Effect of night shift work on the control of hypertension and diabetes in workers taking medication
Article information

Abstract
Background
Night shift work induces physiological and psychological stress by altering sleep and biological rhythms and is associated with hypertension, diabetes, obesity, and cardiovascular diseases. Few studies have been conducted on the control of hypertension and diabetes. This study aimed to examine the effect of night shift work on the control rate of hypertension and diabetes.
Methods
Subjects comprised workers aged 20–65 years who underwent specific health examination at a single facility in seven different affiliated examination centers from 1 January to 31 December 2016. Workers were categorised into day workers and night shift workers. Demographic and medical history were taken, and physical examination was done. Blood pressure (BP) and fasting glucose were measured. The control rate of each disease was evaluated based on treatment goals presented in the treatment guidelines of the Korean Society of Hypertension and the Korean Diabetes Association (systolic BP < 140 mmHg and diastolic BP < 90 mmHg; fasting glucose ≤ 130 mg/dL).
Results
Among 631,418 subjects, 11.2% (70,450) were night shift workers. Of whom 6.1% (4,319) were taking antihypertensive medication and 2.5% (1,775) were taking diabetes medication. Among patients taking antihypertensive medications, the proportion of those whose BP was controlled to suit treatment goals was 81.7% (26,635) of day workers and 77.4% (3,343) of night shift workers, which was significantly different (p < 0.001). Among patients taking diabetes medications, the proportion of those whose blood glucose was controlled to suit treatment goals was 37.4% (4,489) of day workers and 36.5% (647) of night shift workers, but the difference was not significant. The control rates for patients taking antihypertensive medications (odds ratio [OR]: 0.74, 95% confidence interval [CI]: 0.68–0.80) were lower among night shift workers than day workers with adjustment for age, sex, smoking history, alcohol consumption, exercise, and obesity. However, there were no differences in control rates for patients taking diabetes medications (OR: 0.99, 95% CI: 0.87–1.10) between day workers and night shift workers.
Conclusions
Night shift work can have an effect on the uncontrolled BP in workers taking antihypertensive medications. Therefore, additional efforts for disease control are necessary for night shift workers with hypertension.
BACKGROUND
The proportion of workers who perform shift work in Korea is continuously increasing from 7.2% in 2006 to 9.7% in 2017 [1]. According to the 2017 statistics, many shift works is done in order of transportation, electricity and gas industry, and arts and sports industry [2]. In the traditional manufacturer-centered industrial structure, shift work was implemented to maximise production. However, the economic structure has changed, emphasizing service and information, pattern changes in consumer culture; with this, our society has evolved to a 24/7 society in which the working hours are 24 hours per day, 7 days per week. Workers are required to work longer hours and more shifts including nights or weekends [3].
Night shift work is a specialised type of work. The Ministry of Employment and Labor defines night work as performing 8 hours work between 10 pm and 6 am the next day that includes continuous work for at least 5 hours between midnight and 5 am for at least 4 times a month and for a total of 6 months, or performing work between 10 pm and 6 am the next day for ≥ 60 hours per month on average for 6 months [4].
Night shift work induces mental, behavioural, and physiological stress from changes in the sleep rhythm and sleep deprivation. Physiologically, a diurnal pattern of maintenance of reduced blood pressure (BP) is usually observed during sleep (referred to as ‘nocturnal dip’) due to the mechanisms of supine position, muscle relaxation, and lowered tone of sympathetic nerves. However, changes in sleep due to night work make nocturnal dip incomplete [5].
Night shift work is closely related to the occurrence of atherosclerosis, diabetes, and metabolic syndrome in addition to sleep changes, and is ultimately known to be an important cause of cardiovascular diseases [67]. The shift work including night work is well known an important risk factor of hypertension and closely related to the occurrence of diabetes [89]. Sleep deprivation and poor quality sleep disrupts the circadian rhythm and autonomic balance. Its makes BP control difficult and also reduces insulin sensitivity and exacerbates insulin resistance [101112]. In type 1 diabetes patients, diabetes control is affected by shift work [13]. There are several reports about the relation of night shift work with hypertension and diabetes. However, studies examining how effective hypertension and diabetes are controlled in night shift workers are a few.
In this study, we aimed to examine whether night shift work have an effect on the control rate of hypertension and diabetes.
METHODS
Subjects
In this cross-sectional study, we targeted 657,056 workers who received specific health examinations at a single facility in 7 different affiliated examination centers between 1 January and 31 December 2016. Work type was identified through a questionnaire of specific health examination specified by Korea Occupational Safety and Health Agency [14]. Subjects who responded with fixed night work or shift work (second shift, third shift, 24-hours interval work, etc.) or irregular work type on the survey were defined as night shift workers, according to the definition of night work by the Ministry of Employment and Labor [4]. Others were categorised as day workers. Finally, we included those aged 20–65 years, an age group of major economic activity, as the subjects of the study, resulting in a total of 631,418 subjects [15]. Among them those who are currently taking antihypertensive medication were categorised as subjects taking antihypertensive medications, resulting in 36,914 subjects. Those who are currently taking diabetes medication were categorised as subjects taking diabetes medications, resulting in 13,826 subjects.
Definitions of variables
Age was categorised into 20–29, 30–39, 40–49, 50–59, and 60–65 years. Subjects with a smoking history were categorised into non-smokers, ex-smokers, and current smokers. For alcohol consumption, those who drank > 1 time per week were categorised as drinkers [16]. For exercise, those who performed > 150 minutes of mid-level exercise or 75 minutes of high-level exercise per week were categorised as health exercisers [17]. Body mass index (BMI) was obtained by measuring height and weight, and those with BMI ≥ 25 kg/m2 were defined as obese, based on the Asian standards defined by the World Health Organization [18]. Subjects were categorised through surveys. Subjects who had been taking treatment were categorised as subjects with medications.
Assessment of hypertension and diabetes and definition of control rate
The examinees were asked to receive examinations after taking sufficient rest before the examination. BP was measured using an automatic BP device after the subject had maintained 5 minutes of stable condition while sitting. If systolic blood pressure (SBP) was ≥ 120 mmHg or diastolic blood pressure (DBP) was ≥ 80 mmHg in the first examination, re-examination was performed after more than 2 minutes [19]. If SBP was ≥ 140 mmHg or DBP was ≥ 90 mmHg in the first examination, second examination was performed after two weeks. The second examination was performed in the same way as the first examination. According to the diagnostic guidelines of the Korean Society of Hypertension, BP is controlled if SBP is < 140 mmHg and DBP is < 90 mmHg, whereas BP is uncontrolled if SBP is ≥ 140 mmHg or DBP is ≥ 90 mmHg [20]. For blood glucose measurements, blood sample was taken after at least 8 hours of fasting prior to specific health examination [19]. If the fasting glucose level is > 130 mg/dL in the first examination, second examination was performed after 2 weeks. The second examination was performed in the same way as the first examination. Following the 2015 diabetes diagnostic guidelines of the Korean Diabetes Association, diabetes is controlled if the fasting glucose level is ≤ 130 mg/dL, whereas diabetes is uncontrolled if the fasting glucose level is > 130 mg/dL [21]. Control rate was evaluated if subjects taking medications had control of their disease.
Statistical analyses
Information on age, sex, smoking history, alcohol consumption, exercise, obesity, BP and fasting glucose level were compared between day workers and night shift workers using the χ2 or t-tests.
To examine the effect of work type on BP and blood glucose control between subjects currently on medication and whose hypertension and diabetes are controlled, we performed a multivariate logistic regression analysis, with adjustment for age, sex, smoking history, alcohol consumption, exercise, and obesity. Statistical significance was set at p < 0.05. IBM and SPSS version 25.0 software (IBM Corp., Chicago, IL, USA) were used for statistical analyses.
Ethics statement
This study was approved by the Institutional Review Board of Dankook University Hospital (approval No. DKU 2017-09-003). The need for informed consent was waived by the board.
RESULTS
Demographic and clinical characteristics of subjects
Among the 631,418 subjects, 365,553 (57.9%) were male and 265,865 (42.1%) were female, while 560,968 (88.8%) were day workers and 70,450 (11.2%) were night shift workers. In the night shift workers, 53,840 (76.4%) were male and 16,610 (23.6%) were female.
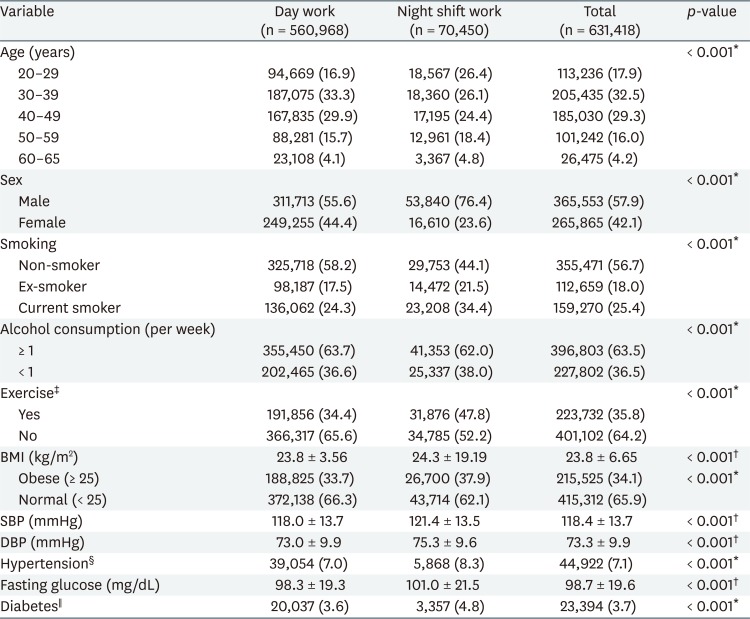
The day workers, with an average age of 40.1 ± 10.3 years, was significantly older than night shift workers, with an average age of 39.4 ± 11.7 years (p < 0.001). Among night shift workers, 34.4% were current smokers, which was significantly higher than that for day workers (24.3%) (p < 0.001). Obese subjects with BMI ≥ 25 kg/m2 comprised 37.9% of night shift workers, which was significantly higher than that of day workers (33.7%) (p < 0.001). A total of 223,732 subjects (35.8%) were health exercisers, of whom 31,876 (47.8%) were night shift workers and 191,856 (34.4%) were day workers; this difference was statistically significant (p < 0.001). The total number of alcohol drinkers was 396,803 (63.5%); among them, 41,353 (62.0%) were night shift workers and 355,450 (63.7%) were day workers; such difference was also statistically significant (p < 0.001).
For BP, the mean SBP was 118.0 ± 13.7 mmHg and the mean DBP was 73.0 ± 9.9 mmHg in day workers. The mean SBP was 121.4 ± 13.5 mmHg and the mean DBP was 75.3 ± 9.6 mmHg in night shift workers. Thus, SBP and DBP in night shift workers were significantly higher than day workers (p < 0.001). Fasting glucose level was 101.0 ± 21.5 mg/dL and 98.3±19.3 mg/dL, with the night shift workers having significantly higher than day workers (p < 0.001) (Table 1).
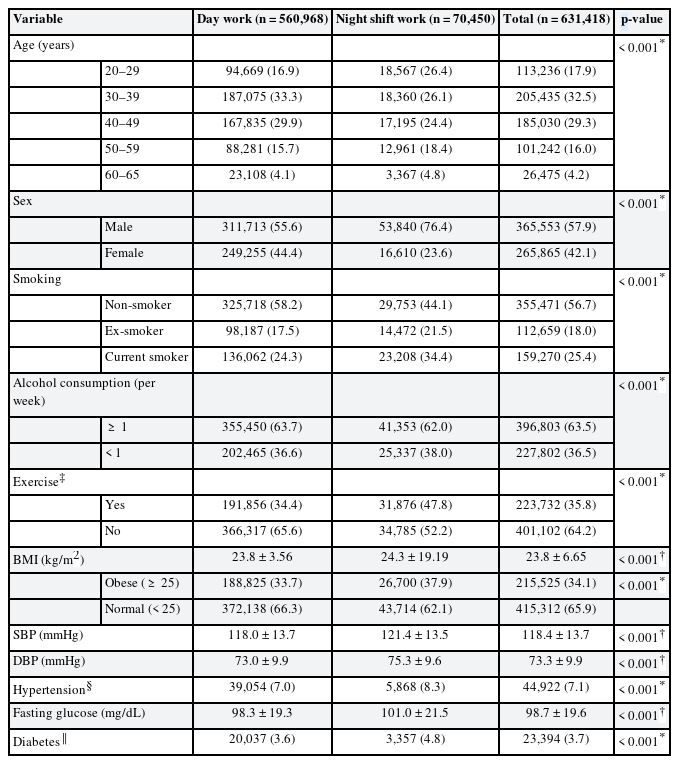
Demographic and clinical characteristics of subjects according to work type (n = 631,418)
Control rate of subjects taking antihypertensive and diabetes medication according to work type
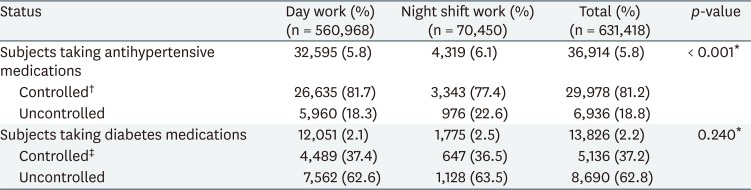
Among subjects 4,319 (6.1%) night shift workers and 32,595 (5.8%) day workers were taking antihypertensive medications. Among subjects 1,775 (2.5%) night shift workers and 12,051 (2.1%) day workers were taking diabetes medications.
The control rate of might shift workers taking antihypertensive medications was 77.4%, which was also significantly lower than 81.7% of day workers (p < 0.001). However, the control rate of subjects taking diabetes medications were not statistically significant (Table 2).
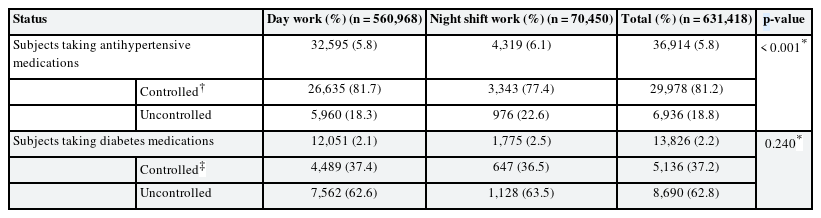
Comparison of control rates in subjects taking antihypertensive and diabetes medications
Control rate of subjects taking antihypertensive and diabetes medication according to work type and associated variables
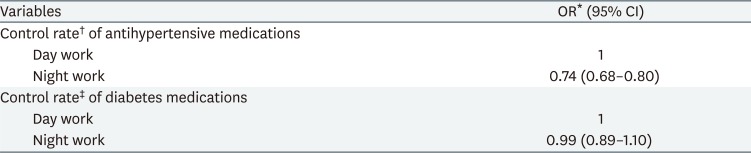
On multivariate logistic regression analysis, after adjusting for age, sex, smoking history, alcohol drinking, exercise, and obesity, the odds ratio (OR) of subjects taking antihypertensive medications among night workers was also 0.74 (95% confidence interval [CI]: 0.68–0.80) compared with day workers. In contrast, there were no statistically significant differences in the control rates of subjects taking diabetes medications between night workers and day workers (OR: 0.99, 95% CI: 0.89–1.10) (Table 3).
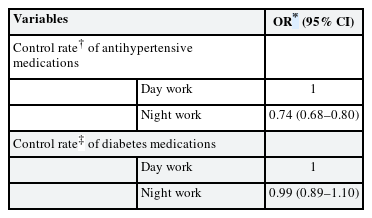
Multivariate analysis of variables affecting control rate of hypertension and diabetes
DISCUSSION
In this study, we found that when subjects were treated for hypertension, night workers had lower control rate of hypertension (OR: 0.74, 95% CI: 0.68-0.80) compared with day workers.
According to the 2017 Korean National Health and Nutrition Examination Survey, in the general population aged 30–65 years, the percentage of taking antihypertensive medication 6.7% and the control rate in people who received antihypertensive medications was 72.2% [22]. In our study, the subjects who answered that received antihypertensive medications among day workers was 5.8% and night shift workers was 6.1%, and the control rates in those who taking antihypertensive medication was 81.7% in day workers, 77.4% in night shift workers. Overall, the Korean National Health and Nutrition Examination Survey and our study do not show much difference, but some differences exist. Such differences may be due to lower average age of subjects as our study investigated including those who were under 29 years old, use of survey rather than health diagnostic processes such as laboratory data to determine prevalence rate, and mainly healthy worker effect [23].
Since most studies have focused on the association between shift work and hypertension or diabetes, very few studies are concerned with treatment control rates. Therefore, it is difficult to compare the results of previous studies with our research.
Suwazono and colleagues [24] also identified that shift work, including night work, is an independent risk factor of increased BP, and reported that work type had an important impact on the progression of hypertension more than age or obesity [25]. Similarly, in our study, we also found that night shift workers have a problem with controlling BP in patients who were treated for hypertension.
Shift work, including night work, can affect the patterns of activity and rest, resulting in changes in sleep and activity intervals and thus inducing sleep deprivation. Chronic sleep deprivation interferes with BP control by increasing BP and heart rate, increasing sympathetic nerve activity, and exacerbating physical and psychosocial stress as well as inducing water retention. Long-term exposure to these factors can bring about structural abnormalities such as left ventricular hypertrophy, ultimately causing difficulty in controlling hypertension [1026].
Research on the relation of shift work including night work and blood glucose control in patients with diabetes is limited. A study of 95 workers with diabetes found that shift work, including night work, did not affect blood glucose control [27]. A study of 32 workers also found no differences in glycated haemoglobin levels between day workers and shift workers, although the sample size was small [28]. However, Manodpitipong and colleagues [29] reported that shift workers, including night workers, had lower sleep time, higher BMI, and higher caloric consumption than day workers and that their average glycated haemoglobin level increased by about 5.9%. That is, if a non-shift worker's glycated haemoglobin was 7%, for example, shift workers including night workers would have a value of about 7.4%, indicating that shift work type, including night work, can make blood glucose control difficult. Sleep changes, lack of exercise, and failure to control diet can increase body fat quantity, leading to insulin resistance and increased weight, resulting in uncontrolled diabetes [30]. In our research, we found that night work did not have an independent effect on blood glucose control in patients with diabetes. However, the average blood glucose level of night workers was higher than that of day workers, and the number of obese workers with BMI ≥ 25 kg/m2 was also higher than that of day workers.
In this study, night workers had a lower rate of alcohol consumption, a higher rate of healthy-exercise, higher BMI, and a higher rate of obesity than day workers. But night workers had insufficient sleep time and lower quality of sleep, and shift workers, including night workers, have been shown to have higher BMI and obesity rates; such variables can be important risk factors for disease control [293031].
This research is significant as it was conducted in a large sample size-subject including night shift workers and it was performed on actual examinees after performing specific health examinations. But, there are some limitations to this study. First, factors such as impact by work type, differences in work duration, existence of health facility within the workplace, presence of an alternative welfare facility, and whether the examination was performed immediately after night work were not considered. Also, logistic regression analysis was used to control confounding variables without using stratification or restriction. The adjusted variables have limitations because they have not been classified in detail. Second, this study is a cross-sectional that we cannot infer any causal relationships. So prospective cohort study that addresses these limitations may be necessary in the future to further evaluate the impact of night work. Third, to more accurately assess, BP and blood sugar control, we recommend performing ambulatory BP monitoring or examining blood glucose control by glycated haemoglobin measurements. Fourth, since there may be selection biases or healthy worker effect in night shift workers, further analysis should be considered. Finally, we have not determined whether the medications were taken on the day of the examination, the duration of medication, the number and type of medications, the number of hospitals to visit, whether there was a recent hospital visit, and the interval between visits. Therefore, it will be necessary to revise the question items in this study and modify them to the actual examinee's specific health examination.
CONCLUSIONS
In conclusion, this study revealed that night work can have an effect on the uncontrolled BP in workers who are taking antihypertensive medications. Therefore, additional efforts for disease control are necessary for night workers with hypertension.
ACKNOWLEDGEMENTS
The research was supported by the Korea Medical Institute.
Notes
Funding: This research was funded by Korean Medical Institute's public offering for research purposes.
Competing interests: The authors declare that they have no competing interests.
Availability of data and materials: The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Author Contributions:
Conceptualization: Park J.
Data curation: Park J, Kang Y.
Formal analysis: Park J.
Funding acquisition: Shin SY.
Investigation: Shin SY.
Methodology: Park J, Rhie J.
Project administration: Park J, Rhie J.
Resources: Park J, Shin SY.
Supervision: Shin SY, Rhie J.
Writing - original draft: Park J.
Writing - review & editing: Park J, Kang Y, Rhie J.
Abbreviations
BP
blood pressure
BMI
body mass index
SBP
systolic blood pressure
DBP
diastolic blood pressure
CI
confidence intervals
OR
odds ratio