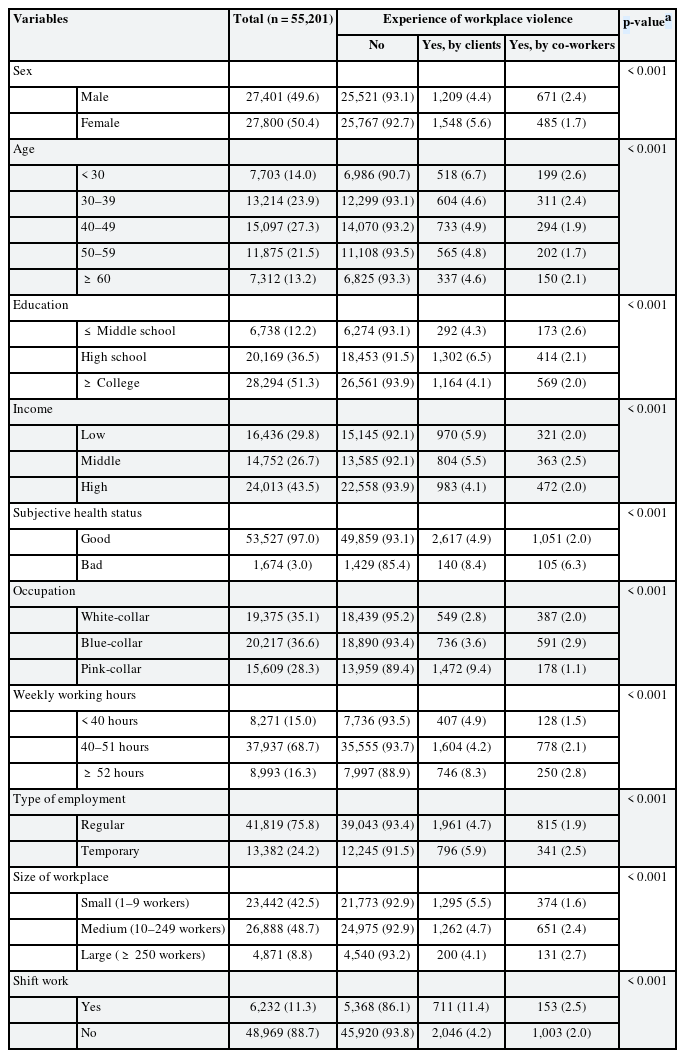
General characteristics of the study population according to their experience of workplace violence
The proportion of pink-collar workers who experienced workplace violence by clients was nearly three times (9.4%) that of white-collar workers (2.8%) or blue-collar workers (3.6%). Temporary workers, shift workers and those who worked 52 hours or more per week experienced more violence at their workplace. All sociodemographic and occupational characteristics showed statistically significant differences in the experience of workplace violence.
Table 2 compares the proportion of male and female workers with work-related depression/anxiety, depending on whether they had experienced workplace violence. Work-related depression/anxiety was more common among those who experienced workplace violence by co-workers than among those who experienced workplace violence by clients or those who did not experience workplace violence, in both male and female workers.
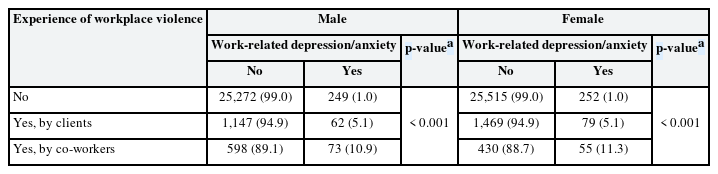
The proportion of work-related depression/anxiety with respect to the experience of workplace violence, stratified by sex
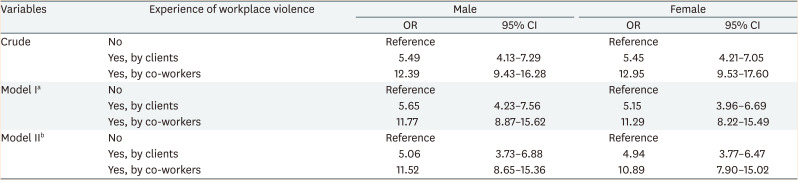
Table 3 shows the risk of work-related depression/anxiety in association with workplace violence, analyzed using multiple logistic regression. After adjusting for sociodemographic characteristics (age, education, income, and subjective health status) and occupational characteristics (occupation, weekly working hours, type of employment, size of workplace, and shift work), male workers with experience of workplace violence by co-workers were at a higher risk of work-related depression/anxiety (OR, 11.52; 95% CI, 8.65–15.36), compared to those with experience of workplace violence by clients (OR, 5.06; 95% CI, 3.73–6.88). The same was confirmed for female workers; the risk of work-related depression/anxiety was higher when the perpetrators of violence were co-workers (OR, 10.89; 95% CI, 7.90–15.02) than when they were clients (OR, 4.94; 95% CI, 3.77–6.47) (Fig. 2).
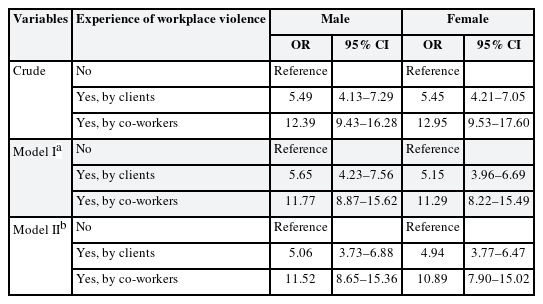
Multiple logistic regression analysis of work-related depression/anxiety according to workplace violence, stratified by sex
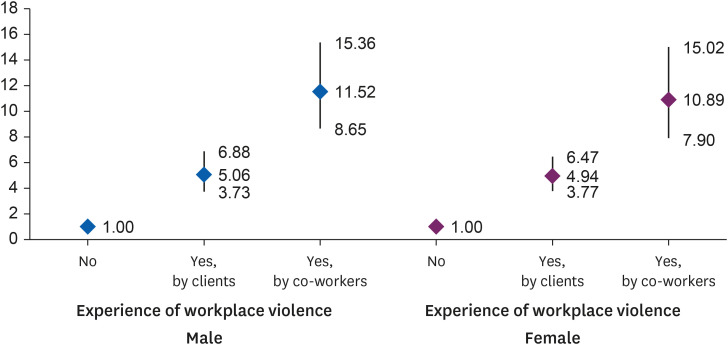
Odds ratios and 95% confidence intervals of work-related depression/anxiety according to the experience of workplace violence, adjusted by sociodemographic characteristics and occupational characteristics.
DISCUSSION
This study examined the association between workplace violence and work-related depression/anxiety among employees in all types of industries by distinguishing the perpetrators of violence into co-workers and clients. Women had more experiences of violence in the workplace than men, which was consistent with other study results,14 and both workplace violence by clients and co-workers were more frequent in the youngest age group, compared with other age groups. In terms of occupation, temporary workers, shift workers and those who worked more than 52 hours per week experienced more violence in their workplace. Pink-collar workers suffered more workplace violence by clients than workplace violence by co-workers, compared with white or blue-collar workers. This is presumed to be due to the nature of their work; pink-collar workers spend more time in contact with their clients than with their co-workers.
Our results showed that employees who experienced workplace violence were at a higher risk of work-related depression/anxiety than those who did not experience workplace violence, which is consistent with previous studies.10171819 Employees who experienced workplace violence by co-workers were at a higher risk of having work-related depression/anxiety than those who experienced workplace violence by clients or those who did not experienced workplace violence, regardless of gender. Similar results were obtained when analyzing only the employees who experienced workplace violence separated with respect to the perpetrators of violence. (Supplementary Tables 1 and 2). This is in line with previous studies on the association between workplace violence and depressive symptoms18 and sleep disturbances.20
Unlike workplace violence by clients, workplace violence by co-workers is followed by continuous contact between the perpetrator and victim; the latter might experience traumatic flashbacks and constantly feel distress at the workplace.21 A secondary assault by the same perpetrator is possible if the victim and perpetrator continue to work in the same environment. The effect of daily exposure to unpleasant co-workers is worse than temporal insults by clients.22
In this context, workplace violence should be addressed by considering the perpetrators. The negative aftermath of workplace violence by co-workers can be effectively mitigated through follow-up management measures,23 and it could even be prevented through appropriate precautions and in-house training. In companies where organizational policies for workplace violence prevention and control are well established, workers’ job satisfaction has increased, and the degree of depression has decreased.24
This study has a few limitations. First, the cross-sectional design of the study using the KWCS precludes causative interference. A direct causal relationship between workplace violence and work-related depression/anxiety could not be established through this study alone. However, when considering previous studies that reported the effects of workplace violence on mental health78910 and the depression and anxiety symptoms that occur in response to continuously applied stress,16 it would be reasonable to explain that work-related depression/anxiety can occur as a result of workplace violence.
Second, we did not distinguish between depression and anxiety symptoms. There are specific diagnostic criteria for major depressive disorder and anxiety disorders, but there is also considerable clinical overlap in symptoms, which often precede or follow each other.25262728 A certain degree of anxiety symptoms appears in 85% of patients with depression, and 90% of patients with anxiety disorders have depressive symptoms.29 Depression and anxiety often show similar clinical patterns through common neuroendocrine dysfunctions.30 In the initial phase, mental symptoms are ambiguous and nonspecific, which prevents people from visiting the clinic and makes the diagnosis difficult for physicians.
In addition, work-related depression/anxiety does not necessarily indicate a major depressive or anxiety disorder. The KWCS does not include questions to address psychiatric diagnostic criteria, such as the duration of depression, anxiety, or other accompanying symptoms, hence, various ranges of depression and anxiety could have been classified as merely experiencing symptoms. Therefore, in interpreting the results of this study, rather than assuming that workplace violence by co-workers causes major depressive or anxiety disorder, it would be appropriate to assume that workplace violence by co-workers has a greater negative association with workers' mental health manifested in the form of depression and anxiety symptoms.
According to the structure of the KWCS questionnaire, participants were required to respond to the perpetrators of workplace violence as either a co-worker or client, and it was not possible to analyze the cases of violence by both, which is also a limitation of this study.
Despite these limitations, this study distinguishes itself from other studies by its in-depth analysis of workplace violence by classifying it according to the perpetrators. Although many people are aware of the aftermath and problems of workplace violence, the actual situation of workplace violence by co-workers that occurs inside the workplace is not well understood. This may be due to an attempt to find the cause of violence in the individual victim and perpetrator, or a culture that shy away from incidents within the company.3132 Only recently have they received public attention as reports of deaths with workplace violence. Few studies have been conducted to classify the perpetrators of workplace violence and further studies are needed to avoid unfortunate losses.
Moreover, in terms of prevention and intervention, workers at the symptomatic stage were identified and analyzed before being diagnosed with a disease. Depression and anxiety are mental illnesses with the highest, gradually increasing prevalence, worldwide. In 2015, 4.4% of the global population suffered from depression, 3.6% suffered from anxiety disorders, and the same was true for Koreans—4.1% suffered from depression and 3.8% suffered from anxiety disorders.33 Some patients with these mental disorders are reluctant to undergo treatment; however, under an appropriate treatment regimen, they can maintain optimal functioning at work, at home, or in relationships with others.3435 If these disorders are left untreated, they may lead to suicide, which has a ripple effect on those related to the deceased.36 Through appropriate intervention at the pre-disease stage, it is possible to prevent progression to major depressive disorder or anxiety disorders. The prevention, early detection, and treatment of these disorders can provide several benefits at the individual and social levels.
In addition, the data used in this study were obtained from the KWCS, and we were able to compare large groups through a nationwide survey.
As workplace violence and subsequent incidents have become an emerging problem, countries worldwide are taking cognizance of this serious social issue that can no longer be neglected, and are preparing various measures to prevent it.37 In Korea, through the enactment of the Workplace Harassment Prevention Law, attempts have been made to prevent workplace violence and the resulting loss of labor.38 Considering the influence of individual workers’ mental health on workers’ lives, the company, and society, workplace violence should be eradicated. Preventive or follow-up measures that focus on perpetrators of violence are considered helpful. Further research in this field is required in the future.
CONCLUSIONS
Workplace violence by co-workers was more strongly associated with work-related depression and anxiety than that by clients. Appropriate prevention and intervention measures are needed to prevent losses caused by workplace violence with respect to the perpetrators of violence.
ACKNOWLEDGEMENTS
The study used data from the 4th and 5th Korean Working Conditions Survey (KWCS), which is open to researchers on request.
Notes
Funding: This work was supported by the research fund from Soonchunhyang University.
Competing interests: The authors declare that they have no competing interests.
Author Contributions:
Conceptualization: Lee NR.
Data curation: Lee NR, Kim SW, Joo JH, Lee JH.1
Formal analysis: Lee NR.
Supervision: Lee JH,2 Lee KJ.
Writing - original draft: Lee NR.
Writing - review & editing: Lee NR, Lee JH,2 Lee KJ.
Lee JH,1 Jae-Han Lee; Lee JH,2 June-Hee Lee.
References
SUPPLEMENTARY MATERIALS
Supplementary Table 1
The proportion of work-related depression/anxiety with respect to the perpetrator of workplace violence, stratified by sex
Supplementary Table 2
Multiple logistic regression analysis of work-related depression/anxiety according to the perpetrator of workplace violence, stratified by sex