Hospital admissions due to endocrine diseases in Korean male firefighters
Article information

Abstract
Background
The aim of this study was to investigate the relationship between occupational exposure to various hazards and hospital admission due to endocrine diseases in Korean male firefighters.
Methods
From 2000 to 2008, former and current male firefighters registered in the Korean National Emergency Management Agency were investigated based on their hospitalized health insurance admission data for the same period. Admission data for endocrine, nutritional, and metabolic diseases were obtained from the Korean National Health Insurance Service database. Standardized admission ratio (SAR) with reference to the general population of Korean men was analyzed.
Results
SAR for firefighters with endocrine, nutritional, and metabolic diseases was 0.56 (95% confidence interval [CI]: 0.49–0.65), which was significantly less than that of the general population of Korean men. For those with endocrine, nutritional, and metabolic diseases, SARs for those with a history of fire suppression tasks and those without experience of fire suppression tasks were 0.58 (95% CI: 0.49–0.68) and 0.53 (95% CI: 0.40–0.70), respectively.
Conclusions
The admission rate of Korean male firefighters due to endocrine, nutritional and metabolic diseases was significantly lower than that of the general Korean men population, the hazardous potential of endocrine disruptors remains an open question. Further studies of firefighters with longer follow-up are needed.
BACKGROUND
In modern society, environmental pollutants are causing major health concerns, because they can lead to public health problems.1 Some pollutants are endocrine-disrupting chemicals, including natural and synthetic chemicals found in our environment. They can interfere with body hormone synthesis, secretion, activity, and metabolism.2
Firefighters can be exposed to these endocrine-disrupting chemicals and heavy metals frequently due to their occupation as they have to work at disaster sites.3 At fire sites, dioxin, heavy metals including lead, cadmium, mercury, persistent organic pollutants (POPs) like polybrominated diphenyl ethers (PBDEs), brominated flame retardants, and tetrabromobisphenol A can act as endocrine disruptors.4567 It has been reported that exposure to dioxin can affect thyroid function and increased the prevalence of diabetes.89 There is a report about exposure to lead and cadmium can affect changes in thyroid indexes.10 These heavy metals also affect the onset and worsening of diabetes.11 Also reduced thyroxine (T4) level from exposure to organophosphate flame retardants has been reported.12 Moreover, firefighters also perform night shifts that affect the endocrine system.1314
It is clear that firefighters are exposed to endocrine disruptors. However, it is difficult to quantitatively evaluate such exposure.15 In addition, the onset period of endocrine diseases due to chronic exposure to endocrine disruptors varies greatly from person to person. Despite reports on the association between various endocrine diseases and exposure to flame retardants from the fire sites, there is a lack of research on endocrine diseases of firefighters. Therefore, the objective of this study was to investigate the risks of endocrine diseases related with occupational exposure to various hazards in Korean male firefighters through the comparison with the general population.
METHODS
Study population
From 2000 to 2008, a total of 34,875 former and current male firefighters registered with the Korean National Emergency Management Agency (NEMA) were investigated based on hospitalized health insurance admission data for the same period (Fig. 1). Female firefighters were excluded, because the number of women affected by endocrine diseases was very small. If a firefighter enters the National Fire Agency before 2000, then the cohort start date is January 1, 2000; other firefighters were calculated starting from the date of the firefighter's first day of service. Person-years were calculated starting from the cohort start date and ending on one of followings: December 31st 2008, the first admission date upon diagnosis of endocrine, nutritional and metabolic diseases, retirement, and death, whichever came first. Data provided by the NEMA included resident registration number, affiliated office and department, rank, appointment year and month, working period (as of December 31, 2008, month), working period by experience job, and main job. The presence of fire suppression tasks experience was defined as firefighters with fire suppression tasks experience regardless of their main job among firefighters with more than one year of work experience. However, we could not distinguish between the different task assignments.
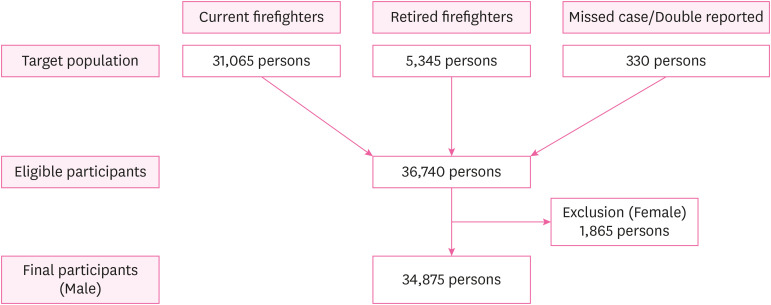
Flowchart of firefighters as study subjects.
Health outcome and exposure data
Admission data for endocrine diseases were obtained from the Korean National Health Insurance Service (NHIS) database. Among data provided by the NEMA, the resident registration number of firefighters were submitted to the NHIS and data from 2000 to 2008 were obtained. As for the reference population, 2% of the insured were randomly selected by considering the region, and age distribution of firefighters (from 20 to 75 years old) using NHIS 2000 database. Data included admission rates and diagnoses of endocrine diseases based on World Health Organization 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10) criteria.
Disease codes E00–E90 in ICD-10 criteria were analyzed for endocrine, nutritional, and metabolic diseases. Sub-categories of E codes included E00–E07 for disorders of the thyroid gland, E10–E14 for diabetes mellitus, E15–E16 for other disorders of glucose regulation and pancreatic internal secretion, E20–E35 for disorders of other endocrine glands, E40–E46 for malnutrition, E50–E64 for other nutritional deficiencies, E65–E68 for obesity and other hyperalimentation, and E70–E90 for metabolic disorders. Of these, thyroid disorder (E00–E07), diabetes (E10–E14), and metabolic disorder (E70–E90) were analyzed. Categories with less than 10 cases including other disorders of glucose regulation and pancreatic internal secretion (E15–E16), disorders of other endocrine glands (E20–E35), malnutrition (E40–E46), other nutritional deficiencies (E50–E64), and obesity or other hyperalimentation (E65–E68) were excluded to enhance the statistical power.
According to their age, subjects were divided into five age groups: 20s, 30s, 40s, 50s, and 60s and over. Depending on the working period, they were divided into five groups: less than 1 year, 1 year and more but less than 5.0 years, 5.0 years and more but less than 10.0 years, 10.0 years and more but less than 20.0 years, 20 years and more. According to their current main job, they were divided into four groups: fire suppression, rescue, driving, and others.
Statistical methods
Multiple admissions of the same patient for the same endocrine disease category subclass were considered a single admission. Multiple admissions of the same patient for different endocrine disease category subclasses were regarded as separate admissions. The same principles regarding the number of admissions were applied to both the male firefighter cohort and the reference population. The number of admission records for endocrine, nutritional, and metabolic diseases of male firefighters that occurred during the period was divided by that of the reference population and calculated as a standardized admission ratio (SAR). The SARs with 95% confidence intervals (CIs) were estimated by the person-years and mortality computation software.16
Ethics statement
This study was approved by the Dongguk University Ilsan Hospital Institutional Review Board (2009-1-17). The need for informed consent was waived by the board.
RESULTS
General characteristics
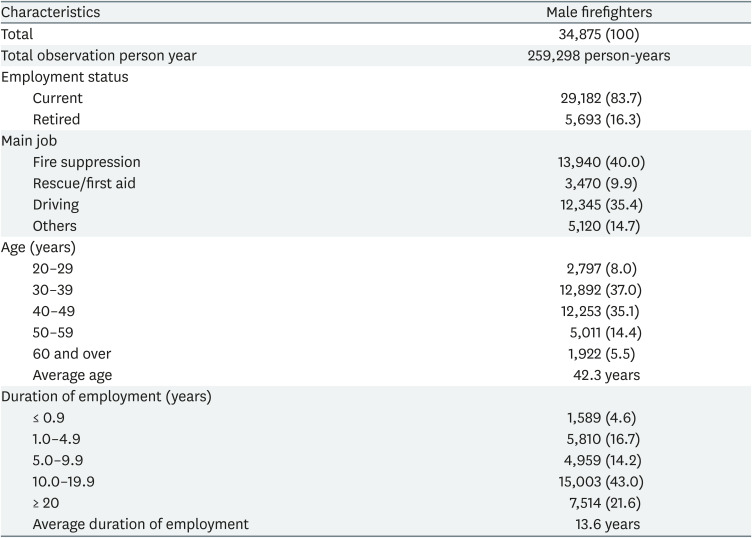
The total study population was 34,875 male firefighters. The number of observation person-year was 259,298 (Table 1). Among them, 29,182 (83.7%) firefighters were incumbent and 5,693 (16.3%) firefighters were retired depending on the employment status. By the main job, fire suppression has the highest proportion at 40.0% with 13,940 people, followed by driving at 35.4% with 12,345 people, other tasks at 14.7% with 5,120 people, and rescue/first aid at 9.9% with 3,470 people. The average age was 42.3 years. There were 2,797 (8.0%) people in their 20s, 12,892 (37.0%) in their 30s, 12,253 (35.1%) in their 40s, 5,011 (14.4%) in their 50s, and 1,922 (5.5%) in their 60s and over. Regarding the working period, the average was 13.6 years, with 1,589 (4.6%) firefighters having less than 1.0 year, 5,810 (16.7%) firefighters having more than 1.0 year but less than 5.0 years, 4,959 (14.2%) firefighters having more than 5.0 years but less than 10.0 years, 15,003 (43.0%) firefighters having more than 10.0 years but less than 20.0 years, and 7,514 (21.6%) firefighters having more than 20.0 years.

General characteristics of male firefighters (As of Dec. 31, 2008)
SARs in male firefighters
The SAR for endocrine, nutritional, and metabolic diseases was 0.56 (95% CI: 0.49–0.65), which was significantly smaller than that of the general population of Korean men (Table 2). Among the endocrine, nutritional and metabolic diseases, only SAR of thyroid disorders (1.48, 95% CI: 0.97–2.15) was higher than that of the reference group without statistical significance. However, those with diabetes (0.50, 95% CI: 0.42–0.59) and other metabolic disorders (0.55, 95% CI: 0.32–0.87) were lower than those of the reference group with statistical significance.

SARs for endocrine, nutritional and metabolic diseases
SARs according to the presence or absence of fire suppression tasks
For SAR with endocrine, nutritional, and metabolic diseases, SAR for firefighters with a history of fire suppression tasks and those without experience of fire suppression tasks were 0.58 (95% CI: 0.49–0.68), and 0.53 (95% CI: 0.40–0.70), respectively. Both groups were significantly less hospitalized than the general population of Korean men (Table 3).

SARs according to the presence or absence of fire suppression tasks
SAR for endocrine, nutritional, and metabolic diseases of the presence of fire suppression tasks
For SAR with endocrine, nutritional, and metabolic diseases, SAR for firefighters with the presence of fire suppression tasks with the absence of fire suppression tasks as the reference were 0.96 (95% CI: 0.69–1.34) (Table 4).

SARs for endocrine, nutritional and metabolic diseases of presence of fire suppression tasks group with absence of fire suppression tasks group as the reference
DISCUSSION
Various studies have reported that some POPs have the potential to disrupt multiple endocrine systems. However, these studies were performed in a laboratory situation. Thus, their toxicological profiles were insufficient for an adequate human risk assessment.17 Heavy metals like lead and cadmium are well-known endocrine disrupters that firefighters are often exposed to.18 There are several reports about lead and cadmium's association with diabetes, but its metabolic health effects of exposure are incomplete.111920 Moreover, shift work has been reported as a risk factor for diabetes and metabolic disorders.21
Despite exposure to endocrine disrupters in firefighters, this study showed that the SAR for male firefighters with endocrine, nutritional, and metabolic diseases was significantly lower than that of the general Korean male population. In addition, the SARs for those with diabetes and metabolic disorders were significantly lower compared to those in the general Korean male population. To our best knowledge, we could not find any human studies that evaluated a relationship between endocrine disruptor exposure at the fire scene and endocrine disease.
In the case of diabetes, a low incidence rate was found to be more closely related to physical conditions such as weight, body mass index (BMI), and lifestyle habits rather than to the effect of shift work in an actual disease outbreak, consistent with previous studies showing that lifestyle habits had greater effects on diabetes and metabolic diseases than shift work.222324 One study has compared German firefighters and shift workers in other occupations and reported that firefighters are much healthier.22 One study in the United States has found that the prevalence of metabolic syndrome in firefighters is lower than that in the general population.23 On the ground that lifestyle habits of firefighters have a greater influence than shift work, one study of Japanese firefighters and police officers has noticed that their type 2 diabetes mellitus might be caused by an increase of BMI.24
These healthy worker effects could also be seen in this study. There is no concrete evidence that indicates that firefighters are healthy workers compared to other shift occupation groups, although previous reports have shown that the health status and lifestyle factors of Korean firefighters were significantly better than those of Korean adult men.25 Therefore, further research on the effects of endocrine disruptor exposure at the fire scene on diabetes and metabolic diseases are needed in the future.
However, there is a possibility of endocrine disruptors are likely to have more impact on disorders of the thyroid gland. Although there was no significant difference, crude SARs for male firefighters with disorders of the thyroid gland was higher than the general population. This is probably due to the widened CI associated with the small number of subjects having disorders of the thyroid gland. On the basis of supporting this, female firefighters in San Francisco, California with a primary job task of fire suppression have also been reported to show decreased T4 levels.26
Many reports have shown that exposure to PBDE is associated with changes in thyroid hormone levels.67 Flame retardants of organophosphate are associated with decreased T4 levels.12 As heavy metals with the relationship with thyroid diseases, there is a report of lead and cadmium exposure can affect higher thyroid antibodies and thyroid dysfunction in Chinese women.10 There is also a report of increased hyperthyroidism of foundry workers exposed to lead.27 If the follow-up period is prolonged and the number of cases increases, there is a possibility of a significant increase of SARs.
This study has some strengths. First, in accordance with the Framework Act on Health, Safety, and Welfare of Fire Officials, our cohort included most of the firefighters defined by the NEMA and was thus representative. Second, the quality of the comparative group was excellent because the majority of Koreans were enrolled in health insurance was conducted at the national level.28 Third, this study used admission data and ICD-10 classification criteria. Because of this, the diagnosis was very accurate. For example, a previous study showed the diagnosis validity of 87.2% (95% CI, 83.8–90.7%) for admission episodes and 72.3% (95% CI, 67.4–77.2%) for outpatient cases in Korean diabetes patients.29 In addition, measurement or information bias such as recall bias, memory decay bias could be completely excluded. Thus, an accurate admission rate could be obtained.
This study also has some limitations. First, those with diabetes, thyroid diseases, and metabolic disorders are often treated in an outpatient department rather than admission, so that we likely underestimate the number of cases of endocrine disease in the study population. For example, in 2003, the annual admission rate in Korean diabetes patients was 10.3%.29 However, this limitation would not affect the SAR, because the admission data was also used for the ascertainment of morbidity in the reference group. Also, it reflects the number of severe patients well. Second, our study was based on hospital admission data with no controls for lifestyle factors such as smoking, alcohol drinking,30 and exercise,31 which might have affected endocrine diseases. In particular, smoking is known to be an influencing factor in thyroid diseases.32 Third, the evaluation of firefighters' exposure was insufficient. It was impossible to know the actual number of fire extinguishing or the number of dispatches to the fire sites that might have harmful substances. Moreover, the main job category was defined based on the job during the 9 years of the investigation period. Thus, there was a limitation to show that the firefighters had worked for a considerable amount of time for fire suppression for occupational disease to appear. Lastly, although the number of subjects and person-years in this study was large, the observation period was short. The period between exposure to an endocrine-disturbing substance and the onset of the disease is not known exactly. However, it is a well-known fact that for a disease to develop after chronic exposure to hazardous substances, a considerable period of time is needed.33
CONCLUSIONS
This study showed that the SARs for those with endocrine, nutritional, and metabolic diseases in firefighters and those with fire suppression tasks were lower than those of the general population of Korean men. However, in case the of thyroid disease, it is difficult to draw a conclusion. To evaluate more detailed relevance, a longer-term follow-up study is warranted in the future.
Notes
Funding: This work was supported by the Soonchunhyang University Research Fund.
Competing interests: The authors declare that they have no competing interests.
Author Contributions:
Conceptualization: Ryu S.
Data curation: Ryu S, Kim K, Lee YJ, Jang EC, Kwon SC, Ahn YS, Min YS.
Formal analysis: Ryu S, Kim K, Lee YJ, Jang EC, Kwon SC, Ahn YS, Min YS.
Investigation: Ryu S, Kim K.
Writing - original draft: Ryu S.
Writing - review & editing: Min YS.
Abbreviations
BMI
body mass index
CI
confidence interval
NEMA
National Emergency Management Agency
NHIS
Korean National Health Insurance Service
PBDE
polybrominated diphenyl ethers
POP
persistent organic pollutant
SAR
standardized admission ratio
WHO
World Health Organization