A case series of flight attendants at risk of COVID-19 in South Korea in 2020
Article information

Abstract
Background
Coronavirus disease 2019 (COVID-19) has infected many individuals worldwide. Individuals in contact with unspecified people during their work, may be at risk of occupational exposure. On June 22, 2020, 1,435 overseas patients were identified in the Republic of Korea. Considering the influx of overseas patients, aircraft-mediated COVID-19 transmission is a major concern.
Case presentation
We presented two flight attendants diagnosed with COVID-19 who shared the crew's resting area and ground transportation, and discussed the risks experienced by flight attendants.
Conclusions
Biosafety guidelines for cabin crews should be intensified, and their COVID-19 risks must be further investigated. Policymakers must consider comprehensive surveillance systems for workers with high risks of occupational exposures and transmissions, such as flight attendants.
BACKGROUND
Coronavirus disease 2019 (COVID-19) has infected over 8 million individuals worldwide as of June 2020 and resulted in more than 0.4 million deaths. Since the local outbreak in Wuhan, China, overseas importation of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which causes COVID-19, remains a key source of domestic epidemics globally [12]. COVID-19 can affect all individuals directly or indirectly. However, individuals such as flight attendants, who are in contact with many unspecified individuals as part of their work, are considered to have a higher risk of occupational COVID-19 exposure. In the case of flight attendants, contacts with international travelers put them at potentially higher risk. As of June 22, 2020, a total of 1,435 out of 12,438 patients was identified as overseas patients in the Republic of Korea (ROK) [2]. Considering the influx of overseas patients, aircraft-mediated COVID-19 transmission is of great concern.
The ROK, a leading nation in the fight against COVID-19, has established a close epidemiologic inspection system, and all patients are investigated by local authorities. Authorities share patients' epidemiological information clearly and transparently for public welfare. We examined two flight attendants infected with COVID-19 using public information, and discussed their risks for COVID-19.
CASE PRESENTATION
Case A
A 25-year-old woman working for Korean Air as a cabin crew member became ill on February 21, 2020, with symptoms of cough and a mild fever. She was examined for COVID-19 on February 24, 2020 and was confirmed positive the next day (Table 1).

Clinical information in cases A and B
Thorough epidemiologic investigations suggested in-flight disease transmission as the source of infection. On February 15, 2020, 39 Korean Catholic pilgrims boarded KE958 (B777) from Tel Aviv, Israel to Incheon, ROK. Soon after their return to ROK, 30 pilgrims were diagnosed with COVID-19. The flight attendant had worked during this flight. Moreover, there were no other identified sources. After the flight, she flew back and forth from Incheon, ROK, to Los Angeles, USA, between February 19 and February 22, 2020. On route from Los Angeles (February 20, KE012, A380), she began to feel ill and was subsequently diagnosed with COVID-19 on February 25, 2020 (Table 2).
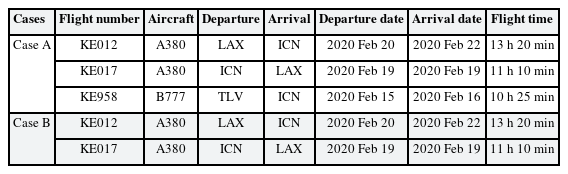
Flight characteristics
Case B
A 36-year-old woman who worked on the same flights (KE012 and KE017) showed symptoms including coughs, a mild fever, and myalgia on March 6, 2020. She was diagnosed with COVID-19 on the same day (Table 1).
After the first flight attendant was diagnosed with COVID-19, a 2-week self-quarantine period was imposed on all crew members, including the second flight attendant. Of the 30 crew members, only she was diagnosed with COVID-19 on the eleventh day of quarantine. She did not have any known epidemiological links to COVID-19, other than contact with the first flight attendant. During both flights (KE012 and KE017, A380), the second flight attendant worked on the upper deck (prestige class), and the first flight attendant worked on the main deck (first and economy class) (Table 2). They shared the crew's resting area and ground transportation after the first flight attendant had developed symptoms.
Epidemic response of Korean Air
Korean Air shut down its Incheon Operation Center on February 25, 2020 and disinfected the aircrafts. All 30 crew members entered self-quarantine for 2 weeks, which was later extended by an additional week after the second flight attendant was diagnosed with COVID-19 (Fig. 1).
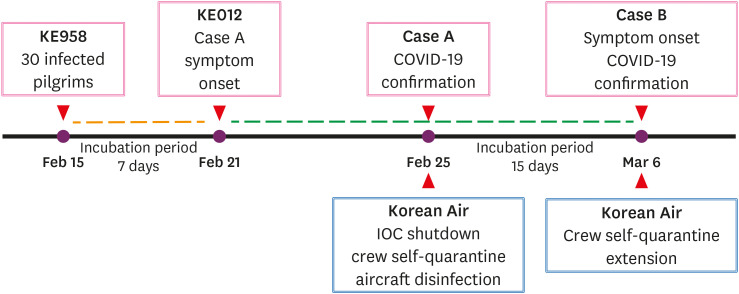
Flowchart of events.
COVID-19: coronavirus disease 2019.
Ethics statement
The study was approved by the Institutional Review Board of Kangbuk Samsung Hospital (KBSMC 2020-06-044), which exempted the requirement of informed consent owing to the use of public information.
DISCUSSION AND CONCLUSION
Occupationally, flight attendants contact many unspecified individuals and visit countless locations. Contacts may be encountered during the flights or on the ground before and after flights, including at airline operation centers, airports, accommodations, transportations, and local stopover areas. In the aircrafts, flight attendants encounter random passengers in cabins and may be in close contact with other flight attendants, especially in the galleys and the crew's resting areas. Therefore, they can contract COVID-19 by inter-transmission (via external environments), as in case A; or intra-transmission (among themselves), as in case B. In particular, the aircraft cabins, where flight attendants contact random individuals and their belongings, as well as stopover sites and the crew's resting areas, where flight attendants relax and are unsupervised, pose the highest exposure risks.
Generally, cabin air quality has a high purity level because the recirculated air passes through high-efficiency particulate air (HEPA) filters. The International Air Transport Association (IATA) considers the risk of COVID-19 transmission among passengers to be very low for several reasons: 1) passengers are seated facing forward and not toward each other, 2) the back of seats serve as a physical barrier, 3) passenger movements are limited onboard, and 4) the direction of air flow is from the ceiling to the floor [3]. However, this risk assessment neglects the possibility of transmission via contaminated surfaces and also underestimates people's onboard activities.
The cases of in-flight transmission of COVID-19 between passengers and crew members have recently been reported [4]. The Centers for Disease Control and Prevention (CDC) and Federal Aviation Administration (FAA) recommend that crew members with known exposure to COVID-19 do not work for 14 days, even if they have no symptoms. Besides the risk of in-flight transmission, transmission from the external environment may also be significant considering that flight attendants' activities extend beyond the cabin environment. The CDC and FAA recommend providing crew members with private ground transportations for travelling back and forth hotels near the airport, and that their rooms are sanitized in advance of the crew's arrival. However, current guidance lacks surveillance for asymptomatic infections through uncertain or undetermined transmission routes [5]. Considering the substantial occupational risks of flight attendants, in addition to general risks that the public is exposed to, surveillance should not only rely on self-reports of symptoms or exposures to COVID-19. Authorities should consider mandatory COVID-19 testing of all flight attendants prior to take-off, regardless of symptoms or exposures to COVID-19.
International air travel of travelers has been collapsing for several months during the COVID-19 pandemic. Recently, some nations and airlines are preparing to resume operations. As flight attendants repeatedly contact many unspecified individuals, their protection against COVID-19 risks is of utmost importance. By protecting the flight attendants, another COVID-19 wave may also be prevented. Biosafety guidelines for cabin crews should be intensified, and their COVID-19 risks must be further investigated. Policymakers must consider comprehensive surveillance systems for workers with high risks of occupational exposures and transmissions, such as flight attendants.
ACKNOWLEDGMENTS
The authors would like to thank HJK, III, and EJN for advice on the occupational characteristics of flight attendants.
Notes
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Competing interests: The authors declare that they have no competing interests.
Authors contributions:
Conceptualization: Lee C.
Data curation: Mun E.
Investigation: Mun E, Kim YM, Han B.
Writing - original draft: Mun E, Lee C.
Writing - review & editing: Jeong J, Kim W, Lee C.
Abbreviations
CDC
Centers for Disease Control and Prevention
COVID-19
coronavirus disease 2019
FAA
Federal Aviation Administration
HEPA
high-efficiency particulate air
IATA
International Air Transport Association
ROK
Republic of Korea

