The association between dependent self-employment and self-reported depression/anxiety and sleep disorder in South Korea
Article information

Abstract
Background
Dependent self-employment is precarious employment, which can be vulnerable to mental health problems. This study aimed to investigate the association of dependent self-employment with depression, anxiety, and sleep disorder in South Korea.
Methods
This study used data from the Fourth Korean Working Conditions Survey and included 32,691 paid workers. Dependent self-employment and self-reported depression/anxiety, and sleep disorder were investigated using a questionnaire. Logistic regression analysis was performed to investigate the association between dependent self-employment and mental health problems.
Results
Of the 32,691 paid workers, 2,371 (7.3%) were dependent self-employed workers. The odds ratio (OR) of dependent self-employment for self-reported depression/anxiety was 1.78 (95% confidence interval [CI]: 1.29–2.45) and the OR of dependent self-employment for self-reported sleep disorder was 1.26 (95% CI: 1.01–1.59) compared to other paid workers.
Conclusions
Dependent self-employment is related to an increased risk of self-reported depression/anxiety and sleep disorder in South Korea.
BACKGROUND
The International Labour Office categorizes non-standard employment into 4 categories: 1) temporary employment; 2) part-time work; 3) temporary agency work and other forms of employment involving multiple parties; and 4) disguised employment relationships and dependent self-employment. Dependent self-employment refers to services that are performed for a business under a contract that is different from an employment contract. Such workers depend on one or a small number of clients for their income or receive detailed instructions regarding how the work is to be done [1]. Even though they provide labor like dependent workers, they are falsely classified as self-employed by employers in order to circumvent collective agreements, labor laws, employment taxes, and other liabilities implied in the standard contract of employment [2].
Typical dependent self-employment workers in South Korea include insurance salespersons, door to door delivery persons, and visiting teachers [34]. They make subcontracting agreements rather than employment contracts with employers. They personally find or receive customers to provide goods or services and receive performance allowances or incentives instead of fixed pay.
Dependent self-employed workers are not legally recognized to have employee status. Therefore, they are not guaranteed the rights and legal protections under the labor laws and collective agreements, receive less favorable benefits from social security protection, and are not entitled to labor unions or collective bargaining [56]. For this reason, they work in poor working environments compared with regular employees. Dependent self-employed workers have low job security [7] and work long or irregular hours to overcome their low and unstable income [4].
These risk factors such as job insecurity, long working hours and low or unstable income can cause a variety of health problems such as cardiovascular diseases [8910], mental health problems [1112131415161718], injury [1920], and sickness absence [21]. In particular, mental health problems are very common and important health issues in South Korea. An epidemiological study of Korean adults in 2016 reported that 13.2% of the population experienced one or more mental illnesses (not including alcohol and nicotine use disorders) [22]. Depression, anxiety, and sleep disorder are the most common mental illnesses, and the number of patients with such mental illnesses is steadily increasing every year. From 2013 to 2017, the number of patients experiencing depression increased from 591,000 to 680,000, anxiety disorders from 526,000 to 634,000, and sleep disorder from 381,000 to 515,000 [23]. Furthermore, mental and substance use disorders accounted for 6.2% of the total burden of disease of South Korea in 2012, and it was the seventh greatest burden of disease [24].
Based on these findings, it is assumed that dependent self-employed workers are at high risk of having mental health problems such as depression, anxiety, and sleep disorder. And, as growing prevalence of dependent self-employment, their working environment is becoming social issue [12]. Nevertheless, there has been no study on the association between dependent self-employment and these mental health problems. This study aimed i) to identify the characteristics and distribution of dependent self-employment in South Korea and ii) to investigate the association between dependent self-employment and depression/anxiety and sleep disorder.
METHODS
Study subjects
The Fourth Korean Working Conditions Survey (KWCS) was conducted in 2014 by the Korean Occupational Safety and Health Research Institute. The KWCS was designed to investigate overall working conditions including work type, employment type, occupation, business type, exposure to occupational hazards, and job security based on the European Working Conditions Survey and the Labor Force Survey in the United Kingdom. From June 1 to August 31, 2014, 50,007 employed workers aged 15 years or older across the country were extracted through multistage systematic cluster sampling and surveyed through one-to-one interviews by trained researchers who visited each household. Detailed information about the survey is available [25].
The subjects of this study were paid workers among the 50,007 participants in the Fourth KWCS. The KWCS classified dependent self-employed workers as paid workers. Self-employed workers with no employee, self-employed/employers with employees, unpaid family workers, and other workers were excluded from this study. Soldiers were excluded from this study. In addition, those who did not respond to any of the questions about the variables used in this study or did not answer or refused to answer were excluded from this study. The fourth KWCS provides a weight variable for their data to represent the working population across the country. The KWCS calculated the design weight based on the sample design and then adjusted the weight by applying the raking ratio method based on the "economically active population survey" conducted in 2014. The weight variable was applied for statistical analysis. Finally, 32,691 paid workers (18,883 male and 13,808 female) were included in the study.
Main variables
All variables were evaluated through questions. If the subject responded with “yes” to the following question, he or she was defined as a dependent self-employed worker: “Does your job correspond to a type of job that you personally find or receive customers to provide goods or service and earn as much as you work (depending on job performance)? Examples: insurance salespersons, visiting teachers, express delivery motorcycle riders, concrete engineers, etc.”
Mental health problems were assessed using the following question: “Did you have any of the following health problems during the past 12 months?” The sub-items of this question involved various health problems such as hearing problems, back pain, abdominal pain, cardiovascular disease, and injury. The subjects who reported having depression or an anxiety disorder and those who reported having insomnia or a sleep disorder were defined those who had a self-reported depression/anxiety and those who had a self-reported sleep disorder, respectively.
Covariates
The general and occupational factors of the subjects were selected as the covariates. The general factors included sex, age, education level, and monthly income. Age was classified as below 40, 40–49, 50 years or older. Education level was classified as below college graduate and college graduate or above. Monthly income was classified as less than KRW 1,300,000, KRW 1,300,000–1,990,000, KRW 2,000,000–2,990,000, and more than KRW 3,000,000.
The occupational factors included occupation, employment status, shift work, working hours per week, workplace scale, and occupational hazard exposure (physical, chemical/biological, and ergonomic exposure). Based on the Korean Standard Classification of Occupations (KSCO), occupation was divided into 3 groups: white-collar workers, service/sales workers, and blue-collar workers. Managers, professionals and related workers, and office workers were classified as white-collar workers, service workers and sales workers were classified as service/sales workers, and skilled agricultural, forestry and fishery workers, technicians and related technical workers, equipment and machinery operation and assembly workers, and simple laborers were classified as blue-collar workers. Employment status was classified into 2 groups: regular workers and temporary workers or daily employed workers. Working hours per week were classified as less than 40, 40–52, and 53 hours or more. The workplace scale was divided into two groups based on the number of current workers at each subject's workplace: less than 30 employees and more than 30 employees. Physical exposure was defined as exposure to at least one of the following for more than a quarter of working hours: vibration, noise, high temperature, and low temperature. Likewise, inhalation of smoke, fumes, dust, or vapor such as organic solvents or thinners; skin contact with chemicals or substances; exposure to secondhand smoke, wastes, or infectious substances such as body fluids and experimental substances for more than a quarter of working hours was defined as chemical/biological exposure. Assuming postures causing fatigue or pain, lifting or moving people, dragging, pushing or moving heavy objects; maintaining a standing posture; or having a repetitive hand or arm movements for more than more than a quarter of their working hours was defined as having ergonomic exposure.
Statistical analysis
A χ2 test was performed to compare the characteristics of the subjects according to status of dependent self-employment. Logistic regression analysis was used to estimate the odds ratios (ORs) and 95% confidence intervals (CIs) for self-reported depression/anxiety and sleep disorder. In Model 1, a simple binomial logistic regression analysis was performed. In Model 2, adjustments were made for sex, age, education level, and monthly income. In Model 3, adjustments were additionally made for occupation, employment status, shift work, working hours per week, workplace scale, and occupational hazard exposure. All statistical analyses were performed using SPSS (Statistical Package for the Social Science) for Windows version 23.0 (SPSS Inc., Chicago, IL, USA).
Ethics statement
This study was approved by the Institutional Review Board of Ajou University Hospital. (AJIRB-MED-EXP-19-036).
RESULTS
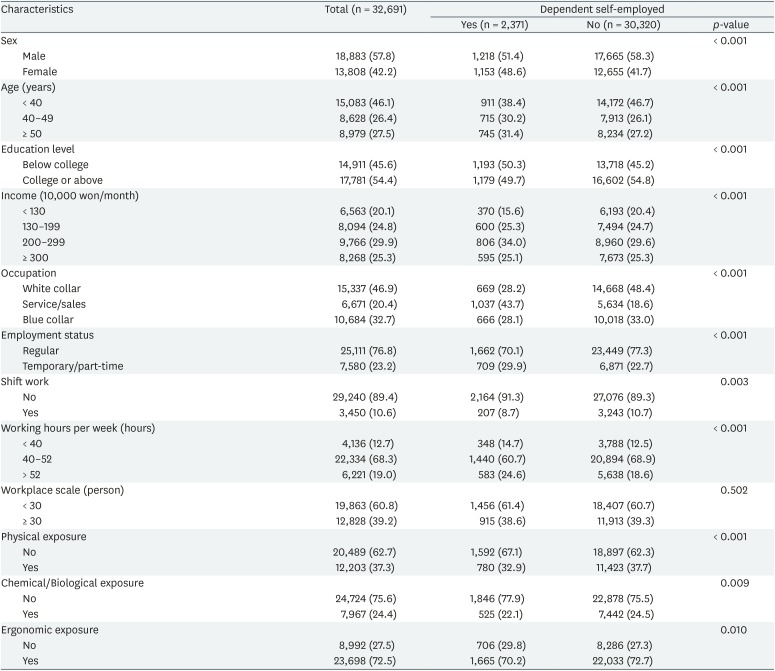
Of 32,691 subjects, 2,371 (7.3%) were dependent self-employed workers. Regarding the distribution of dependent self-employed workers, there were a similar number of male and female, 43.7% of workers were engaged in service and sales, and approximately one-third were temporary/part-time workers. Compared with paid workers (the control group) who were not dependent self-employed workers, dependent self-employed workers were less exposed to physical, biochemical, and ergonomic hazard (Table 1).
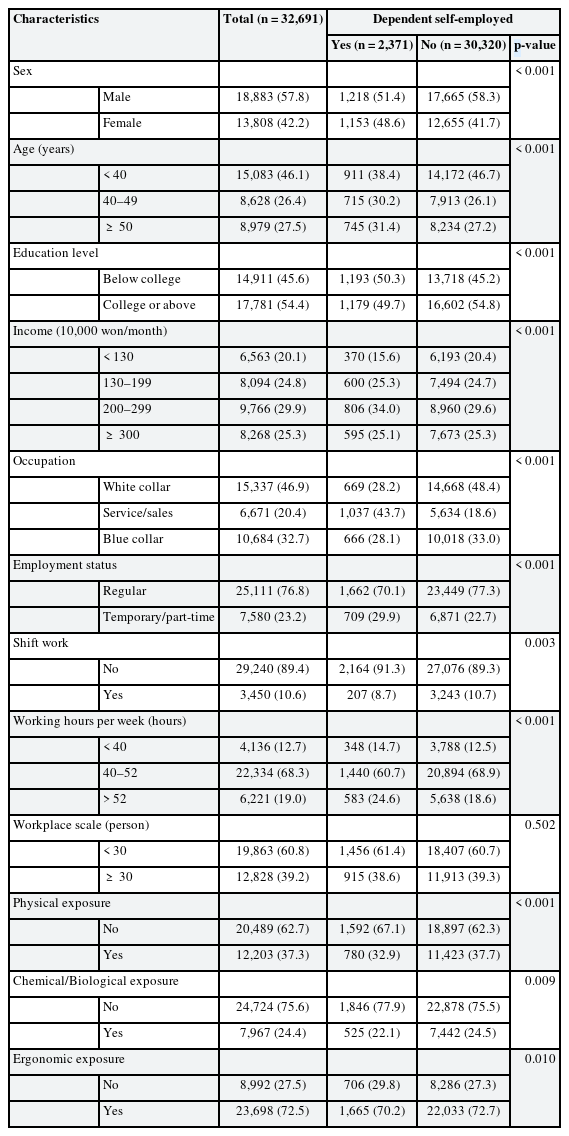
Characteristics of the study population according to dependent self-employment
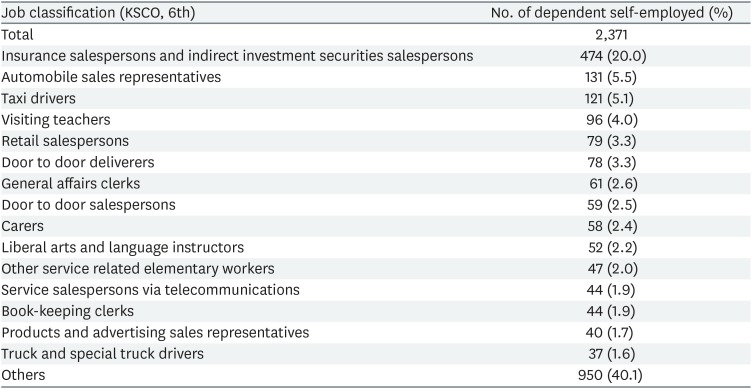
The KWCS classified the workers' occupations based on the Sixth KSCO. Table 2 lists the 15 occupations with the highest number of dependent self-employed workers in descending order. Of the 2,371 dependent self-employed workers, insurance salespersons and indirect investment securities salespersons accounted for 474, followed by automobile sales representatives, taxi drivers, and visiting teachers. (131, 121, and 96, respectively).
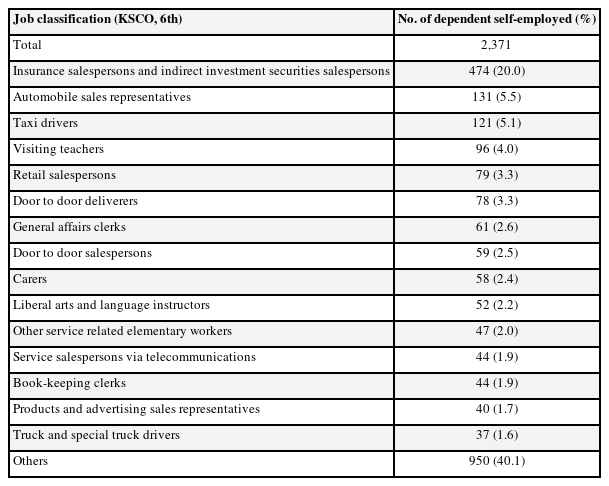
Typical occupations of dependent self-employment
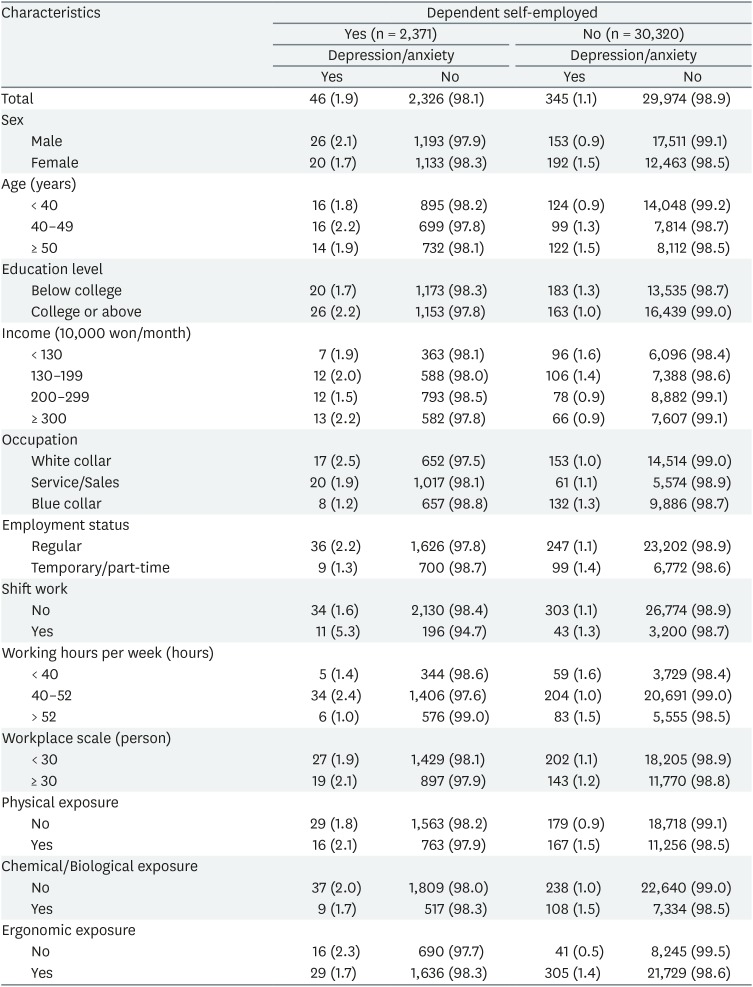
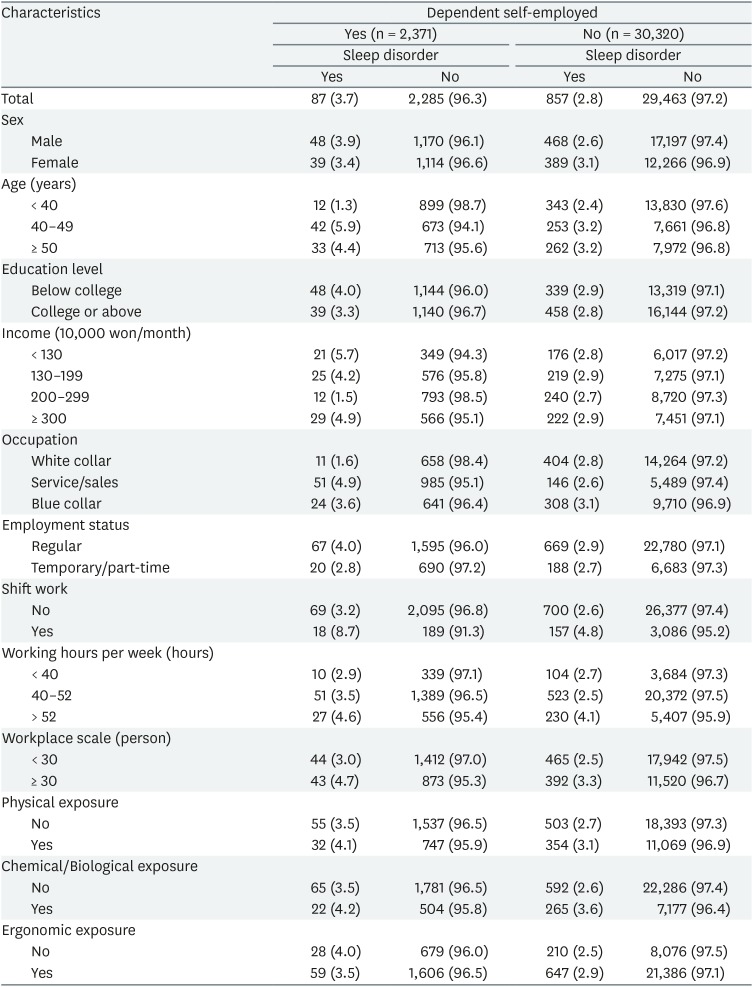
The prevalence of each mental health problem by subject's characteristics according to status of dependent self-employment is shown in Tables 3 and 4. Of 32,691 subjects, 391 (1.2%) reported having experienced depression or anxiety during the past 12 months. Of 2,371 dependent self-employed, 46 (1.9%) had self-reported depression/anxiety and 354 (1.1%) of the 30,320 controls had self-reported depression/anxiety. And, of 32,691 subjects, 994 (2.9%) reported having experienced insomnia or a sleep disorder during the past 12 months. Of 2,371 dependent self-employed, 87 (3.7%) had self-reported sleep disorder and 857 (2.8%) of the 30,320 controls had self-reported sleep disorder.
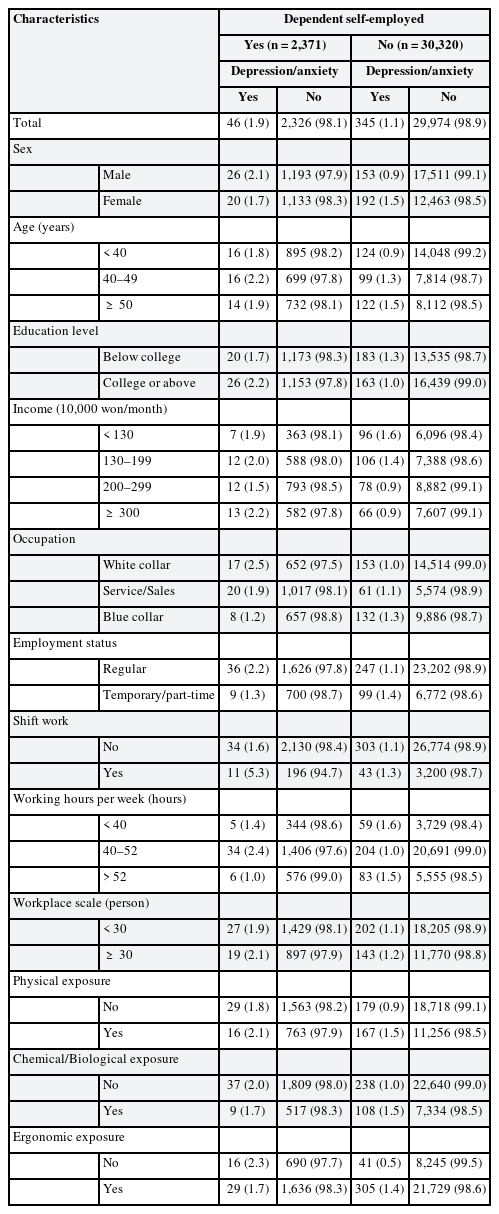
The prevalence of self-reported depression/anxiety according to characteristics of the study population
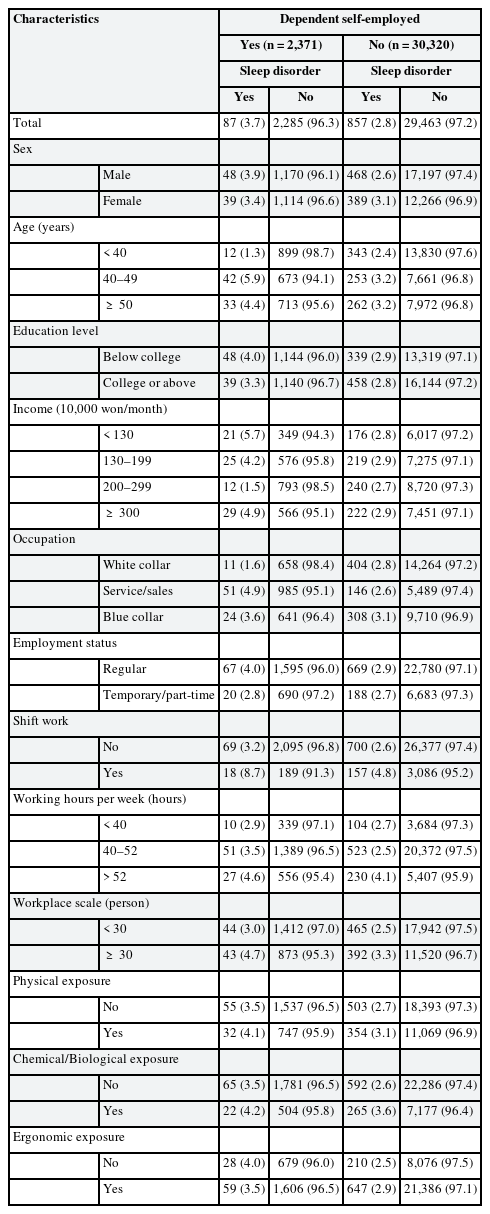
The prevalence of self-reported sleep disorder according to characteristics of the study population
The ORs and the 95% CIs of dependent self-employment for self-reported depression/anxiety and sleep disorder were calculated using multiple logistic regression analysis. Paid workers who were not dependent self-employed workers were used as the reference group. In Model 1 (crude model), the OR for self-reported depression/anxiety was 1.69 (95% CI: 1.24–2.31) and the OR for self-reported sleep disorder was 1.31 (95% CI: 1.05–1.64).
In Model 2, adjusted for age, sex, education level, and monthly income, the OR for self-reported depression/anxiety was 1.63 (95% CI: 1.18–2.23) and the OR for self-reported sleep disorder was 1.27 (95% CI: 1.01–1.60). In Model 3, additionally adjusted for occupation, employment status, shift work, working hours per week, workplace scale, and occupational hazard exposure (physical, chemical/biological, and ergonomic exposure), the OR for self-reported depression/anxiety was 1.78 (95% CI: 1.29–2.45) and the OR for self-reported sleep disorder was 1.26 (95% CI: 1.01–1.59) (Table 5).
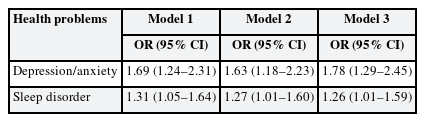
The ORs and 95% CIs for self-reported depression/anxiety and sleep disorder by dependent self-employment
DISCUSSION
The present study aimed to investigate the characteristics and distribution of dependent self-employed workers and the association between dependent self-employment and depression or anxiety and sleep disorder using a nationally representative sample of Korean workers. To our best knowledge, this is the first study to investigate mental health problems in dependent self-employed workers. The results of this study showed that dependent self-employment was positively associated with self-reported depression/anxiety and sleep disorder (OR: 1.78 and 1.26, respectively).
The analysis results of the Sixth European Working Conditions Survey in 2015 revealed that 4.3% of the total employment in 28 EU member countries was dependent self-employment [1]. In South Korea, approximately 500,000 (2.5%) of a total of 20 million workers were categorized their jobs as dependent self-employment [26].
In this study, the proportion of dependent self-employed workers was 7.3% of the total paid workers, which was higher than the proportion (2.5%) estimated by the National Statistics Office (NSO) in South Korea [26]. This big difference comes from the difference in survey method. The KWCS classified all the dependent self-employed workers as paid workers. On the other hand, the NSO first divided workers into paid workers and non-paid workers (e.g., self-employed) and subsequently surveyed paid workers for dependent self-employment. Dependent self-employed workers, who are in a vague boundary between dependent employment and self-employment, can regard themselves as self-employed workers. Therefore, because the research method used by the NSO did not include those who reported themselves as self-employed workers, the number of dependent self-employed workers was highly likely to be underestimated.
Unlike previous studies in the literature reporting that dependent self-employed workers had low wages [47], this study found that they did not have a lower monthly income than other paid workers. However, dependent self-employed workers are likely to use some of their income to perform their tasks. According to a report on the human rights situation of dependent self-employed workers issued in 2015 by the National Human Rights Commission of Korea [27], they often paid for the purchase, maintenance, and management costs of the equipment required for work. In particular, designated drivers and express delivery motorcycle riders were burdened with fuel and vehicle insurance costs. In many cases, they were responsible for losses incurred due to job-related accidents or mistakes. Given these points, actual available income of dependent self-employed workers is thought to be lower than the income superficially surveyed in the KWCS.
The Industrial Accident Compensation Insurance Act in South Korea defines dependent self-employed worker as persons who are not subject to the Labor Standards Act, etc., “regardless of the type of contract, even though they offer labor service similar to that of workers, and, therefore, need protection from occupational accidents, and who also meet all the following requirements: 1) they mainly provide one line of business with labor service necessary for the operation thereof on a routine basis, and receive payment for such service and live on such pay; 2) they do not use other persons to provide such labor service” [3]. However, despite the fact that dependent self-employment is actually distributed in a much wider variety of occupations [28], this Act limits the scope of dependent self-employment to nine occupations: insurance salespersons, concrete mixer truck drivers, visiting teachers, golf course caddies, door to door delivery persons, express delivery motorcycle riders, mortgage solicitors, credit card solicitors, and designated drivers.
In this study, dependent self-employed workers were distributed in various occupations in addition to the nine occupations designated by the Industrial Accident Compensation Insurance Act in South Korea. In particular, many dependent self-employed workers worked as automobile sales representatives, taxi drivers, retail salespersons, door to door salespersons, carers, service salespersons via telecommunications, book-keeping clerks, and product and advertising sales representatives. This finding supports the findings of previous studies claiming that the Industrial Accident Compensation Insurance Act does not adequately cover dependent self-employed workers in various occupations [42728].
According to the Survey of Mental Disorders in Korea in 2016, the one-year prevalence rate for mood disorders including major depressive disorders, dysthymia and bipolar disorder was 1.3%, and 1-year prevalence rate for anxiety disorders including generalized anxiety disorder, post-traumatic stress disorder and panic disorder was 5.7% in the general population of Korea [22]. However, in this study, the self-reported depression/anxiety was found to be 1.9%, and it was much lower than that of Korean general population. However, while the study population of Survey of Mental Disorders in Korea is the general adult population, current study targeted paid workers. Persons with mental health problems may have difficulty getting or maintaining a job [2930]. This healthy worker effects seem to have led to differences in the prevalence of depression/anxiety among paid workers and the general population of Korea.
To our knowledge, there was no previous study investigating the association between dependent self-employment and depression, anxiety, and sleep disorder. Meanwhile, many studies have reported that precarious employment, such as on-call work, subcontracted work, and temporary-help agency work, has a negative impact on mental health [313233]. Although there is no consensus on its definition, precarious employment can be usually seen as a type of employment characterized by employment insecurity, individualized bargaining relations between workers and employers, low wages and economic deprivation, limited workplace rights and social protection, and powerlessness to exercise workplace rights [34]. These characteristics have a negative impact on workers' mental health [31]. Dependent self-employment can be seen as precarious employment because it involves high employment instability [7], low wages [47], and limited workplace rights and social protection [56]. As such, it can be inferred that dependent self-employment, like other types of precarious employment, may also have a negative impact on mental health.
The results of this study showed that despite adjusting for occupational factors such as working hours and wages, dependent self-employment was associated with an increased risk of self-reported depression/anxiety and sleep disorder. One possible explanation for these results is a lack of legal protection. Dependent self-employed workers are typically not covered by the provisions of labour law or employment-based social security, and few countries have legal statutes governing this category of work [1]. In Korea, only the Industrial Accident Compensation Insurance Act covers them. This act says that the dependent self-employed need protection from occupational accidents because they are not subject to the labour laws [3]. Typical examples of these labor laws are the Labor Standards, which aims to guarantee and improve the basic living standards of workers by establishing standards for working conditions, and the Labor Union Act, which aims to guarantee the rights of association, collective bargaining, and collective action. The lack of protection from these labor laws could have put dependent self-employed workers in dangerous environment or poor mental working conditions.
For example, they may be disadvantaged owing to termination of a contract without reasonable cause or may be subjected to tyrannies that are not specified in their contracts, such as holiday work or unpaid education. Such a poor working environment can cause stress to workers, leading to mental health problems such as depression, anxiety, and sleep disorder.
Another possible explanation is job insecurity. Dependent self-employed workers have low job security [47]. In South Korea, there are many cases where a contract period is not specified, and even if a contract period is determined, such a contract period is often less than 1 year. In addition, because the contract termination and renewal procedures are not specified, contracts may be terminated arbitrarily, resulting in loss of employment [4]. Previous studies have shown that job insecurity was associated with depression, anxiety, and sleep disorder [15161718]. Having a premonition of losing their job or feeling that promotion is difficult may lead to emotions such as irritation, fear, and despair. These emotions can stimulate the stress response and induce the production of stress hormones such as epinephrine and cortisol, thereby promoting mental and physical arousal. In addition, continued emotional distress can lead to mental illnesses such as depression or anxiety [18]. Therefore, job insecurity resulting from dependent self-employment may play a major role in increasing the risk of depression, anxiety, and sleep disorder.
This study has several limitations. First, because it was a cross-sectional study, the causal relationship between dependent self-employment and mental health problems could not be identified, and the long-term effects of dependent self-employment could not be found. In view of the fact that reverse causation of mental health problems affecting employment status cannot be ruled out [35], further studies with a longitudinal design are needed in the future. Second, using a question to classify subjects into dependent self-employed workers and non-dependent self-employed workers may have resulted in misclassification. There are limitations in screening various types of dependent self-employment using a question. However, we believe that because well-trained researchers conducted the survey through individual interviews, such a misclassification issue could be minimized. Third, the validity of the diagnosis might be limited because in this study, depression/anxiety, and sleep disorder were diagnosed based on dichotomous questions as to whether or not they had experienced depression/anxiety or sleep disorder during the past 12 months. Further studies using medical records including proven diagnostic tools, hospital use, or drug use are needed. Finally, information such as drinking, smoking, caffeine intake, and medical history (especially mental illness) that could affect mental health problems could not be identified owing to the limitations of the data.
CONCLUSIONS
Dependent self-employed workers in South Korea had a high risk of self-reported depression/anxiety, and sleep disorder. Therefore, to reduce the risk of mental health problems among dependent self-employed workers, legal and institutional improvements are needed, such as recognizing them as workers or making exceptional provisions for them. Further studies with proven diagnostic tools and a longitudinal design are also needed in the future.
ACKNOWLEDGEMENTS
This study was conducted based on raw data from the 2014 Korean Working Conditions Survey, the fourth survey of the Occupational Safety.
Notes
Competing interests: The authors declare that they have no competing interests.
Availability of data and materials: The dataset is available in the Korea occupational safety and health agency (www.kosha.or.kr).
Author Contributions:
Conceptualization: Won G, Jeong I.
Data curation: Ha R.
Formal analysis: Won G, Lee S.
Investigation: Won G, Park JB, Lee KJ, Jeong I.
Writing - original draft: Won G.
Writing - review & editing: Won G, Park JB, Lee KJ, Ha R, Lee S, Jeong I.
Abbreviations
CI
confidence interval
KSCO
Korean Standard Classification of Occupations
KWCS
Korean Working Conditions Survey
NSO
National Statistics Office
OR
odds ratio